Open Journal of Preventive Medicine
Vol.05 No.02(2015), Article ID:53843,8 pages
10.4236/ojpm.2015.52005
Community-Based Screening and the Detection of Critical Carotid Artery Stenosis and Abdominal Aortic Aneurysm
Steven M. Weisman1, Nathalie I. Garbani2, Andrew J. Manganaro2
1Innovative Science Solutions, Morristown, USA
2Life Line Screening (LLS), Independence, USA
Email: weisman@innovativescience.net
Copyright © 2015 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 10 January 2015; accepted 3 February 2015; published 6 February 2015
ABSTRACT
Background: Community-based cardiovascular screening has the opportunity to detect critical cardiovascular disease and positively affect public health outcomes. Disease deemed to be critical or severe at detection requires appropriate medical follow-up. This article examined the self-reported outcomes of individuals who had undergone community-based cardiovascular screening and had critical findings for abdominal aortic aneurysm (AAA) or carotid artery stenosis (CAS). Methods: Over 390,000 screening records for AAA and over 490,000 screening records for CAS were reviewed to identify individuals with critical screening findings. A critical AAA is defined as an aneurysm ≥ 5cm and critical CAS is defined as a hemodynamically significant stenosis with recorded peak systolic velocities of ≥300 cm/s, in this population. Identified individuals were then contacted via phone and surveyed about the medical care they received after their screening. Results: Review of the screening records found a prevalence of critical AAA findings of 0.037% (146 participants) and critical CAS findings of 0.12% (579 participants). 61% of participants with critical findings were reached for follow-up from both groups. Over 96% of participants with critical AAA and over 92% of participants with critical CAS had some forms of medical follow-up. Conclusions: Community-based cardiovascular screening has the ability to detect critical levels of disease. Findings of critical disease in the reviewed population are similar to the findings from previously published studies. Importantly, medical treatment received by those who seek follow-up appears to be consistent with recommended treatment guidelines. Identification and management of critical disease represent meaningful public and individual health benefits and the possibility of cost-savings.
Keywords:
Cardiovascular, Screening, Carotid Artery Stenosis, Abdominal Aortic Aneursym

1. Introduction
Community-based cardiovascular screening represents a unique modality for detecting cardiovascular disease and improving public health. While early detection of disease is intuitively of benefit, the true impact is only realized with appropriate follow-up and care, when indicated. Imperative to improving outcomes with screening results, the screening findings must lead to appropriate follow-up; a screening that uncovers no findings should require no further medical follow-up while a screening that uncovers a serious medical condition may warrant medical follow-up and treatment through the appropriate treatment paradigm.
Life Line Screening is the leading provider of community-based preventive health screenings in the United States. Since its inception, the company has screened more than 8 million people and currently screens more than one million people every year at a variety of community-based test sites. Through this experience, it has identified serious health issues and has helped save thousands of lives. This article examined the self-reported outcomes of self-referred individuals who had been screened by Life Line Screening (LLS) and found to have results defined as “critical”.
2. Purpose
While the primary aim of screening for atherosclerotic disease is to identify nascent vascular disease at its earliest and non-critical stages so that it can be treated prior to becoming life-threatening; it is important to examine the outcomes for those whom critical disease was identified. Therefore, the goal of this research is to provide insights on the referral and management of patients following a cardiovascular screening that detects a serious cardiovascular condition, specifically a critical finding of carotid artery stenosis (CAS) or abdominal aortic aneurysm (AAA). The outcomes of these patients are compared to those whose condition was detected in the traditional medical setting.
3. Methods
3.1. Participants
Participants self-selected to receive screening services provided by Life Line Screening (LLS). LLS utilizes direct mail marketing, email and television advertising to promote their service offerings. Participants self-pay for the service.
Participants have been screened in all 48 contiguous states. As reviewed in the recent publication by Drs. Weisman and Manganaro, the total population of screened individuals are largely over the age of 50 (91.2%), includes slightly more women than men (63.3%), and is disproportionally Caucasian (87.8%) [1] . Despite these imbalances, the overall size of the population (more than 6 million screenings completed) allows for extrapolation to the American population as a whole.
