Health
Vol.5 No.5(2013), Article ID:31964,10 pages DOI:10.4236/health.2013.55125
Multiple factors contribute to obesity among Kuwaiti college women
![]()
1Department of Community Medicine & Behavioural Sciences, Faculty of Medicine, University of Kuwait, Kuwait; *Corresponding Author: alisa@hsc.edu.kw
2Department of Medical Genetics, Centre for Molecular Medicine and Therapeutics, Child and Family Research Institute, University of British Columbia, Vancouver, Canada
3Department of Pediatrics, University of British Columbia, Vancouver, Canada
4BC Injury Research and Prevention Unit, Child and Family Research Institute, BC Children’s Hospital, Vancouver, Canada
Copyright © 2013 Abdulwahab Naser Al-Isa et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 29 January 2013; revised 12 March 2013; accepted 10 May 2013
Keywords: Obesity; Kuwait; Women; Eating Habits
ABSTRACT
There is a need to understand gender-dependent lifestyle habits of different ethnic groups in order to comprehend the risk factors associated with the development of obesity. It has been suggested that diet and physical exercise are two primary determinants of health. We examined the dietary habits and physical activity levels of Kuwaiti college women in order to understand these gender-specific factors contributing to obesity. A total of 304 female students were grouped as obese or non-obese as defined by their body mass index (BMI). Our study identified three factors that contributed to obesity: 1) consumption of more calories; 2) having obese parents and relatives; and 3) engagement in activities that consume less energy. Therefore, individually targeted weight management programs including healthy eating and active lifestyle interventions with a specific focus on female-friendly physical activity should be promoted within university settings in Kuwait.
1. INTRODUCTION
Obesity is defined as increased fat mass resulting from a chronic imbalance between energy intake and expenditure [1]. Currently, a sedentary lifestyle is a primary risk factor for the development of obesity [2]. Unfortunately, obesity increases the likelihood of developing metabolic diseases such as type 2 diabetes, heart disease, and certain types of cancers, obesity has been suggested as becoming the fifth leading cause of death world-wide [3]. In sixteen countries studied, obesity reduced longevity by up to two years in males [4] and in another report, a BMI above 32 was associated with the doubling of mortality in females [5]. A recent study published in Lancet noted that although the global obesity epidemic has been escalating for four decades, sustained prevention efforts have barely begun [6]. An individual’s pattern of lifestyle is usually set early in life, laying the foundation for subsequent health behaviours. Therefore, children and young adults are ideal target groups for new policies and programs sharing the importance of a healthy lifestyle [7,8].
Most cultures in the developing world indulge in food rich in fat and sugar. Until recently their active lifestyles compensated for these non-ideal eating habits. However, within the last 10 - 20 years rapid urbanization of these populations has allowed them to become increasingly sedentary. Similarly, the Kuwaiti population until the fifties relied on strenuous work for a living, however after that the emergence of the wealth of the country from oil brought in new enterprises leading to less need for physical activity. Therefore, the Kuwaiti population provides a useful example of health transitions and risk factors for overweight and obesity that can provide for a preventative policy development especially within the developing world [9].
The authors recently reported that among Kuwaiti college students, there is a higher prevalence of obesity in males as compared to females [10]. Interestingly, a number of studies carried out among college students world-wide suggest that obesity is indeed more prevalent in males than in females, primarily as the latter group has healthier eating habits [11-16]. Therefore, the authors hypothesized that the main cause of obesity among Kuwaiti college women is reduced physical activity and not unhealthy eating habits. This may not be entirely true because of lack of supportive material. As such, the present study was designed to closely examine lifestyle, dietary and exercise habits of Kuwaiti college women and compare their impact on obesity.
2. METHODS
2.1. Sample
Kuwait has one university attended by about 20,000 students annually [17]. The participants were recruited from students arriving to register and no compensation was given. A total of 304 female students were selected to participate in this study. The study included those who were apparently healthy. The authors at the onset of the study did not ask the participants if they suffered from a chronic disease until they agreed to participate in the study and until they were given the questionnaire. The students were guided into a lecture room and interviewed by trained female volunteer students. Their weight and height were measured by a nurse and following a verbal introduction describing the voluntary nature and purpose of the survey they were asked to complete a previously validated and published questionnaire [9,10,18] which obtained information on their dietary habits, lifestyle and activity preferences and socio-economic background. The data was collected from highly literate adult students at the College of Medical Sciences at the University of Kuwait. As such, our study was exempted from the University of Kuwait’s institutional ethics approval due to its non-invasive nature as previously described [10] Informed consent was obtained from each participant prior to enrolement in the study. The refusal rate at initial recruitment was less than 15%.
