J. R. HALL ET AL.
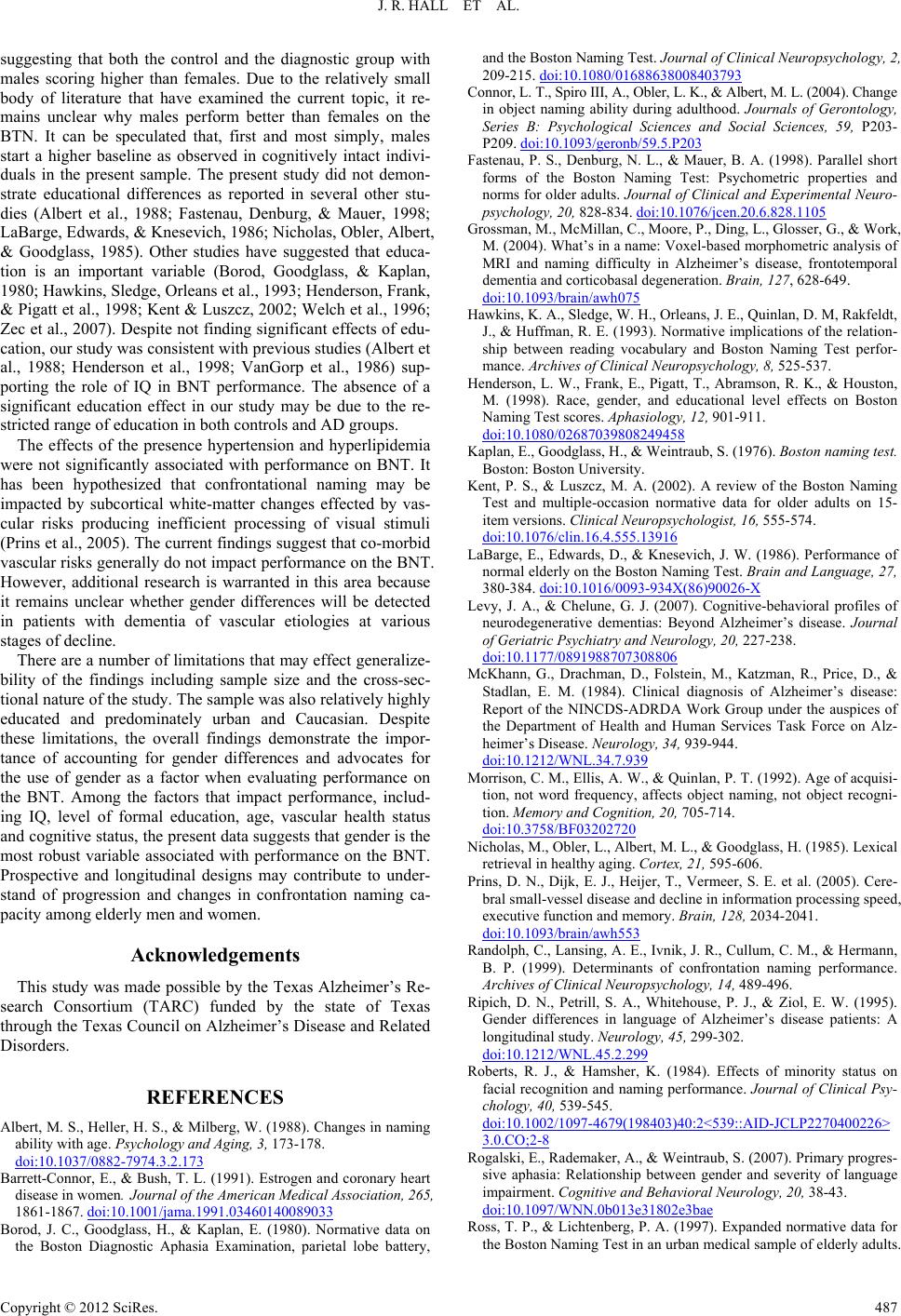
suggesting that both the control and the diagnostic group with
males scoring higher than females. Due to the relatively small
body of literature that have examined the current topic, it re-
mains unclear why males perform better than females on the
BTN. It can be speculated that, first and most simply, males
start a higher baseline as observed in cognitively intact indivi-
duals in the present sample. The present study did not demon-
strate educational differences as reported in several other stu-
dies (Albert et al., 1988; Fastenau, Denburg, & Mauer, 1998;
LaBarge, Edwards, & Knesevich, 1986; Nicholas, Obler, Albert,
& Goodglass, 1985). Other studies have suggested that educa-
tion is an important variable (Borod, Goodglass, & Kaplan,
1980; Hawkins, Sledge, Orleans et al., 1993; Henderson, Frank,
& Pigatt et al., 1998; Kent & Luszcz, 2002; Welch et al., 1996;
Zec et al., 2007). Despite not finding significant effects of edu-
cation, our study was consistent with previous studies (Albert et
al., 1988; Henderson et al., 1998; VanGorp et al., 1986) sup-
porting the role of IQ in BNT performance. The absence of a
significant education effect in our study may be due to the re-
stricted range of education in both controls and AD groups.
The effects of the presence hypertension and hyperlipidemia
were not significantly associated with performance on BNT. It
has been hypothesized that confrontational naming may be
impacted by subcortical white-matter changes effected by vas-
cular risks producing inefficient processing of visual stimuli
(Prins et al., 2005). The current findings suggest that co-morbid
vascular risks generally do not impact performance on the BNT.
However, additional research is warranted in this area because
it remains unclear whether gender differences will be detected
in patients with dementia of vascular etiologies at various
stages of decline.
There are a number of limitations that may effect generalize-
bility of the findings including sample size and the cross-sec-
tional nature of the study. The sample was also relatively highly
educated and predominately urban and Caucasian. Despite
these limitations, the overall findings demonstrate the impor-
tance of accounting for gender differences and advocates for
