Severe Diffuse Lamellar Keratitis Following Laser in Situ Keratomileusis with an Iatrogenic Double Flap 35
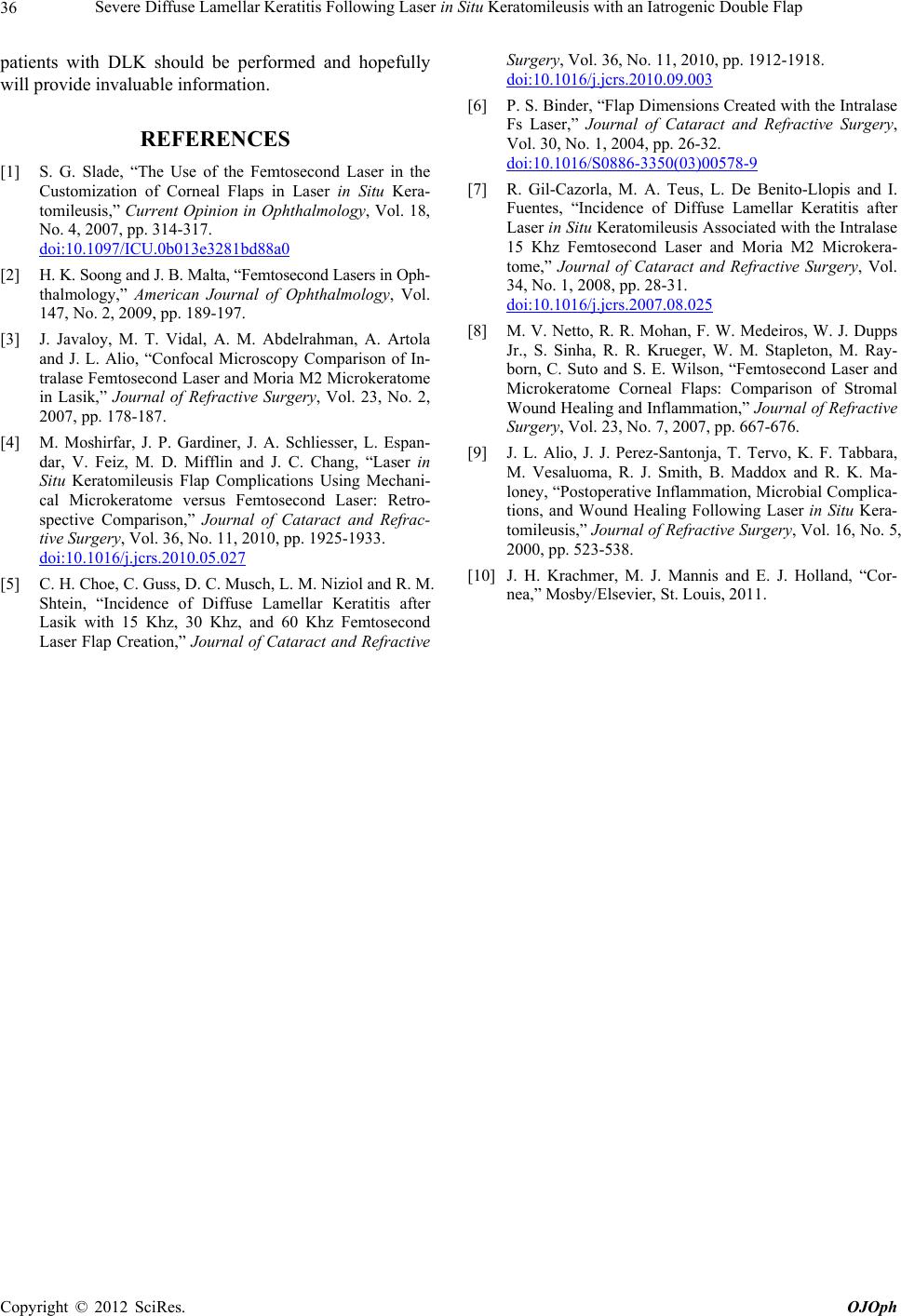
Figure 2. (a) Scheimpflug photograph of the right eye (1
week postoperatively). There is a diffuse layer of high pixel
intensity (arrowheads). Relatively high pixel intensity area
also can be seen in a shallower layer that is assumed to be
the flap (arrows); (b) On a Scheimpflug photograph of the
left eye (1 week postoperatively), there is an area of rela-
tively high pixel intensity in a shallower layer that is as-
sumed to be the flap (arrows); (c) Biomicroscopy of the
right eye 3 years postoperatively shows a corneal scar in the
deep stroma (arrowheads).
