Open Journal of Nursing
Vol.3 No.1(2013), Article ID:28702,8 pages DOI:10.4236/ojn.2013.31002
Factors that affect the process of professional identity formation in public health nurses
![]()
1Department of Human Health Sciences, Kyoto University Graduate School of Medicine, Kyoto, Japan
2School of Health Sciences, Faculty of Medicine, University of the Ryukyus, Nishihara, Japan
3School of Health Sciences, Sapporo Medical University, Sapporo, Japan
4Department of Site Management Organization, Sehma Co., Ltd., Fukui, Japan
5Faculty of Health Sciences, Hokkaido University, Sapporo, Japan
Email: okura.mika.2e@kyoto-u.ac.jp
Received 16 January 2013; revised 28 February 2013; accepted 4 March 2013
Keywords: Professional Identity; Public Health Nurse; Professionalism; Career Development
ABSTRACT
Objective: The aim of this study was to elucidate the process of professional identity formation and the factors that affect the process in public health nurses (PHNs). Methods: We performed an inductive qualitative analysis based on semi-structured interviews and focus group interviews of 65 PHNs. Results: At years 1 - 5, PHNs did not have a professional selfidentity. Therefore, it was important for them to recognize the significance of their own work. At years 6 - 10, PHNs acquired self-assurance as a practitioner through feedback from residents. It was important for them to have a better understanding, broader viewpoints and more affection for their own community. At years 11 - 20, PHNs felt ambivalent toward the challenges and heavy responsibilities based on the objective assessment of their jobs and roles. PHNs felt embarrassed by role changes when they became a manager or an expert. It was important for them to become aware of their new role through managerial education and training. However, some PHNs who were unable to establish a clear PHN identity experienced setbacks at each developmental stage. Conclusions: Our data suggest that a differential approach dependent on the stage and level of confidence in an individual’s PHN identity is required for the formation of PHN identity.
1. INTRODUCTION
In Japan, public health centers and local health centers have been established as activity centers for the promotion of health in local areas and the improvement of public health in each administrative division. In December 2008, 31,226 of 43,446 (72%) public health nurses (PHNs) were employed in prefectural and administrative organizations in the municipalities [1].
In recent years, changes in the work environment of PHNs have been accompanied by significant changes in the health care services offered by PHNs. First, community health needs are significantly changing as a result of the nationwide reformations of the health care system and diversification of the health care needs of local residents [2]. Second, the work environment has changed since the 1990s, when the number of workplace employees was decreased as a result of municipal mergers [1]. Third, there has been a sudden increase in the number of nursing care workers operating in communities. Fourth, there is a demand for workers to fill the new role of PHNs. Because regular personal services are increasingly offered by subcontractors, the role of PHNs as community health managers who are providing a needs-oriented service is becoming more and more important [2]. Fifth, there are demands related to the awareness of expectations and competencies of PHNs as specialists with a high level of knowledge and as generalists within their organizations [3].
In light of these changes in both the community and workplace environments, there are reports that it is not only difficult for PHNs to receive recognition of the significance and results of their work from bosses and other employees but also that it is difficult for them to derive pleasure and satisfaction from their work [4-6]. PHNs do not have a clear perception of the specialization of their field and thus experience a professional identity crisis.
If PHNs who do not have clear professional identities are working for residents to provide community care, their activities may not be effective. Therefore, at first, it is important to address how PHNs’ professional identities (PHN identity) are formed and what affects their identities.
Fagermoen [7] stated that professional identity refers to the actualization of the values of dignity, personhood, being a fellow human, and reciprocal trust, which depicts nursing as a human and moral practice concerned with providing personalized care to patients; that is, working as nurses maintains and enhances their self-concepts both as nurses and persons. Also, Gregg and Magilvy [8] has stated that “Bonding into nursing” was described as an initial substantive theory, which is defined as the process by which each nurse established her/his professional identity as a Japanese nurse. In other words, the establishment of a PHN’s identity is the source of energy that allows them to perform their health care services without fear of failure in an environment that demands a diversified and highly advanced role [9].
