Open Journal of Stomatology
Vol.2 No.1(2012), Article ID:18206,4 pages DOI:10.4236/ojst.2012.21002
A comparative evaluation of dentin caries removal with polymer bur and conventional burs—An in vitro study
![]()
Department of Conservative Dentistry and Endodontics, Chhatrapati Shahuji Maharaj Medical University, Lucknow, India
Email: *dr.vijay.shakya@gmail.com, ahanachandra@yahoo.com, crown_tikku@hotmail.com, promilarajesh@yahoo.co.in, rakeshanita10@yahoo.in
Received 27 November 2011; revised 29 December 2011; accepted 7 February 2012
Keywords: Polymer Bur (Smartprep); Carbide Bur & Diamond Points; Dentin Caries; PBS Buffer
ABSTRACT
Aim: To evaluate the comparative efficacy of Polymer bur (Smartprep) and Conventional burs (Carbide bur & Diamond Points) in selective Dentin caries removal. Materials and method: 15 freshly extracted carious human premolars and molars were selected for this study. These teeth were split in the center of carious lesion, in order to obtain two corresponding half. Thus 30 samples were prepared in this way. These were randomly divided in to 3 groups of 10 samples each. Group 1: The carious portion of these samples was excavated with the help of polymer bur Smartprep (SS White). Group 3: Prepared with Tungsten carbide round bur (No. 018). Group 3: Prepared with the help of Diamond points (No. 018). The period of time involved in this process is measured. After excavation of all carious lesions, a longitudinal section from mid most part of lesion was obtain with the help of diamond disc at slow speed. After staining with caries detector dye “Seek”, the sections were subjected to histological evaluation under stereomicroscope. The thickness of remaining caries is measured in more or less than 1 mm. Results: The difference in grading of remaining carious dentin between Polymer bur and Conventional burs were statistically nonsignificant, but Polymer bur taken more time in comparison to Conventional burs. Conclusion: Smartprep bur is more conservative in selectively dentin caries removal than Conventional burs but same time it is more time consuming than Conventional burs.
1. INTRODUCTION
The traditional treatment for carious lesions was outlined nearly “a century ago by G.V. Black”. This treatment consists of the removal of the carious lesion, including all demineralized dentin and unsupported enamel. Furthermore, the preparations are extended to include pits and fissures that may at some future date may become carious (extension for prevention). Finally, cavity preparation, according to Sir G.V. Black, requires the removal of tooth structure to prepare a specifically dictated outline form as well as an internal form that provide for mechanical retention of the restoration.
Adhering to these traditional guidelines will results in removal of sound tooth structure, however the net result is that the final preparation for a very limited carious lesion can involve extensive loss of healthy enamel and dentin.
The existence of two layers of carious dentin has been well reported in the literature [1,2].
In contemporary minimally invasive restorative dentistry, the primary aim is to remove only the outer layer of highly infected, denatured caries-infected dentin [1]. This facilitates the preservation of the inner layer of intact, bacteria-free remineralizable caries affected dentin and prevents disease progression [3].
Conversely, studies showed that the application of adhesive-sealed composite restorations to irreversibly infected dentin did not affect the clinical performance of restorations [4,5].
A novel, recently proposed, self-limiting concept in mechanical caries removalhas been brought to fruition by the introduction of a Polymer bur, (SmartPrep, SS White Burs, Inc., Lakewood, NJ, USA) [6].
The paddle-shaped bur has a unique flute design, and is constructed from a medical-grade polyether-ketoneketone (PEKK), with a particular hardness and wear re0 sistance that reportedly enable it to remove only the soft caries-infected dentin, leaving the caries-affected dentin intact, Utilized exclusively at low speed (500 - 800 rpm), the bur quickly dulls and vibrates when it encounters the more highly calcified caries-affected dentin.
Thus, the objective of this study “A comparative evaluation of dentin caries removal with polymer bur and conventional burs—an in-vitro study” was to evaluate the efficacy of the Polymer bur in removing only carious-infected dentin.
2. MATERIALS AND METHODS
15 Freshly extracted carious human premolars and molars were selected for this study.
The teeth having occlusal or cervical caries were selected and cracked or fractured teeth were discarded. The samples were stored in PBS buffer at pH 7.2. These specimens were used within a week for experiment.
The enamel was removed with the help of diamond disc. These teeth were split in the center of carious lesion using a carborundum disc at low speed, in order to obtain two corresponding half from each tooth. Thus 30 samples were prepared in this way for the experiment. These were randomly divided in to 3 groups of 10 samples each.
Group 1: Consisted of 10 samples. The carious portion of these samples was excavated with the help of Smartprep bur (SS White) at slow speed. During the excavation procedure there were no limitation to number of burs used, but the main aim was to remove all the carious portion of the sample.