the use of gender as a factor when evaluating performance on
the BNT. Among the factors that impact performance, includ-
ing IQ, level of formal education, age, vascular health status
and cognitive status, the present data suggests that gender is the
most robust variable associated with performance on the BNT.
Prospective and longitudinal designs may contribute to under-
stand of progression and changes in confrontation naming ca-
pacity among elderly men and women.
Acknowledgements
This study was made possible by the Texas Alzheime r’s Re-
search Consortium (TARC) funded by the state of Texas
through the Texas Council on Alzheimer’s Disease and Related
Disorders.
REFERENCES
Albert, M. S., Heller, H. S., & Milberg, W. (1988). Changes in naming
ability with age. Psychology and Aging, 3, 173-178.
doi:10.1037/0882-7974.3.2.173
Barrett-Connor, E., & Bush, T. L. (1991). Estrogen and coronary heart
disease in women. Journal of the American Medical Association, 265,
1861-1867. doi:10.1001/jama.1991.03460140089033
Borod, J. C., Goodglass, H., & Kaplan, E. (1980). Normative data on
the Boston Diagnostic Aphasia Examination, parietal lobe battery,
and the Boston Naming Test. Journal of Clinical Neuropsychology, 2,
209-215. doi:10.1080/01688638008403793
Connor, L. T., Spiro III, A., Obler, L. K., & Albert, M. L. (2004). Change
in object naming ability during adulthood. Journals of Gerontology,
Series B: Psychological Sciences and Social Sciences, 59, P203-
P209. doi:10.1093/geronb/59.5.P203
Fastenau, P. S., Denburg, N. L., & Mauer, B. A. (1998). Parallel short
forms of the Boston Naming Test: Psychometric properties and
norms for older adults. Journal of Clinical and Experimental Neuro-
psychology, 20, 828-834. doi:10.1076/jcen.20.6.828.1105
Grossman, M., McMillan, C., Moore, P., Ding, L., Glosser, G., & Work,
M. (2004). What’s in a name: Voxel-based morphometric analysis of
MRI and naming difficulty in Alzheimer’s disease, frontotemporal
dementia and cor ticobasal degeneration. Brain, 127, 628-649.
doi:10.1093/brain/awh075
Hawkins, K. A., Sledge, W. H., Orleans, J. E., Quinlan, D. M, Rakfeldt,
J., & Huffman, R. E. (1993). Normative implications of the relation-
ship between reading vocabulary and Boston Naming Test perfor-
mance. Archives of Clinical Neuropsychology, 8, 525-537.