The purpose of this study was to describe how PHN identity is established over time, from the viewpoint of occupational development, and how PHN identity is affected. The results of this study can be used by PHNs to consciously envision their own careers and professional outlook. Furthermore, from an occupational development point of view, this study can be used as supporting data useful in planning more systematic ongoing education programs.
In this study, PHN identity indicates the meaning provided to the PHNs by their job; it is the psychological and social self-definition derived from receiving approval and positioning oneself in society as a result of fulfilling a social role through the specific occupation of PHN follow.
2. METHODS
2.1. Data Collection
We prepared an interview guide based on the Behavioural Event Interview (BEI) [10]. Most people do not always recognize their own abilities or strengths and weaknesses or are uncertain of whether they like their work. Most people do not always honestly describe their true motives or competencies at the time of an interview. The BEI style is based on the belief that hypothetical responses do not predict how a person will act in a future situation. We believed that this characteristic of the BEI was suitable for this study because we did not assume that most PHNs would be able to answer questions about PHN identity through straightforward questions.
The main contents of the interview were as follows: daily activities as a PHN, things about the job that provide a sense of satisfaction or are important, things considered typical of a person who becomes a PHN and their image of a PHN, and the importance in their lives of their job as a PHN. The subjects were asked to discuss approximately 4 - 6 important anecdotes from their past that were related to the practice of public health nursing.
2.2. Participants for Individual Interviews
We conducted personnel training workshops and semistructured interviews from the end of June 2003 to October 2005. There were 7 interviewers in charge of PHNs who had been working for 1 or 2 years and 1 interviewer for all other PHNs. All interviewers had previously conducted qualitative research, and several meetings were held before the actual interviews to ensure that the interviewers understood the intention of the interviews and questions. The subjects were 44 PHNs who gave consent for the interviews and were from 3 prefectures involved in a research project on human resource development.
2.3. Participants for Group Interviews
We held personnel training on investigative committee meetings and conducted focus group interviews from December 2008 to February 2010. The subjects were 21 PHNs who gave consent to participate in the interview and group discussion and worked in 2 prefectures that requested consultation on human resource development. In addition, the PHNs included in the group interviews were working in prefectures different from those who participated in the individual interview.
Participants were divided into groups of 7 to 9 people and were allocated based on whether their PHN experience was more or less than 10 years. Due to the small number of participants, we could not assign the participants based on their demographic characteristics.
2.4. Analysis Method
Using an inductive approach for qualitative data analysis based on the philosophy of the Grounded Theory method [11], we identified the smallest possible comprehensible unit related to PHN identity based on the episodes described by the PHNs. When we examined the encoded contents, no difference related to the interview method (individual interview or group interview) or the collected data that we used from 2003 to 2010 was found. Therefore, they were treated as equal data in the analysis. We gathered codes that had the same meaning in each stage and used these as the final codes from which we derived categories and subcategories. Throughout the data analysis, we continually performed comparative analyses and obtained demographics of the interviewees, such as affiliation organization, position, and years of work experience as a PHN.
To ensure the possibility of verification, we recorded how we obtained our results by maintaining records of the analytical process. To ensure reliability, we verified the results of this study and received the consent of 9 PHNs in stage 1 or stage 2 and 5 PHNs in stage 5.
2.5. Ethical Considerations
This study was conducted with the approval of the ethical committee of the Kanazawa University Graduate School of Medical Science. We provided both written and verbal explanations of this study to the interviewees. We explained that interviewees had the right to withdraw from the study even while it was in progress. We also confirmed that we guaranteed no professional demerits, protection of personal information by consolidated anonymity, and data storage on lockable shelves. In addition, we received consent for participation by asking the subjects to sign consent forms.
3. RESULTS
For the individual interviews, each subject was interviewed once, and the mean time for each interview was 58 ± 42 minutes (min-max; 30 - 180 minutes). For the group interviews, each group was interviewed for 2 - 7 sessions, with each session lasting 198 ± 43 minutes (mean ± SD, min-max; 120 - 240 minutes).