2.2. Measurements
Weight was measured to the nearest 0.1 kg with the subject in light indoor clothes, with emptied pockets and without shoes using a pre-calibrated SECA scale. Height was measured without shoes to the nearest 0.5 cm. The index of adiposity was determined by the body mass index (BMI), which is the weight in kilograms divided by the height in meters squared (Kg/m2). The classification [19] of the BMI categories are as follows: Non-obese (< 25 Kg/m2) and obese (BMI ≥ 25 Kg/m2).
2.3. Associated Factors
Age was divided into ≤19, 20 - 21, ≥22, as students fell into a narrow range which was best categorised as indicated. Other domains were divided into sub-factors as listed (Tables 1-6). Domains were classified as general characteristics, leisure time activities, weekly frequency of participating in sports, and dietary and health habits.
2.4. Data Analysis
The SPSS (Statistical Package for Social Sciences, version 19) was used for data analysis. In addition to descriptive statistics, the chi-square (p-value) test was used to assess the association between categorical variables. The logistic regression analysis was carried out using a binary variable: non-obese (BMI <25 kg/m2) or obese (BMI ≥ 25 kg/m2) as a dependent variable and the other variables as independent variables. The logistic regression approach provides adjusted odd ratios (OR; estimated relative risk) attributed to the independent variable in relation to a reference group. A p-value of ≤ 0.05 was used as the criterion of statistical significance.
3. RESULTS
3.1. Characteristics of Students
A total of 304 female students were categorized based on their BMI as non-obese and obese with ages ≤19, 20 - 21, ≥22 (Table 1). Distribution of students into nonobese verses obese categories was similar within each age group.
3.2. Eating Habits
Within both non-obese and obese groups, the majority reported engaging in snacking (Table 1). Interestingly, 38.6% of females who were obese self-reported dieting compared to 13.7% of those who were not. The majority had gained their nutritional knowledge from their parents and print media, regardless of being non-obese or obese (Table 4). Nevertheless, obese females were reported to have more obese parents and relatives (Table 1). Surprisingly, non-obese females consume more butter, full cream, non-diet soda and more sugar compared to those who were (Table 5). There were no significant differences between all other food types consumed. Females who were obese also tended to eat less after a dinner party compared to those who were not (Table 6). However, overall, the former group (27.1%) had the selfperception of consuming more calories as compared to the latter group (14.5%). Other eating habits were reported to be similar between the two groups.
3.3. Physical Activity
Level of exercise was divided into four sections: None, low, medium and high. The authors did not use standardised physical activity questionnaire. The study just wanted to know if a participant did or did not engage in physical activity and how often. Interestingly, the percentage of females engaged in exercise among those who were non-obese versus obese was similar (Table 1). Activity level and frequency of participating in certain sports also remained the same (Tables 1 and 3). However, more females who were obese appeared to work around the house and went to health clubs as compared to those who were not (Table 2). In contrast, they tended to take the lift and to play thinking games more often. The feeling of tiredness was also similar between the two groups (Table 1).
4. DISCUSSION
The current study was performed in order to identify potential risk factors that may lead to the development of obesity in young Kuwaiti college women. One of the authors previously reported that Kuwaiti college students lead sedentary lifestyles, expending low amounts of energy on physical activity [19]. Reduced physical activity was associated with an increased level of obesity. In this study, the authors found three factors that may contribute towards the resultant obesity in females: consumption of more calories, having obese parents and relatives, and engagement in activities that consume less energy. As the majority of the students gained their nutritional knowledge from their parents, it was apparent that they have been aware of appropriate healthy eating habits from very young age. However, studies frequently find that college students, regardless of gender, have unhealthy eating habits may be due to the time constraints placed on them in order to accommodate their study habits [20,21]. Similarly, this study reported that the majority of the students were used to snacking. The same time constraints may also restrict them from engaging in physical activity. Regardless of being non-obese or obese, the study found that majority of students engaged in none or a low level of exercise. In support of this finding, a previous study found that physical inactivity to be more common among Kuwaiti women than men [22]. Additional studies suggested lack of motivation; lack of energy; lack of knowledge; physical injuries and cost were found to act as barriers against physical activity [23]. Lack of motivation, energy, and boredom during exercise were significant factors influencing physical activity in a young Kuwaiti population [24]. While this study did not take physical injuries into account, the majority of participants appeared not to have any chronic diseases, nor did they have frequent health checkups. In addition, this study showed that some females did attend health clubs and had access to them. Their availability may be limited by cost as it also may be an important dictating factor. However, regarding this matter one study found no association among a sample of Kuwaiti population [24]. Safety and limited child-care have been reported as some additional barriers for females to engage in physical activity [23]. The latter, may not apply to Kuwaiti women due to easy access to servants. The cultural setting and the warm weather may also dictate that females cannot freely exercise outdoors [24]. Neighbourhood walkability has indeed been associated with physical activity among adolescents in low socioeconomic Belgian neighbourhoods [25,26]. Furthermore, studies conducted in Muslim countries showed that females were restrained from engaging in physical activities due to the customs and cultural attitudes of the society [27,28], although one study showed no such association [24]. In addition, it is rare to have no servants in most households of Kuwait, thus preventing most Kuwaitis from engaging in household activities.