At screening, individuals are notified that the results of their screenings may be utilized for research purposes. The authors of this paper had access solely to de-identified data to perform this review. This dataset meets the definition of “de-identified” as described in the CFR Title 45 Section 164.514. According to the HIPPA Privacy Rule, de-identified datasets are not considered Protected Health Information and can be released and used without further authorization (consent) or any further restrictions, including IRB review or approval.
3.2. Study Size
Participants in this study consist of individuals who underwent cardiovascular screening services between July 1st, 2013 and February 28th, 2014. Records were reviewed for 491,471 participants who underwent CAS screening and 396,163 participants who underwent AAA screening to identify individuals with critical findings. Participants who were identified as having critical results for either of these tests were immediately notified verbally at the screening site of the results following a rescreening by a second technologist to verify results. In addition, participants, while still at the screening site, were provide with a report of their finding, a critical release form, and were advised to follow-up with a physician within 24 hours.
This article presents the results of this chart review and self-reported subject follow-up only. As such, rigorous statistical analysis of this data was not conducted.
3.3. Measured Variables
LLS offers a range of cardiovascular and other health outcome screening services. Of relevance to this manuscript are the carotid duplex ultrasound assessment of CAS, using plaque visualization and peak systolic velocity (PSV) measurement, and abdominal ultrasound assessment of AAA which measured the diameter of the vessel from the outer wall to the other outer wall.
At screening, subjects also completed a questionnaire and provided self-reports of their age, smoking status, history of statin use, history of stroke, and prior diagnoses of COPD, atrial fibrillation, hypertension, high cholesterol or diabetes. Subjects also underwent a measurement of their body mass index.
LLS has conservatively defined CAS as noted in Table 1. Table 1 also provides definitions for “critical” findings in the traditional healthcare setting. A screening critical finding of AAA is defined as >5 cm. USPSTF defines AAA as present at 3.0 cm, small AAA as 3.0 - 3.9 cm, intermediate AAA as 4.0 - 5.4 cm, and a large AAA as 5.5 cm or greater [4] .
3.4. Follow-Up Survey
Subjects identified as having critical findings of CAS or AAA were contacted by LLS between one and six months following the initial screening. Subjects were contacted by phone and surveyed to learn more about what, if any, medical interventions were performed following the identification of either critical AAA or CAS. Three attempts to reach participants were made; participants were called at varying times during the day (morning―8 - 9 a.m., lunch time, and early evening―6 - 7 p.m.). Voicemails were left for participants when possible.
Participants successfully contacted were first asked whether they followed up with a physician, and if yes, what the outcome was (further tests, treatment, etc.). If subjects reported undergoing surgery, they were asked whether they had a stent (CAS), endograft (AAA) or open surgery.
4. Results
4.1. CAS
A review of 791,471 CAS screenings found 8012 abnormal CAS findings (1.01%), including 579 critical findings (0.073% of all screenings; 7.2% of abnormal findings). Of the critical findings, 314 were women (54%) and 265 were men (45%). Table 2 provides an overview of the characteristics of the participants with critical findings. Important to note is that almost 90% of participants with a critical finding were asymptomatic (no reported history of prior TIA or stroke).
355 participants with critical findings were reached for follow-up (61%). 180 participants reported undergoing carotid endarterectomy (CEA) (50.7%); 17 reported receiving a stent (4.78%); 129 had medical follow-up but had not received an intervention (36.3%); 20 participants had not received any follow-up yet (5.6%); 8 participants had chosen to have no follow-up (2.3%); and lastly, one participant was found to have died pre-opera- tively (0.28%). Table 3 provides a breakdown of follow-up/treatment status by gender and risk factor status.

Table 1. Definitions for “critical” findings of CAS.
aUSPSTF assigns an even broader definition to “severe CAS”, defining severe as 60% - 99% stenosis [3] . Abbreviations: CAS―carotid artery stenosis; PSBV―peak systolic velocity.