3.1. Participant Demographic Characteristics
A total of 65 subjects participated in the individual and group interviews. The mean age of the subjects was 33.8 ± 11.9 years (min-max; 22 - 59 years), and the mean work experience as a PHN was 10.8 ± 11.4 years (minmax; 1 - 37 years). Ten people worked at public health centers in a prefecture, 7 worked for designated or core cities, and 17 worked at smaller cities, towns or villages. Sixty-three PHNs were female, and 17 held the position of subsection chief or higher. Thirty-two PHNs had graduated from training schools or junior colleges, 30 from college, and 3 from graduate school. Other demographic details are shown in Table 1.
3.2. PHN Identity Formation through Each Stage of Development (Table 2)
By focusing on their duration of work experience, we found that PHN identity formation could be divided into the following 5 stages: 1st year, 2 - 5 years, 6 - 10 years, 11 - 20 years, 21 years or more/subsection chiefs and above. Each stage was defined based on the number of employed years. However, these stages were not clearly separated because it was not a linear process, and some people’s careers included both advances and setbacks. Furthermore, some PHNs employed for 21 years or more still did not have a definite identity.
3.2.1. Stage 1: Verifying Personal Significance before Becoming a PHN
The first year of work as a PHN was a time during which
Table 1. Participant demographic characteristics.
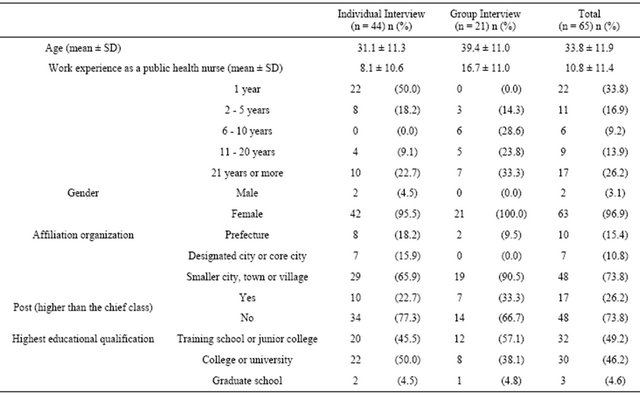
Table 2. PHN identity formation through each stage of development.

they understood nothing and were filled with anxiety. PHNs at this stage worked as hard as they could in a workplace filled with anxiety and stress in order to become a member of the organization where they worked before becoming a full-fledged PHN. In addition, their emotions varied between joy and sadness, and they worried about how others perceived them. They wanted to be accepted by the residents before they understood the residents. In other words, this stage was a time of verifying the significance of the sense of “independence” they had before they became full-fledged PHNs.
3.2.2. Stage 2: Borrowed PHN Identity
Years 2 - 5 of the PHNs’ careers were the years when they were impatient with their own immaturity because they compared themselves with senior PHNs who they considered as their role models. However, the episodes narrated by the subjects in this study did not show this process; the narrations lacked specific substantiation and explanations of the significance of their experiences. In other words, the advanced beginner stage was a time of borrowed PHN identity.
3.2.3. Stage 3: Confidence in PHN Identity as a Practitioner
Years 6 - 10 of the PHNs’ careers were the years when they gained adequate practical experience as a practitioner in charge of nursing care in their community. Furthermore, they were keenly aware of the reactions and responses of the residents and were proud of being a competent and professional worker. In other words, based on their experiences, this stage was a time when they obtained their self-confidence as a practitioner.
3.2.4. Stage 4: PHN Identity Becomes Unstable
Years 11 - 20 of the PHNs’ careers were the years when nurses experienced a crossroads between introspection and outlook, during which they looked back on their previous nursing care activities and thought about their future. Primarily because they could see the entire situation, they stood at a crossroads between reflection on the past and thoughts of the future. From this, they derived encouragement and felt a sense of great responsibility toward their duties. In other words, this stage was a time of unstable PHN identity during which they experienced a great deal of ambivalence.
3.2.5. Stage 5: Acting as a Manager or Expert with PHN Identity at the Core
PHNs at this stage were confused about their changes to managerial posts. In addition, even when they were not a manager, they undertook the role of a person in charge of community nursing care, which included guaranteeing the quality of services. In other words, the stage during which PHNs were in managerial positions or were pursuing professional expertise was a time when they were active in community nursing care management.
