S. Manduz et al. / HEALTH 2 (2010) 454-457
Copyright © 2010 SciRes. http://www.scirp.org/journalT /
456
Openly accessible at/HEALH
4. DISCUSSIONS
Some association has been suggested between Buerger’s
disease (TAO) and other syndromes but there is still no
consensus about diagnostic criteria. TAO is a nonathero-
sclerotic inflammatory disorder of unknown etiology
that affects small and medium-sized vessels of the ex-
tremities [1-3]. It is usually present at less than 40 years
old in male sex. However, last studies show that this
disease can be appears in smoking females [5]. In our
study, there were 28 (93%) males, 2 (7%) females’ cases
in TAO group and the mean age was 42.9 ± 14.3 years.
On the other hand, control group was consisted of 27
(90%) males, 3 (10%) females. Additionally 29 (97%)
subjects had smoking history in TAO group and 22 (73%)
in control group. TAO is diagnosed and treated with dif-
ficulty because of elusive etiology (10]. There is no suf-
ficient knowledge about the other risk factors and pre-
disposing conditions in the literature [11,12]. It was
documented that there was a strongly relationship be-
tween TAO and HLA-9 and HLA-B5. This situation
remind to genetical predisposition can be rolled in back-
ground of this disorder [5]. The effected vessel was
filled with the thrombus formation in microscopical
scanning [5]. Prothrombotic risk factors were observed
in this disease because of genetical suspicions and
thrombotic findings [6]. The 4G/5G alleles in PAI-1 and
MTHFR C677T gene polymorphisms may help to iden-
tify the couples at risk for recurrent pregnancy loss [13].
Abboud et al. showed that the risk of myocardial infarc-
tion (MI) was notably high in 4G and -844A carriers
with elevated plasma PAI-1 and were associated with
reduced tPA levels [14]. PAI-1 concentration increases
because of the 4G deletion of 675th promoter region of
PAI gene. Therefore, fibrinolytic activity is reduces and
predisposing thrombotic events are increases [15]. It was
demonstrated that all alone or combined effect of this
gene deletion was impacted deep venous thrombosis
(DVT), in studies [16]. Choudhury and friends detected
that the free PAI-1 levels can be significant venous oc-
clusion in TAO patients [17]. This gene mutation ac-
cused in Turkish DVT patients [18]. A meta-analyze
signs to 4G/4G genotype was 20% folds increased of
myocardial infarction risk that have included 9 studies
[19]. Another meta-analyze points to each 4G allele was
slightly increased of myocardial infarction risk that have
included 37 studies [20]. Recently another meta-analyze
that included 17 studies points that there was average
relation ship between 4G allele and venous thrombo-
emboli in subjects which have no genetical and acquired
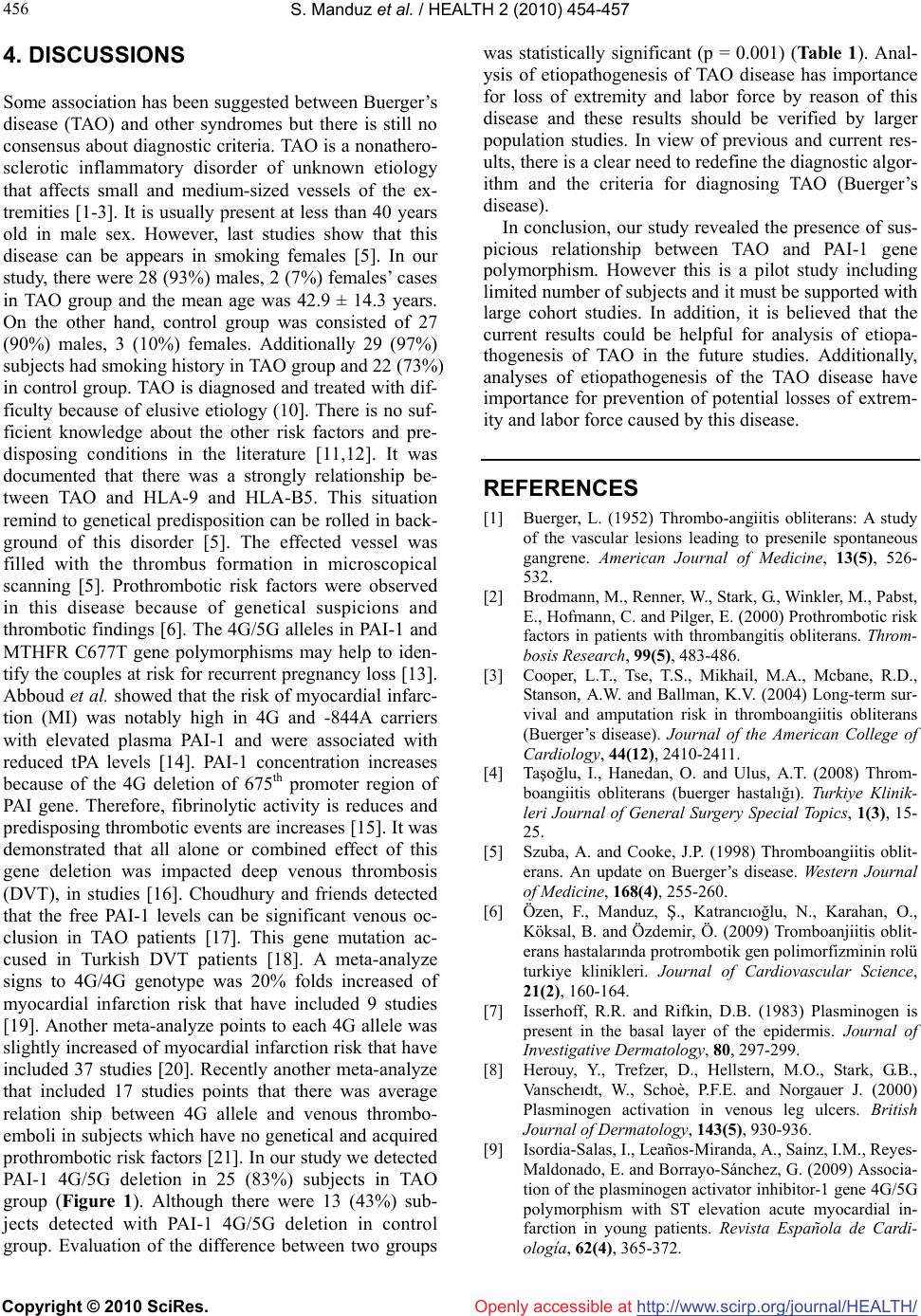
prothrombotic risk factors [21]. In our study we detected
PAI-1 4G/5G deletion in 25 (83%) subjects in TAO
group (Figure 1). Although there were 13 (43%) sub-