Table 2. Characteristics of participants with critical CAS findings.
aRisk factors include self-reported atrial fibrillation, hypertension, high cholesterol and diabetes. Abbreviations: BMI―body mass index; TIA―transient ischemic attack; CVA―cerebrovascular accident (stroke); Afib―atrial fibrillation.
Table 3. Results of follow-up survey for participants with critical CAS finding.
aRisk factors include self-reported atrial fibrillation, hypertension, high cholesterol and diabetes. Abbreviations: CEA―carotid endarterectomy.
4.2. AAA
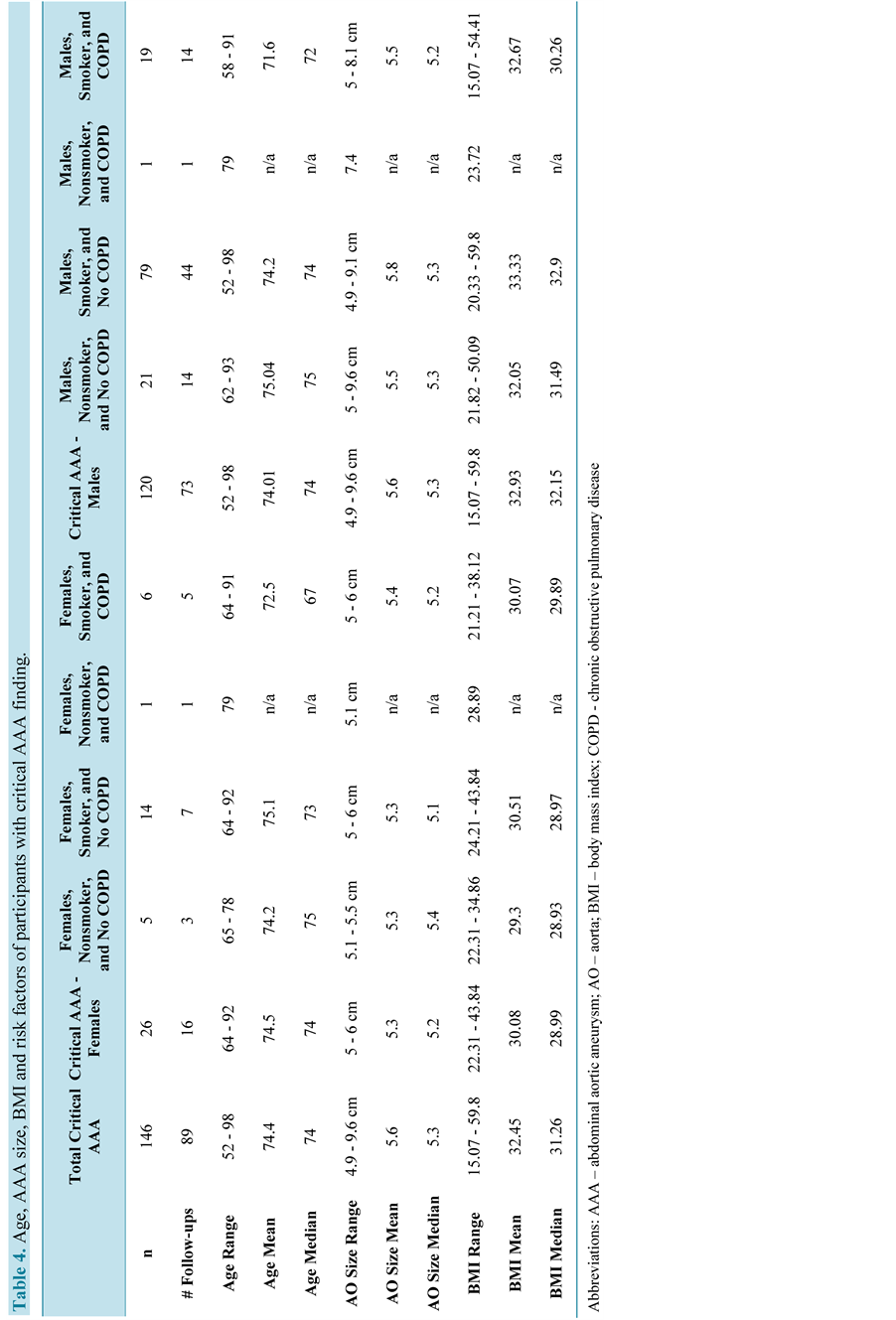
A review of 396,163 AAA screenings found a total of 2970 abnormal (AAA present but <5 cm) and critical findings (prevalence of 0.75%). 146 AAA were critical and represented 0.037% of all screened aorta and 5.2% of all aneurysms found. Of the 146 critical findings, 26 were in women (18%) and 120 were in men (82%). An overview of the 146 critical participants’ characteristics (age, AAA size, BMI, and smoking/COPD status) is shown in Table 4.