Group 2: Samples was prepared with Tungsten carbide round bur (No. 018). Excavation criteria were same as in Group 1.
Group 3: Samples of this group were prepared with the help of Diamond points (No. 018). Excavation criteria were same as in Group 1.
The following parameters were use to assess the caries free status of dentin:
• Hardness on probing;
• Dentin colouration;
• Unique sound of uninfected dentin on probing (cri dentare).
The amount of time involved in this process is measured from starting of hand piece until the final probing for dentin hardness, with the help of stop watch [7].
After excavation of all carious lesion, a longitudinal section from mid most part of lesion was obtain with the help of diamond disc at slow speed.
2.1. Preparation of Samples for Staining
After that these sections were stained with the help of caries detector dye “Seek”. Staining of all sections was done separately.
2.2. Preparation of Samples for Histological Evaluation
After drying with the filter paper these sections were subjected to histological evaluation under stereomicroscope at 20× magnifications. Remaining caries appears as pink color after staining with the caries detector dye, is recorded for every section.
With the help of photomicrograph obtained on a background of graph paper which has the grading of 1 mm. The thickness of remaining caries is measured in more or less than 1 mm.
The period of time taken in caries removal for each group was also recorded. Collected data submitted for statistical analysis.
3. OBSERVATION AND RESULTS
Order of grading of remaining carious dentin is (in ascending order):
• 0 mm grading: Smartprep bur group < Diamond Points group < Carbide bur group.
• <1 mm grading: Carbide bur group < Diamond Points group < Smartprep bur group.
• >1 mm grading: Carbide bur group = Diamond Points group < Smartprep bur group.
The results of this study shows that difference in grading of remaining carious dentin between Smartprep and Conventional burs (Diamond and Carbide) after total excavation of samples were statistically insignificant.
Results of processing time were in following order: Processing time of Group 1 > Group 2 > Group 3 Time required for total excavation of caries was statistically higher in Smartprep bur (Group 1) when compared with Carbide bur (Group 2), and diamond point (Group 3), but the difference between Diamond point and Carbide bur groups was insignificant.
4. DISCUSSION
Conserving healthy tooth structure is a critical component of today’s restorative dentistry. This is especially important due to current adhesion technology linked with compatible cavity preparation design available to us. With traditional detection methods like explorer, magnification, spoon excavator, caries-detection dye, and round burs, active caries can be located, removed, and the tooth is restored. However, during this process, the clinician is challenged to discern the precise juncture of the carious dentin from healthy dentin. Precision cannot be achieved and questions remaining: When is “sound” dentin reached? How do these removal process impact dentinal tubules? Has maximum protection of sound tooth structure been achieved?
Traditionally, this was accomplished using rotary Carbide and Diamond points and spoon excavator hand cutting instrument, assessing the resultant surface with a dental explorer and continuing to excavate until it “feels as hard as sound dentin”. This procedure is somewhat imprecise because it is practically impossible to provide a clinical description of the boundary between infected and non infected dentin. Further, the traditional approach is not fundamentally conservative because it often results in cavity preparation that extends beyond the infected outer carious dentin layer into the non infected or lightly infected inner carious dentin or normal dentin [8].
When this relatively aggressive cutting tendency is combined with dentist’s goal of obtaining an excavated surface that feels normal, larger than necessary cavity preparations can be expected. Moreover, a drill on a high or low speed hand piece equally removes infected and uninfected dentin, resulting in excessive loss of healthy tooth structure [9]. Differences in the hardness, toughness, and resiliency of carious verses non carious dentin would at least partially determine the relative efficiency with which these tissues could be removed by any new mechanical means of caries excavation. Toughness and resiliency is not known for the various zones within the carious dentin lesion, and therefore have not been correlated with pathologic changes. However, the microhardness of carious dentin has been well studied and correlated with the pathology, providing a rational basis for developing a new selective mechanical device and method for caries excavation [10].
The hardness of sound dentin ranges from 54 to 65 KHN and carious dentin having hardness of 20 KHN or less. The hardness of Smartprep bur is 50 KHN, thus it remove only carious part of the dentin, and worn off when comes in the contact with healthy dentin.
Dentin caries dye staining of dentin collagen matrix, which corresponds by definition to the outer carious dentin, generally occurs at carious dentin hardness of 20 KHN or less [11]. The average hardness after removal of carious dentin with handheld spoon excavator is 23 KHN, leaving the average thickness of softened dentin of 0.7 mm, although this thickness can be more than a millimeter [6]. While it appears that there is a range of hardness values for the microbial front among the various lesion types, excavation of carious dentin to a KHN range of 5 to 20 would completely remove infected dentin in many lesions and adequately disinfects most chronic lesions.