3.3. Different Levels of Confidence for PHN Identity (Figure 1)
In this section, we aimed to explore the process of PHN identity formation, including the level of confidence for PHN identity. We classified PHNs into three types de-

Figure 1. The arcs of public health nurse identity creation.
pending on the level of confidence for PHN identity: a typical type, an introspective-growth type, and a lack-ofconfidence type. In addition, the level of confidence for PHN identity was defined based on the subjective assessment of the interviewers. The interviewers evaluated how confident the interviewees answered the questions and how explicitly they could express what they thought. However, these types were not fixed to only one type and might be flexible for various reasons and triggers at any stage.
First, we describe a typical type in detail. PHNs in stage 1 were in the process of trying hard to adapt to their workplace before they had formed a PHN identity. Therefore, the confidence in the PHN identity was decreased compared to their basic education, when they lacked experience and had a poor image of PHNs. PHNs in stage 2 were envious of their senior co-workers and were impatient with themselves because they could not do their work well. At the same time, they began to be convinced of the importance of their work due to the reactions and responses of the residents as the subjects of community care. Therefore, their confidence started to rise. Then, in stage 3, they became proud of their work as PHNs. The confidence associated with PHN identity was highest in this stage. However, PHNs in stage 4 felt heavy responsibilities for their role and feared for their future. Therefore, their level of confidence was stable. When PHNs entered stage 5, they developed an upward trend. However, at this stage, they might experience a temporary drop because of the confusion about their role. We named this type as the typical type.
The introspective-growth type of PHNs had the following characteristics. They had higher confidence, a smaller drop and faster recovery than the typical-type PHNs. They strongly recognized the meaning of their work through self-contemplation and tended to strengthen their identity by considering the roles and beneficial functions of PHNs.
In contrast, the lack-of-confidence type had the following characteristics. They had lower confidence in all stages, many sways, and no stable state in their confidence levels.
3.4. Factors that Affect the Creation of PHN Identity (Table 3)
For PHNs in stages 1 and 2, the factors that affected PHN identity formation were the implications of their work. Introspection was promoted by following the advice from preceptors and senior PHNs and looking back on their daily work. They could overcome their confusion and worry by convincing themselves that their work was useful in their actual nursing activities. In addition, if they had a role model, it was easy for them to create their own image as a PHN.
In stage 3, a better understanding, broader point of view and more affection for their own community were
Table 3. The factors that affect the creation of PHN identity.
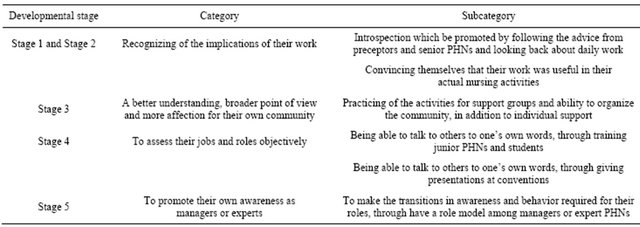
important for PHNs to create their identities. In addition to individual support, the activities for support groups and ability to organize the community made them expand their viewpoints. When they worked professionally, they increased their confidence as a PHN.
In stage 4, it was important for PHNs to assess their jobs and roles objectively. Through training junior PHNs and students and giving presentations at conventions, they could manage to overcome the period of low selfconfidence.
In stage 5, it was important for PHNs to promote their own awareness as a manager or an expert. If they had a role model as a manager or an expert, they had a tendency to make the transitions in awareness and behavior required for their roles.
4. DISCUSSION
4.1. Creation of PHN Identity and Influential Factors
The five stages identified by this study are similar to the following developmental stages described by Benner [12]: new beginner stage; advanced beginner stage; proficient, early stage; proficient, later stage; and expert/ manager stage.
