Open Journal of Radiology
Vol.2 No.4(2012), Article ID:25399,4 pages DOI:10.4236/ojrad.2012.24019
Non Traumatic Myositis Ossificans Mimicking a Malignant Neoplasm: A Case Report
1Rheumatology Department, CHU Hassan II Fes, Fes, Morocco
2Pathology Department, CHU Hassan II Fes, Fes, Morocco
3Radiology Department, CHU Hassan II Fes, Fes, Morocco
4Orthopedic Surgery Department, CHU Hassan II Fes, Fes, Morocco
Email: *latifatahiri@yahoo.fr, chbanil@yahoo.fr, sihamtizniti@yahoo.fr, traumajid@yahoo.fr, t_harzy@yahoo.fr
Received August 23, 2012; revised September 22, 2012; accepted October 6, 2012
Keywords: Myositis Ossificans; Magnetic Resonanace Imaging; Neoplasm; Pathology
ABSTRACT
Myositis ossificans is a benign self limiting condition that usually related to trauma. Despite a clinically and histologically distinct entity, myositis ossificans still causes considerable difficulties in diagnosis. A 33-year-old Moroccan woman presented with a 2-month history of left inguinal inflammatory pain with limping gait, MRI examination suggested a malignant neoplasm such as soft tissue osteosarcoma. A diagnosis of myositis ossificans was made by incisional biopsy. Conservative management with clinical and radiological follow up of 19 months confirm the diagnosis. The symptoms resolved within seven months. Myositis ossificans should be considered by clinicians as a possible diagnosis for a soft tissue lesion.
1. Introduction
Myositis ossificans is a benign, localized, self limiting ossifying soft tissue mass that occurs typically within the large muscles of the extremities [1]. It occurs usually in the second and third decades of life. Prior trauma is not necessary. Its presenting features can be similar to those of neoplasm, with the resultant potential for inappropriate initial management. We report a pseudomalignant myositis ossificans in a young woman.
2. Case Report
A 33-year-old Moroccan woman presented with a 2-month history of left inguinal inflammatory pain. She denied any specific trauma. Past medical history was unremarkable. Physical examination showed only motion pain and limping gait. Results of laboratory tests show a white cell count of 6700/mm3; erythrocyte sedimentation rate of 28 mm, C Reactive protein of 14 mg/l; calcium levels of 92 mg/l;
A left hip plain radiography (14/08/10) was normal. A magnetic resonance imaging (MRI) of pelvis (1/10/10) revealed a 40 × 35 mm mass near the left ilio psoas tendon. On T1 weighted and T2 weighted images, the mass showed hypointense and heterogenous hyperintense signals, respectively. After intravenous Gadolinium injection, the mass was enhanced significantly. Surrounding muscle edema was identified (Figure 1). Ultrasound imaging showed a soft tissue mass and increased vascularity. The possibility of a malignant neoplasm was proposed, and an incisional biopsy (12/10/10) was performed. Microscopically, the lesion was composed of a proliferation of fibroblasts in centre of the lesion with myxoid change admixed with foci of bone trabeculae lined by plump osteoblasts. Abnormal mitotic and nuclear pleomorphism were absent. These features were considered compatible with a diagnosis of myositis ossificans (Figure 2).
A Computed Tomography (CT) Scan (29/10/10) demonstrated peripheral ossification of the lesion, thus further confirming myositis ossificans. Conservative management with clinical and radiological follow-up of 19 months confirm the diagnosis (Figures 3 and 4). The symptoms resolved within seven months.
3. Discussion
The appearence of myositis ossificans (MO) on images varies, it correlates with the stage of the disease [2]. Plain radiographs are usually normal in the first few weeks but can show calcificatin 3 - 8 weeks after onset, starting peripherally and progressing centrally in a zonal pattern [3].
On MR imaging, early lesions are poorly defined and isointense on T1-weighted images, heterogeneously T2
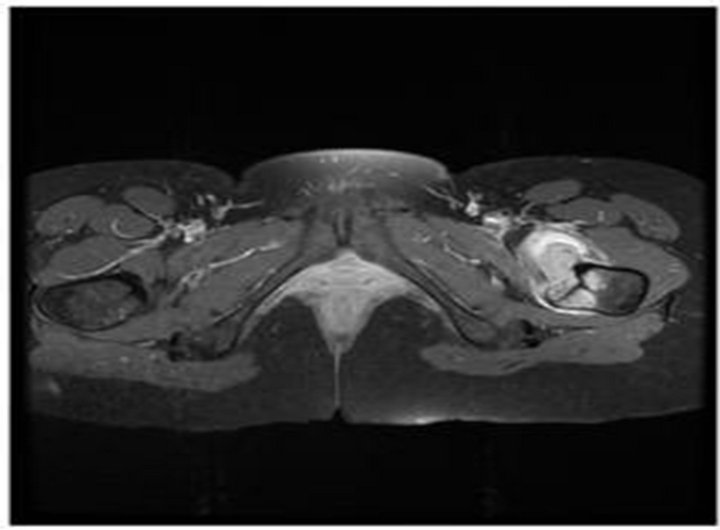
Figure 1. Axial T1 C+ MRI showing a heterogenous hyperintense mass with surrounding edema in the left femur.