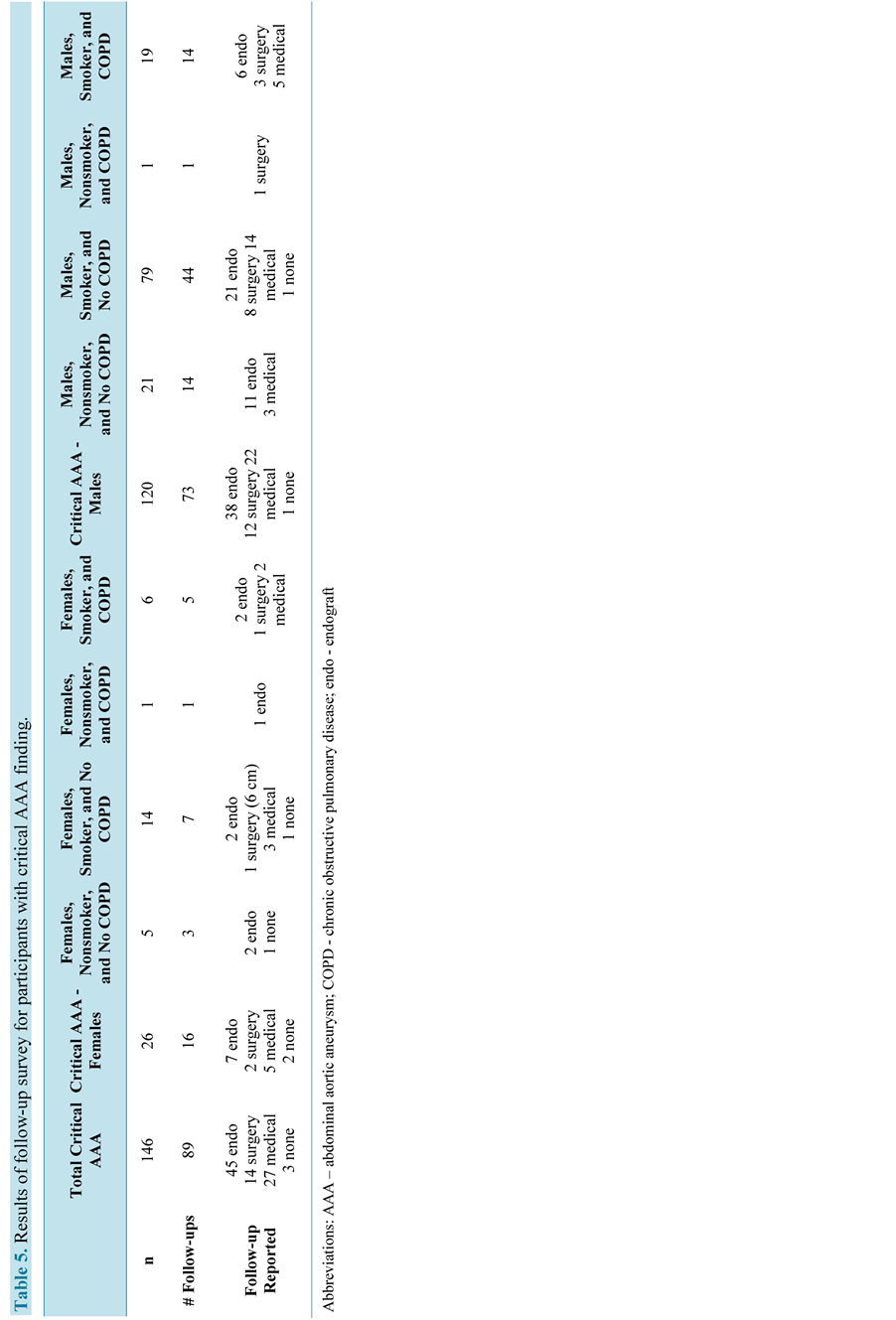
Of the 146 critical findings, 89 participants were reached for follow-up (61%). 45 participants reported endograft repair for their AAA (50.1%); 14 reported having open surgery for AAA resection (15.7%); 27 had sought medical follow-up, but had no intervention for AAA (30.3%); and 3 participants had not yet had any follow-up (3.34%). A breakdown of treatment/follow-up status by gender and smoking/COPD status is shown in Table 5.
5. Discussion
Based on this research, it is clear that community-based cardiovascular screening has the potential to detect significant disease that has otherwise gone undetected. Findings of critical disease are consistent with prior assessments of the prevalence of severe and critical CAS in the general population [5] [6] . This review found a prevalence of critical CAS of 0.073%. In a meta-analysis of 23,706 participants, de Weerd et al. found the prevalence of severe, asymptomatic CAS (defined as ≥70% stenosis) to range from 0% to 3.1% with increasing prevalence with age and in men [5] . A more recent study by de Weerd et al. found an even narrower prevalence of severe, asymptomatic CAS of 0.1% to 1.1% [6] . An earlier study by O’Leary et al. found a similar prevalence of severe CAS (defined as 100% stenosis) of 0.48% [7] .
Furthermore; the prevalence of critical CAS corresponds to the known impacts of risk factors such as high cholesterol, high blood pressure, diabetes, and family history [8] . In the development of a model for detecting occult carotid stenosis, Jacobwitz et al. demonstrated a significant increase in stenosis in the presence of increased risk factors (hypertension, cardiac disease, current smoking, and hypercholesterolemia) [8] . Our review demonstrated a similar increase (87/579 critical findings had no risk factors; 169/579 had one risk factor; and 323/579 had 2 or more risk factors).