2. Discussion
The femtosecond laser delivers thousands of micro-
photodisruptive pulses to a specific corneal plane to ob-
tain a smooth cut and create a stromal flap with parallel
anterior and posterior surfaces [1]. The femtosecond la-
ser microkeratome has achieved good refractive out-
comes with a low complication rate [1,2], although sev-
eral studies have reported complications related to in-
flammatory reactions including DLK [2,3]. We present a
complicated case of severe DLK that developed in an
iatrogenic double flap after LASIK using a femtosecond
laser.
We described a rare complicated case of femtosecond
laser-assisted LASIK with an iatrogenic double flap that
resulted in development of severe DLK.
The low complication rate associated with flap crea-
tion [4] is an advantage of the laser microkeratome.
Nonetheless, in the current case, the surgeon ruptured the
deep stromal layer that resulted in the iatrogenic double
flap.
DLK is characterized by an inflammatory response at
the flap interface after LASIK. Although the detailed
etiology is unknown [5], DLK has been attributed to
multiple etiologies including bacterial endotoxins, chem-
icals, or debris produced during autoclaving or by surgi-
cal gloves and drapes, marking pens, meibomian gland
secretions, atopy, iatrogenic epithelial defects, low mean
endothelial cell density, and wide palpebral fissure height
[5]. DLK currently is thought to be related to the manner
in which endogenous factors modulate the patient re-
sponse to exogenous exposures [5].
The development of DLK after LASIK performed with
a mechanical microkeratome is well recognized. In con-
trast, the incidence of DLK after LASIK performed with
a femtosecond laser has been reported previously [3-7].
The incidence rates of DLK after LASIK in which a laser
keratome is used vary considerably and are higher than
with a mechanical microkeratome. It also has been re-
ported that higher laser energy levels may result in higher
DLK rates.
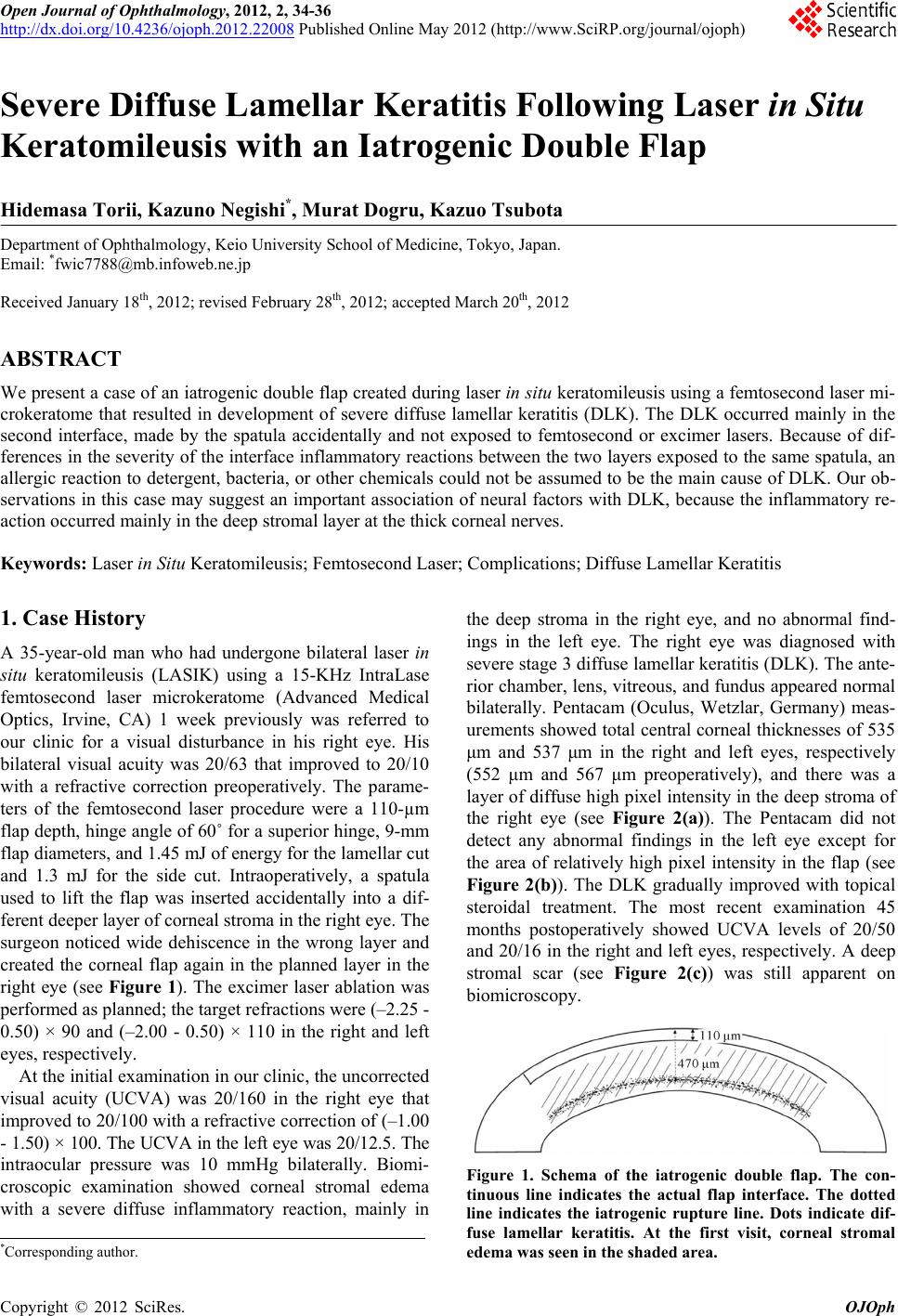