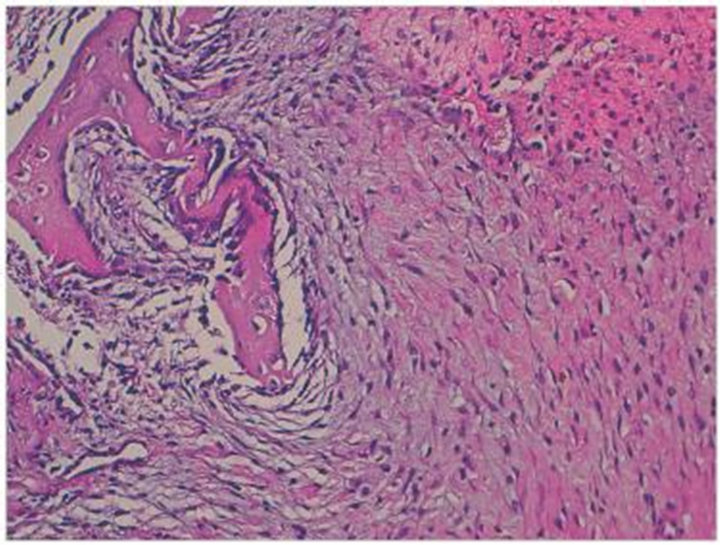
Figure 2. HESX100: Low power view showing zonation with myxoid change (centre) and bone formation at the periphery.
 (a)
(a)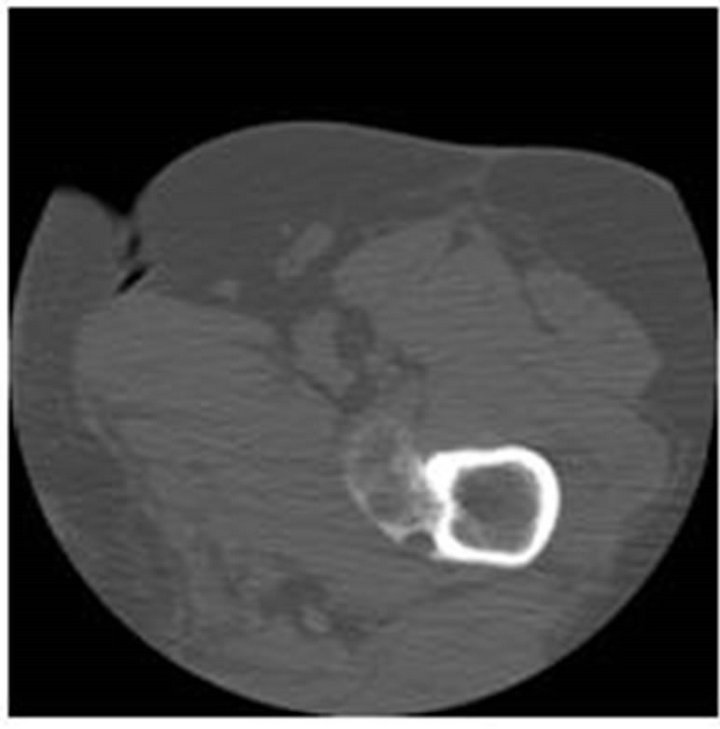 (b)
(b)
Figure 3. (a) Anteroposterior radiographof left femur showing a large ossified mass adjacent to the lesser trochanter 24/03/11; (b) Axial computed tomography (CT) image through the tigh showing the typical coarse peripheral calcification.
hyperintense, and have diffuse surrounding soft tissue edema [4]. Early stage MO can enhance and can be mistaken for soft tissue sarcoma, although the extensive muscle oedema associated with early MO is not a typical feature of soft tissue sarcoma [3]. Other lesions that can

Figure 4. Anteroposterior radiograph 02/04/12 of left femur showing a large ossified mass adjacent to the lesser trochanter.
have surrounding oedema include abscess, rhabdomyolysis and haematoma [5].