In addition to detecting critical CAS, the follow-up survey provides preliminary evidence that individuals who follow-up with their physicians receive treatment in line with current treatment guidelines for their condition. The Society of Vascular Surgery (SVS) Guidelines for CAS recommends CEA as the first-line treatment for most symptomatic patients with stenosis of 50% - 99% and for asymptomatic patients with stenosis of 60% - 99% [9] . Out of subjects reached for follow-up, over half reported undergoing CEA (50.7%). Some stenting was reported (4.78%), which SVS guidelines recommend only for symptomatic patients with 50% - 99% stenosis who are at high risk for CEA.
Lastly, the SVS guidelines recommend that asymptomatic patients at high risk for intervention or with less than three years life expectancy should be considered for medical management only as first-line therapy. Out of all critical findings, 23% of participants were 80 years of age or older, and importantly almost 90% of participants self-reported as having no history of prior TIA or stroke (asymptomatic); with this demographic it appears reasonable that over one third of participants reached for follow-up reported only medical management.
Similar to CAS, critical findings of AAA are corroborated in part by prior studies of cardiovascular screening [10] - [12] . This study found a prevalence of critical AAA of 0.037% Greco et al. reviewed the results of over 3.1 million cardiovascular screening records and found a 0.077% prevalence of critical AAA [10] . Kent et al. reviewed a similarly sized dataset and found similar results of 0.073% critical AAAs (9.5% of all abnormal AAA results) [11] .