In the current case, there was a layer of diffuse high
pixel intensity in the deep stroma of the right eye, which
was the layer into which the surgeon accidentally in-
serted the spatula (see Figure 2(a)). A Scheimpflug im-
age showed inflammation in the deep stromal layer
where dehiscence was present and not in the actual flap
layer. Stromal cell necrosis associated with a femtosec-
ond laser flap likely contributes to greater inflammation
after LASIK, especially with higher energy levels that
result in higher rates of keratocyte cell death [8]. It also
was hypothesized that accumulated gas bubbles and
femtosecond laser energy may increase the inflammatory
response in patients who might be more susceptible to
DLK [7]. However, in the current case, the DLK mainly
developed in the second interface that was not exposed to
femtosecond or excimer lasers. In addition, the associa-
tion with exogenous factors such as an allergic reaction
to detergent, bacteria, or other chemicals could not be
assumed to be the main cause of DLK in the current case
because of the differing severities of the interface in-
flammatory reactions between the two layers, despite
almost the same procedure with the same instruments
except laser ablation. Alio et al. reported that corneal
innervation probably is involved in both the immediate
inflammatory response and long-term healing after LA-
SIK and photorefractive keratotomy [9]. Previous studies
have shown that the ciliary nerves of the ophthalmic
branch of the trigeminal nerve radially penetrate the cor-
nea in the deep peripheral stroma and then course anteri-
orly and the diameter increases with increasing distance
from the anterior corneal surface [10]. In the current case,
we believe that there was an important association of
neural factors with DLK, because the inflammatory reac-
tion developed mainly in the deep stromal layer where
the thick corneal nerves were damaged mechanically.
Further studies on the mechanisms of inflammation in
Copyright © 2012 SciRes. OJOph