Caries detector dye “Seek” (ultradent product inc. USA), was used to detect caries in sample specimens of this study. “Seek” is a glycol based dye, which stains outer carious dentin and spares affected dentin. It has been shown that dyes that were dispensed in higher molecular weight carriers exhibited reduced diffusion properties in porous tissues. Thus, caries detecting dyes prepared with higher molecular weight polypropylene glycols may prevent over-staining and excessive removal of caries-affected or sound dentin.
The sample teeth were stored in PBS buffer solution at pH 7.2. PBS buffer does not alter carious dentin. Other storage media such as alcohol, formalin, or glutaraldehyde may react to the dentin collagen structure and may leads to alter the hardening of the dentin. In contrast PBS buffer possesses a light antibacterial effect without changing the collagen structure of the dentin or denatured proteins [7].
Distribution of grading of remaining carious dentin (Table 1) shows that Group 1 (prepared with Smartprep bur) having 4 samples without any remaining carious dentin in comparison with Group 2 (prepared with Carbide bur) which having 8 samples without caries and Group 3 (prepared with Diamond Points) with 7 samples without caries.
Inter group comparison of grading of remaining carious dentin between Group 1 and Group 2 shows that 0 mm grading is higher in Group 2, <1 mm & >1 mm grading is higher in Group 1, and difference is Statistically insignificant (p = 0.1353).
When same criteria compares between Group 1 and Group 3, 0 mm grading is higher in Group 3, <1 mm & >1 mm grading is higher in Group 1. and the difference is statically non-significant; and between Group 2 and Group 2, 0 mm grading is higher in Group 2, <1 mm & >1 mm grading is higher in Group 3 but the difference is statistically non-significant (p = 0.23, non-significant).
By these observations recorded, we can comment that Smartprep bur is more conservative than Carbide and Diamond Points, because in this study it was noted that conventional bur have high probability of over preparation, therefore the concept of conservation of tooth structure does not fulfill by these burs.
The mean working time needed to complete caries removal with Polymer bur was 133.50 seconds, with Carbide bur it is 99.80 seconds, and with Diamond points it is 111.10 seconds (Table 2). Inter group comparison of
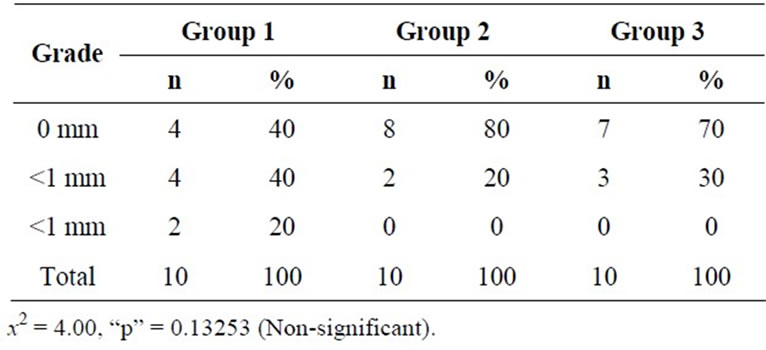
Table 1. Showing distribution of grading of remaining carious dentin in different groups.
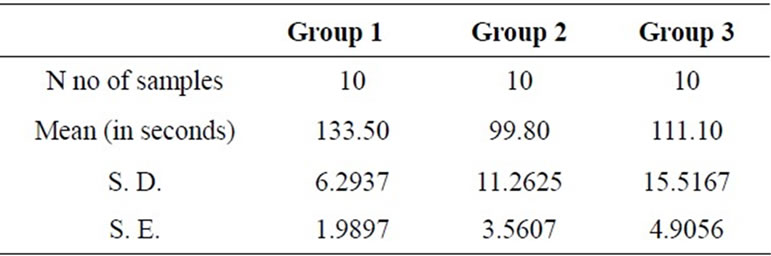
Table 2. Showing mean and standard deviation of processing time in the different groups.
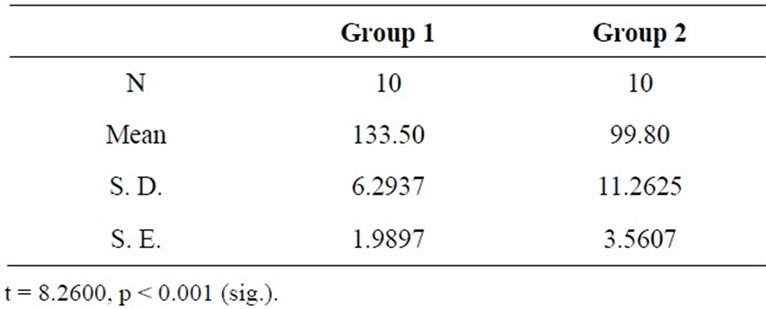
Table 3. Showing comparison of processing time in Group 1 & 2.