4.1.1. Stages 1 and 2 (New Beginner Stage and Advanced Beginner Stage): To Have a Sense of Significance of One’s Own Work Including Introspection
The number of nursing universities is increasing rapidly in Japan, and the majority of the universities train students using an integrated curriculum that can include an examination of nurses’ and PHNs’ national qualifications. Because of the basic training provided using an integrated curriculum, PHN training has decreased in duration, resulting in a situation where a large number of PHNs start their job without forming a clear idea about their job [4,13]. It is very important to understand that this stage is a time when there are opportunities to continuously observe all facets of the job being performed by a preceptor [14,15]. A preceptor who can act as an advisor has great significance during the new beginner stage [16]. Furthermore, we can expect these PHNs to gain an understanding of the significance of their job experiences through the preceptor.
4.1.2. Stages 3 and 4 (Proficient, Early Stage and Proficient, Later Stage): To Be Able to View One’s Own Job and Role Objectively
The proficient stage is often cited as a time when PHNs lose their ability to assess their practical skills and their confidence [5,6]. However, this is not because of a lack of experience but because of careful consideration of how to provide better support and self-assessment of their judgments and actions [6]. In addition, if you think of the creation of PHN identity as a learning process, then the proficient later stage can be considered a “plateau” stage [17]. This plateau is a type of slump a nurse falls into after becoming independent. It happens almost without exception during an individual’s studies [17]. It is conceivable that being able to view their job and role objectively through training underlings leads to a trial and error process to gain insight and the ability to conceptualize their work. They will then be able to overcome their “plateau”.
4.1.3. Stage 5 (Expert/Manager Stage): To Find a “New” or “Modified” PHN Identity
The confusion resulting from the shift to a managerial position is not limited to PHNs. The ability to manage community nursing care, which is the area of expertise of PHNs, is demanded of PHNs even before they adopt a management position. Therefore, even if the practical skills are similar, PHNs may have difficulty accepting this transition. Thus, managerial education that promotes changes in the perception of their role is necessary.
Meanwhile, PHNs who do not want to become a manager or cannot be promoted to a managerial role should find a “new” or “modified” PHN identity that is not based on seniority [18]. Therefore, we expect that they will be more enthusiastic for their activities if they are shown how they should pursue the specialty for their career path more clearly.
4.2. Arc of the Creation of PHN Identity
The process of the creation of PHN identity was neither a linear nor step-by-step improvement. This is consistent with the idea that improvement does not result from having a single unambiguous core goal and that advancement does not occur linearly through skill acquisition [16].
The stages identified by this study correspond to the crossroads of career development described by Schien [19], looking back on past activities and looking forward to the future.
4.3. Study limitations and Future Prospects
This study was not intended to identify what the PHN identity should be. This study was a retrospective study. In addition, a wide variety in experiences as PHNs might have caused recall bias. Thus, the historical background of each developmental stage was not considered.
In addition, we could not explain why the three types of confidence in PHN identity developed, and it might be ascribed to personal characteristics or personal relationships at the workplace or the personnel training system. Furthermore, we could not quantify the types of confidence.
We cannot deny the possibility that the results of this study were biased by the predominantly female study population; gender may affect PHN occupational identity because most PHNs are females [20].
4.4. Conclusions
In this study, we clarified the stages divided by turning points in the development of PHN identify and differences in the levels of confidence that nurses have in their identity.
The results of this study show that the following are necessary: a close role model during the beginner stage, expectations to fulfill central practical roles and feedback that fosters confidence during the proficient stage, and managerial education that takes advantage of the identity of a PHN during the expert/manager stage.
5. ACKNOWLEDGEMENTS
We would like to express our heartfelt appreciation to all the PHNs who spared time from their busy schedules to participate in this study.
This study received funding from the Ministry of Health, Labour and Welfare; Grants-in-Aid for Health and Scientific Research Projects for fiscal years 2002-2004, and the Ministry of Education, Science, Culture, Sports, Science and Technology, Japan, Grants-in-Aid for Scientific Research Projects, Young Researchers for fiscal years 2007-2009.
This work was presented at the 68th Conference of the Japanese Society for Public Health and received an Excellent Subject Award.
![]()
![]()
REFERENCES
- Ministry of Health, Labour and Welfare (2008) National report of public health and hygiene administrative occupation. Ministry of Health, Labour and Welfare, Tokyo.