Henderson, L. W., Frank, E., Pigatt, T., Abramson, R. K., & Houston,
M. (1998). Race, gender, and educational level effects on Boston
Naming Test scores. Aphasiology, 12, 901-911.
doi:10.1080/02687039808249458
Kaplan, E., Goodglass, H., & Weintraub, S. (1976). Boston naming test.
Boston: Boston Univer si ty.
Kent, P. S., & Luszcz, M. A. (2002). A review of the Boston Naming
Test and multiple-occasion normative data for older adults on 15-
item versions. Clinical Neuropsychologist, 16 , 555-574.
doi:10.1076/clin.16.4.555.13916
LaBarge, E., Edwards, D., & Knesevich, J. W. (1986). Performance of
normal elderly on the Boston Naming Test. Brain and Language, 27,
380-384. doi:10.1016/0093-934X(86)90026-X
Levy, J. A., & Chelune, G. J. (2007). Cognitive-behavioral profiles of
neurodegenerative dementias: Beyond Alzheimer’s disease. Journal
of Geriatric Psychiatry and Neurology, 20, 227-238.
doi:10.1177/0891988707308806
McKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., &
Stadlan, E. M. (1984). Clinical diagnosis of Alzheimer’s disease:
Report of the NINCDS-ADRDA Work Group under the auspices of
the Department of Health and Human Services Task Force on Alz-
heimer’s Disease. Neurology, 34, 939-944.
doi:10.1212/WNL.34.7.939
Morrison, C. M., Ellis, A. W., & Quin lan, P. T. (1992). Age of acquisi-
tion, not word frequency, affects object naming, not object recogni-
tion. Memory and Cogniti on, 20, 705-714.
doi:10.3758/BF03202720
Nicholas, M., Obler, L., Albert, M. L., & Goodglass, H. (1985). Lexical
retrieval in healthy agin g. Cortex, 21, 595-606.
Prins, D. N., Dijk, E. J., Heijer, T., Vermeer, S. E. et al. (2005). Cere-
bral small-vessel disease and decline in information processing speed,
executive function and memory. Brain, 128, 2034-2041.
doi:10.1093/brain/awh553
Randolph, C., Lansing, A. E., Ivnik, J. R., Cullum, C. M., & Hermann,
B. P. (1999). Determinants of confrontation naming performance.
Archives of Clinical Neuropsychology, 14, 489-496.
Ripich, D. N., Petrill, S. A., Whitehouse, P. J., & Ziol, E. W. (1995).
Gender differences in language of Alzheimer’s disease patients: A
longitudinal study. Neurology, 45, 299-302.
doi:10.1212/WNL.45.2.299
Roberts, R. J., & Hamsher, K. (1984). Effects of minority status on
facial recognition and naming performance. Journal of Clinical Psy-
chology, 40, 539-545.
doi:10.1002/1097-4679(198403)40:2<539::AID-JCLP2270400226>
3.0.CO;2-8
Rogalski, E., Rademaker, A., & Weintraub, S. (2007). Primary progres-
sive aphasia: Relationship between gender and severity of language
impairment. Cognitive and Behavioral Neurology, 20, 38-43.
doi:10.1097/WNN.0b013e31802e3bae
Ross, T. P., & Lichtenberg, P. A. (1997). Expanded normative data for
the Boston Naming Test in an urban medical sample of elderly adults.
Copyright © 2012 SciRes. 487