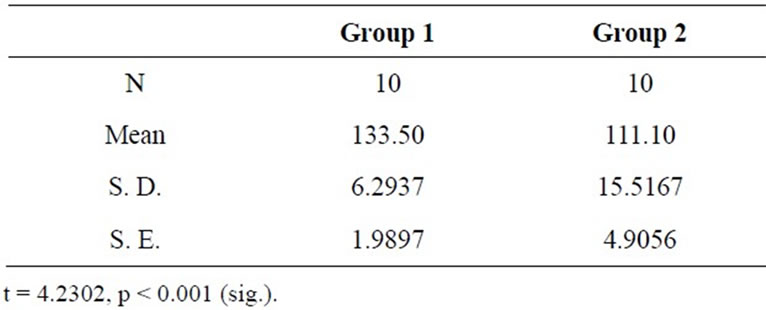
Table 4. Showing comparison of processing time in Group 1 & 3.
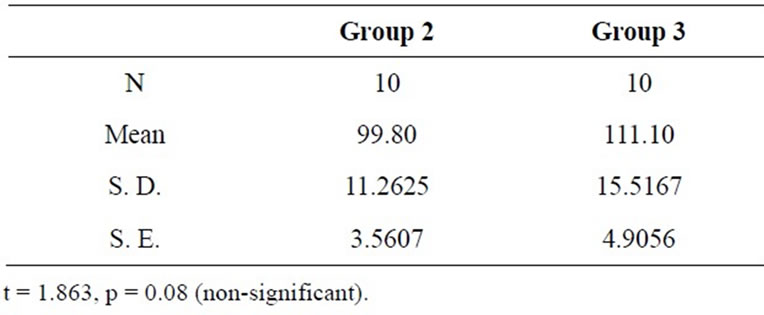
Table 5. Showing comparison of processing time in Group 2 & 3.
mean processing time shows that it is significantly higher (p < 0.001) in Group 1 than Group 2 & 3 (Tables 3, 4, 5).
The repetitive controls using the explorer determining dentin hardness and, the need to replace worn burs during the excavation procedure, was probably the main reasons for the mean time increase in the Smartprep bur group.
5. CONCLUSIONS
Based on the data of this study, it can be concluded that:
• The grading of remaining carious dentin is higher in Smartprep group than Diamond Points and Carbide bur group but the difference is statistically insignificant.
• The time required for complete excavation procedure is significantly higher in Smartprep bur group than Diamond points and Carbide bur group.
• Within the limits of this study, it may be concluded that although Smartprep bur is more time consuming than Conventional burs but at the same time it is more conservative in selectively removing carious dentin than conventional burs.
REFERENCES
- Massler, M. (1967) Changing concepts in the treatment of carious lesions. British Dental Journal, 123, 547-548.
- Fusayama, T. (1979) Two layers of carious dentin, diagnosis and treatment. Operative Dent, 4, 63-70.
- Wei, S.H., Kaqueller, J.C. and Massler, M. (1968) Remineralization of carious dentin. Journal of Dental Research, 47, 381-391. doi:10.1177/00220345680470030701
- Briley, J.B., Dove, S.B., Mertz-Fairhurst, E.J. and Hermesch, C.B. (1997) Computer-assisted densitometric image analysis of previously sealed carious teeth: A pilot study. Operative Dent, 22, 105-114.
- Ribeiro, C.C., Baratieri, L.N., Perdigão, J., Baratieri, N.M. and Ritter, A.V. (1999) A clinical, radiographic, and scanning electron microscopic evaluation of adhesive restorations on carious dentin in primary teeth. Quintessence International, 30, 591-599.
- Daniel, W. and Boston, D.M.D. (2004) New device for selective dentin caries removal. Quintessence International, Indian edition, 3, 40-47.
- Dammaschke, T., Rodenberg, T.N., Schafer, S. and Ott, K.H.R. (2006) Efficacy of the Polymer bur Smartprep compared with conventional Tungsten carbide bud bur in Dentin caries excavation. Operative dentistry, 31, 256-260. doi:10.2341/05-24 PMid:16827030
- Roberson, T.M., Sturdevants, C.M., Roberson, T.M., Heymann, H.O. and Swift, E.J. (2002) Sturevant’s art and science of operative dentistry. 4th Edition, Mosby, St. Louis.
- Banerjee, A., Kidd, E.A.M. and Watson, T.F. (2000) In vitro evaluation of five alternative methods of carious dentine excavation. Caries Research, 34, 144-150.
- Banerjee, A., Sherriff, M., Kidd, E.A.M. and Watson, T.F. (1999) A confocal microscopic study relating the autofluorescence of carious dentine to its microhardness. British Dental Journal, 187, 206-210.
- Yamada, T., Nakamura, K., Iwaku, M. and Fuseyama, T. (1983) The extent of the odontoblast process in normal and carious human dentin. Journal of Dental Research, 62, 798-802. doi:10.1177/00220345830620070401
NOTES
*Corresponding author.