jects detected with PAI-1 4G/5G deletion in control
group. Evaluation of the difference between two groups
was statistically significant (p = 0.001) (Table 1). Anal-
ysis of etiopathogenesis of TAO disease has importance
for loss of extremity and labor force by reason of this
disease and these results should be verified by larger
population studies. In view of previous and current res-
ults, there is a clear need to redefine the diagnostic algor-
ithm and the criteria for diagnosing TAO (Buerger’s
disease).
In conclusion, our study revealed the presence of sus-
picious relationship between TAO and PAI-1 gene
polymorphism. However this is a pilot study including
limited number of subjects and it must be supported with
large cohort studies. In addition, it is believed that the
current results could be helpful for analysis of etiopa-
thogenesis of TAO in the future studies. Additionally,
analyses of etiopathogenesis of the TAO disease have
importance for prevention of potential losses of extrem-
ity and labor force caused by this disease.
REFERENCES
[1] Buerger, L. (1952) Thrombo-angiitis obliterans: A study
of the vascular lesions leading to presenile spontaneous
gangrene. American Journal of Medicine, 13(5), 526-
532.
[2] Brodmann, M., Renner, W., Stark, G., Winkler, M., Pabst,
E., Hofmann, C. and Pilger, E. (2000) Prothrombotic risk
factors in patients with thrombangitis obliterans. Throm-
bosis Research, 99(5), 483-486.
[3] Cooper, L.T., Tse, T.S., Mikhail, M.A., Mcbane, R.D.,
Stanson, A.W. and Ballman, K.V. (2004) Long-term sur-
vival and amputation risk in thromboangiitis obliterans
(Buerger’s disease). Journal of the American College of
Cardiology, 44(12), 2410-2411.
[4] Taşoğlu, I., Hanedan, O. and Ulus, A.T. (2008) Throm-
boangiitis obliterans (buerger hastalığı). Turkiye Klinik-
leri Journal of General Surgery Special Topics, 1(3), 15-
25.
[5] Szuba, A. and Cooke, J.P. (1998) Thromboangiitis oblit-
erans. An update on Buerger’s disease. Western Journal
of Medicine, 168(4), 255-260.
[6] Özen, F., Manduz, Ş., Katrancıoğlu, N., Karahan, O.,
Köksal, B. and Özdemir, Ö. (2009) Tromboanjiitis oblit-
erans hastalarında protrombotik gen polimorfizminin rolü
turkiye klinikleri. Journal of Cardiovascular Science,
21(2), 160-164.
[7] Isserhoff, R.R. and Rifkin, D.B. (1983) Plasminogen is
present in the basal layer of the epidermis. Journal of
Investigative Dermatology, 80, 297-299.
[8] Herouy, Y., Trefzer, D., Hellstern, M.O., Stark, G.B.,
Vanscheıdt, W., Schoè, P.F.E. and Norgauer J. (2000)
Plasminogen activation in venous leg ulcers. British
Journal of Dermatology, 143(5), 930-936.
[9] Isordia-Salas, I., Leaños-Miranda, A., Sainz, I.M., Reyes-
Maldonado, E. and Borrayo-Sánchez, G. (2009) Associa-
tion of the plasminogen activator inhibitor-1 gene 4G/5G
polymorphism with ST elevation acute myocardial in-
farction in young patients. Revista Española de Cardi-
ología, 62(4), 365-372.