While the increased prevalence found in Greco and Kent may be attributable to their larger sample sizes; Lederele et al. screened 73,451 participants, compared to over 390,000 screened in this study, and found a prevalence of AAA ≥ 5.0 cm to be 1.09% [12] . This increase in prevalence may be due to the characteristics of the screened population which was disproportionally male (97%).
The course of treatment of AAA is not associated with a specific threshold of aneurysm diameter, although referral to a vascular specialist is indicated for aneurysms greater than 4.5 cm [13] . SVS and the Society for Vascular Medicine and Biology recommend individualized consideration of rupture risk, operative mortality, and life expectancy; but have also noted that based on currently available data, repair of aneurysms at 5.5 cm is the best benchmark. Guidelines further note that endovascular repair (endograft) is likely most beneficial for
older, high-risk patients, though the choice between endovascular repair and open surgery “relies heavily on patient preference” [13] .
Results of our medical follow-up data appear to mirror these recommendations. Noting that the population found to have critical AAA results at screening are generally older (mean age 74), it is unsurprising that that just over half of subjects reached underwent endovascular repair, while only 15% underwent open surgery. The 30% of participants who reported only medical follow-up may reflect participants who opted to forgo surgical intervention. These findings are strongly corroborated by a study that examined the results of several AAA screening trials and found that out of subjects who met the criteria for surgical intervention (AAA ranging from >5.0 cm to >6.0 cm), 39% - 67% of subjects actually underwent surgical repair [14] .
Importantly, these findings of critical AAA and CAS demonstrate that individuals who self-refer themselves to community based screening likely represent a “usual risk” population and are not, as many may have postulated, the “worried well” nor a population at higher risk due to being outside of the traditional medical system.
This study has a few limitations and ultimately presents the opportunity for further research into the outcomes of individuals who undergo community-based cardiovascular screening. First, as participants self-select and self-pay for screening, the population is subject to selection bias of an uncertain degree. Secondly, the risk factors reviewed in this report are self-reported and subject to potential errors in reporting. The largest limitation to this particular review is the almost 40% of individuals who were identified as having a critical AAA or CAS finding who were lost to follow-up. Lastly, the nature of the follow-up was not always consistent―occurring anywhere between one and six months post-screening, which may have resulted in errors in participant’s response to follow-up questions. Specifically, subjects followed-up at later time points may inaccurately report treatment received.
6. Conclusion
Cardiovascular screening identifies critical disease that may have been undetected. Early identification and management of these conditions yields meaningful public and individual health benefits. Importantly, screening participants who are identified as having critical conditions appear to receive appropriate medical care based on currently recognized treatment guidelines, indicating that had these findings been discovered during routine care or physician-recommended screening, the management and treatment would have likely been similar. Lastly, identification of critical disease presents potential cost savings. Participants treated for critical CAS may have costly strokes prevented; similar savings may be seen for AAA. While the cost-effectiveness of these types of screenings is debated, the identification and follow-up of critical findings may provide data for more robust analyses in the future.
Acknowledgements
Life Line Screening (LLS) provided the datasets used for this study, funded its research and writing, participated in study design, and had editorial input on the article’s content.
Conflict of Interest Statement
Dr. Steven Weisman is an independent scientific consultant that assists Life Line Screening (LLS) in its research efforts. Drs. Manganaro and Garbani are employees of Life Line Screening.
References
- Weisman, S.M. and Manganaro, A.J. (2013) Community-Based Screening: Identifying Risk and Motivating Healthy Lifestyle Changes. Postgraduate Medicine, 125. http://dx.doi.org/10.3810/pgm.2013.07.2675
- Chang, Y.J., Golby, A.J. and Albers, G.W. (1995) Detection of Carotid Stenosis. From NASCET Results to Clinical practice. Stroke, 26, 1325-1328. http://dx.doi.org/10.1161/01.STR.26.8.1325
- USA Preventive Services Task Force (2007) Screening for Carotid Artery Stenosis: USA Preventive Services Task Force Recommendation Statement. Annals of Internal Medicine, 147, 854-859. http://dx.doi.org/10.7326/0003-4819-147-12-200712180-00005
- USA Preventive Services Task Force (2005) Screening for Abdominal Aortic Aneurysm: Recommendation Statement. AHRQ Publication No. 05-0569-A.