Moreover, areas of low signal intensity on MR images may not be recognized as calcifications or ossification, so it is important to consider MO in the differential diagnosis and to assess for the characteristic zonal pattern of mineralization on Radiographs or CT images [2]. CT is the most sensitive imaging method for detecting heterotopic mineralization, zoning phenomenon [6], it identify the typical patterns of this disease including the separation of the mass from the adjacent cortex and the decreased attenuation of the center of the mass [7]. MO is often confused with and must be distinguished from osteosarcoma, but pain and swelling in osteosarcoma are persistent and progressive [8] and cortical destruction is present on bone radiographs, with a neoplasia on histopathology. A malignant transformation of MO is possible but extremely rare [9] although several cases have been reported as secondary osteosarcoma arising from MO. Few of them are supported by histologic evidence [10].
MO is a self limiting condition and spontaneous resolution can occur. This more likely in smaller, upper extremity lesions than larger or lower limb lesions. Conservative management with clinical and radiological follow up may be sufficient when the lesion is typical. Surgical excision is indicated when lesions cause mechanical limitation, discomfort, or impingement on neural or vascular structures [11].
MO should be considered in the differential diagnosis with a soft tissue mass. In atypical cases a histopathological study is necessary to elucidate the diagnosis.
REFERENCES
- N. Crundwell, P. O’Donnell and A. Saifuddin, “Non-Neoplastic Conditions Presenting as Soft-Tissue Tumours,” Clinical Radiology, Vol. 62, No. 1, 2007, pp. 18-27. doi:10.1016/j.crad.2006.08.007
- J. S. Wu and M. G. Hochman, “Soft-Tissue Tumors and Tumorlike Lesions: A Systematic Imaging Approach,” Radiology, Vol. 253, No. 2, 2009, pp. 297-316. doi:10.1148/radiol.2532081199
- J. Parikh, H. Hyare and A. Saifuddin, “The Imaging Features of Post-Traumatic Myositis Ossificans, with Emphasis on MRI,” Clinical Radiology, Vol. 57, No. 12, 2002, pp. 1058-1066. doi:10.1053/crad.2002.1120
- S. Ehara, T. Nakasato, Y. Tamakawa, H. Yamataka, H. Murakami and M. Abe, “MRI of Myositis Ossificans Circumscripta,” Clinical Imaging, Vol. 15, No. 2, 1991, pp. 130-134. doi:10.1016/0899-7071(91)90162-O
- J. Nishio, K. Nabeshima, H. Iwasaki and M. Naito, “NonTraumatic Myositis Ossificans Mimicking a Malignant Neoplasm in an 83-Year-Old Woman: A Case Report,” Journal of Medical Case Reports, Vol. 12, No. 4, 2010, p. 270. doi:10.1186/1752-1947-4-270
- P. Tyler and A. Saifuddin, “The Imaging of Myositis Ossificans,” Seminars in Musculoskeletal Radiology, Vol. 14, No. 2, 2010, pp. 201-216. doi:10.1055/s-0030-1253161
- M. A. Amendola, G. M. Glazer, F. P. Agha, I. R. Francis, L. Weatherbee and W. Martel, “Myositis Ossificans Circumscripta: Computed Tomographic Diagnosis,” Radiology, Vol. 149, No. 3, 1983, pp. 775-779.
- A. E. Hendifar, D. Johnson and D. G. Arkfeld, “Myositis Ossificans: A Case Report,” Arthritis & Rheumatism, Vol. 53, No. 5, 2005, pp. 793-795. doi:10.1002/art.21456
- E. Konishi, K. Kusuzaki, H. Murata, Y. Tsuchihashi, J. W. Beabout and K. K. Unni, “Extraskeletal Osteosarcoma Arising in Myositis Ossificans,” Skeletal Radiology, Vol. 30, No. 1, 2001, pp. 39-43. doi:10.1007/s002560000298
- A. J. Aboulafia, F. Brooks, J. Piratzky and S. Weiss, “Osteosarcoma Arising from Heterotopic Ossification after an Electrical Burn. A Case Report,” The Journal of Bone & Joint Surgery, Vol. 81, No. 4, 1999, pp. 564-570.
- G. Hait, J. A. Boswick Jr. and N. H. Stone, “Heterotopic Bone Formation Secondary to Trauma (Myositis Ossificans Traumatica),” The Journal of Trauma, Vol. 10, No. 5, 1970, pp. 405-411. doi:10.1097/00005373-197005000-00005
NOTES
*Corresponding author.