- Yoshioka, K.K. (2008) Strategies for assessing the feasibility to develop new needs-oriented services by public health nurses. Journal of Nursing Management, 16, 284- 290. doi:10.1111/j.1365-2834.2007.00782.x
- Saeki, K., Izumi, H., Uza, M., et al. (2007) Factors associated with the professional competencies of public health nurses employed by local government agencies in Japan. Public Health Nursing, 24, 449-457. doi:10.1111/j.1525-1446.2007.00655.x
- Okura, M., Saeki, K., Ohno, M., et al. (2005) The image of public health nurses held by public health nurses with 1 - 2 years of experience and their understanding of the job. Journal of Hokuriku Public Health, 32, 31-37.
- Okura, M., Saeki, K., Ohno, M., et al. (2004) The image of the public health nurse that beginner public health nurses have at the time of employment—The career choice motive and the image of the public health nurse. Journal of Tsuruma Health Science Medicine Kanazawa University, 28, 143-150. (in Japanese)
- Laperriere, H.N. (2008) Developing professional autonomy in advanced nursing practice: The critical analysis of sociopolitical variables. International Journal of Nursing Practice, 14, 391-397. doi:10.1111/j.1440-172X.2008.00700.x
- Fogermoen, M.S. (1997) Professional identity: Values embedded in meaningful nursing practice. Journal of Advanced Nursing, 25, 434-441. doi:10.1046/j.1365-2648.1997.1997025434.x
- Gregg, M.F. and Magilvy, J.K. (2001) Professional identity of Japanese nurses: Bonding into nursing. Nursing and Health Science, 3, 47-55. doi:10.1046/j.1442-2018.2001.00070.x
- Bernardino, E. and Felli, V.E. (2008) Knowledge and power necessary to reconstruct nursing after management changes at a teaching hospital. Revista Latino-Americana de Enfermagem, 16, 1032-1037. doi:10.1590/S0104-11692008000600015
- Spencer, M.L. and Spencer, M.S. (1993) How to perform a behavioral event interview (BEI): The development, introduction, creation and use of competency management. In: Competence at Work: Models for Superior Performance, John Wiley & Sons, Inc., New York, 114-134.
- Glaser, B.G. and Strauss, A.L. (1967) The discovery of grounded theory: Strategies for qualitative research. Aldine, Chicago.
- Benner, P.E. (2000) From novice to expert: Excellence and power in clinical nursing practice commemorative ed. Prentice Hall, Upper Saddle River.
- Dalton, L.M. (2004) Time as a source of conflict: Student nurse experiences of clinical practice in a rural setting. Rural Remote Health, 2, 1-10. http://rh.deakin.edu.au
- Adams, R. (2011) Exploring dual professional identities, the role of the nurse tutor in higher education in the UK: Role complexity and tensions. Journal of Advanced Nursing, 67, 884-892. doi:10.1111/j.1365-2648.2010.05519.x
- Zannini, L., Cattaneo, C., Brugnolli, A., et al. (2011) How do healthcare professionals perceive themselves after a mentoring programme? A qualitative study based on the reflective exercise of “writing a letter to yourself”. Journal of Advanced Nursing, 67, 1800-1810. doi:10.1111/j.1365-2648.2011.05615.x
- Lave, J. and Wenger, E. (1991) Situated learning: Legitimate peripheral participation. Cambridge University Press, Cambridge. doi:10.1017/CBO9780511815355
- Jiang, G., Chen, H., Wang, S., et al. (2011) Learning curves and long-term outcome of simulation-based thoracentesis training for medical students. BMC Medical Education. http://www.biomedcentral.com/1472-6920/11/39
- Evans, L. (2008) Professionalism, professionality and the development of education professionals. British Journal of Educational Studies, 56, 20-38. doi:10.1111/j.1467-8527.2007.00392.x
- Schien, E., Bechhard, R. and Bennis, W. (1978) Organization development. Addison-Wesley Publishing Company, Boston.
- Mizuno-Lewis, S. and McAllister, M. (2006) Taking leave from work: The impact of culture on Japanese female nurses. Journal of Clinical Nursing, 17, 274-281.