- deWeerd, M., Greving, J.P., Hedblad, B., et al. (2010) Prevalence of Asymptomatic Carotid Artery Stenosis in the General Population: An Individual Participant Data Meta-Analysis. Stroke, 41, 1294-1297. http://dx.doi.org/10.1161/STROKEAHA.110.581058
- deWeerd, M., Greving, J.P., Hedblad, B., et al. (2014) Prediction of Asymptomatic Carotid Artery Stenosis in the General Population: Identification of High Risk Groups. Stroke, 45, 2366-2371. http://dx.doi.org/10.1161/STROKEAHA.114.005145
- O’Leary, D.H., Polak, J.F., Kronmal, R.A., Kittner, S.J., Bond, M.G., Wolfson Jr., S.K., et al. (1992) Distribution and Correlates of Sonographically Detected Carotid Artery Disease in the Cardiovascular Health Study. The CHS Collaborative Research Group. Stroke, 23, 1752-1760. http://dx.doi.org/10.1161/01.STR.23.12.1752
- Jacobowitz, G.R., Rockman, C.B., Gagne, P.J., et al. (2003) A Model for Predicting Occult Carotid Artery Stenosis: Screening Is Justified in a Selected Population. Journal of Vascular Surgery, 38, 705-709. http://dx.doi.org/10.1016/S0741-5214(03)00730-4
- Ricotta, J.J., Aburahma, A., Ascher, E., Eskandari, M., Faries, P. and Lal, B.K. (2011) Updated Society for Vascular Surgery Guidelines for Management of Extracranial Carotid Disease: Executive Summary. Journal of Vascular Surgery, 54, 832-836. http://dx.doi.org/10.1016/j.jvs.2011.07.004
- Greco, G., Egorova, N.N., Gelijns, A.C., et al. (2010) Development of a Novel Scoring Tool for the Identification of Large ≥ 5 cm Abdominal Aortic Aneurysms. Annals of Surgery, 252, 675-682.
- Kent, K.C., Zwolak, R.M., Egorova, N.N., et al. (2012) Analysis of Risk Factors for Abdominal Aortic Aneurysm in a Cohort of More than 3 Million Individuals. Journal of Vascular Surgery, 52, 539-548. http://dx.doi.org/10.1016/j.jvs.2010.05.090
- Lederle, F.A., Johnson, G.R., Wilson, S.E., Chute, E.P., Hye, R.J., Makaroun, M.S., et al. (2000) The Aneurysm Detection and Management Study Screening Program: Validation Cohort and Final Results. Aneurysm Detection and Management Veterans Affairs Cooperative Study Investigators. Archives of Internal Medicine, 160, 1425-1430. http://dx.doi.org/10.1001/archinte.160.10.1425
- Brewster, D.C., Cronenwett, J.L., Hallett Jr., J.W., Johnston, K.W., Krupski, W.C. and Matsumura, J.S., Joint Council of the American Association for Vascular Surgery and Society for Vascular Surgery (2003) Guidelines for the Treatment of Abdominal Aortic Aneurysms. Report of a Subcommittee of the Joint Council of the American Association for Vascular Surgery and Society for Vascular Surgery. Journal of Vascular Surgery, 37, 1106-1117. http://dx.doi.org/10.1067/mva.2003.363
- Silverstein, M.D., Pitts, S.R., Chaikof, E.L. and Ballard, D.J. (2005) Abdominal Aortic Aneurysm (AAA): Cost-Effec- tiveness of Screening, Surveillance of Intermediate-Sized AAA, and Management of Symptomatic AAA. Proceedings (Baylor University. Medical Center), 18, 345-367.