Surprisingly, no significant differences were found between females who were non-obese versus obese in terms of their level of exercise and participation in sports, implying that the caloric intake and genetic predisposition were likely more important in this group as risk factors leading to the onset of obesity. Other factors that were not considered in this study such as marital status, pregnancies and birth control may have an impact on obesity in females. Girls in Middle Eastern cultures are known to marry young and to have multiple children [29]. Thus, ages of late teens and early twenties are probably when these females become most figure-conscious, as they want to be physically attractive in order to find a prospective husband. However, interestingly, in Kuwaiti culture, female plumpness is considered as a positive attribute [30]. All of these factors could influence healthpromoting behaviours in these young females.
Obesity was not associated with frequent health checkups or feelings of tiredness in this group, suggesting that it did not have a significant impact on health because obese Kuwaiti females work more around the house and attend health clubs. They also tended to eat less high calorie food such as cream, sugar and butter compared to the non-obese. Thus, these habits that should have had a positive impact on health and negative effect on obesity must have had developed secondary to the onset of obesity. Regardless of being non-obese or obese, the majority of participants consume more vegetables and fruits, grill their food, do not coat their bread with butter, frequently weigh themselves, read labels on food packaging and eat plant oils. These were indicators of prevalent healthy eating habits. This evidence showed that students already have some understanding of preventative measures against obesity.
Importantly, research showed that even those genetically susceptible to type 2 diabetes can delay its onset for 15 - 20 years with a little care and by following a lifestyle that includes regular daily exercise and a healthy diet [31]. In addition, there was a strong evidence that habitually engaging in physical activity decreases the risk of all-cause mortality and numerous chronic diseases
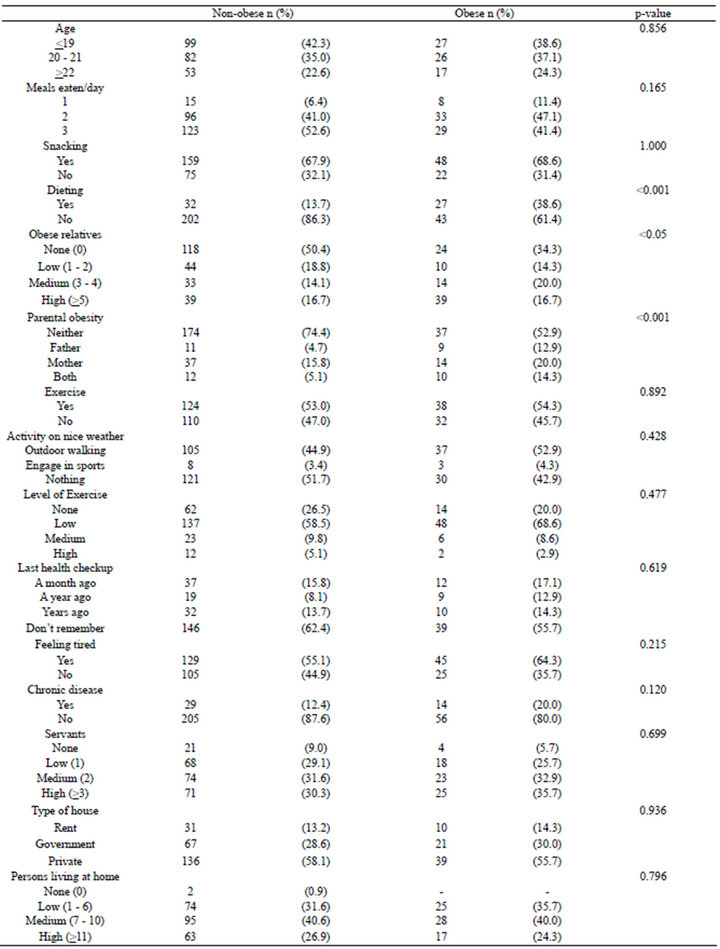
Table 1. Characteristics of the non-obese (BMI < 25 Kg/m2) and obese (BMI ≥ 25 Kg/m2) Kuwaiti College women sample (n = 304).

Table 2. Leisure-time activities of non-obese (BMI < 25 Kg/m2) and obese (BMI ≥ 25 Kg/m2) Kuwaiti college women (n = 304).
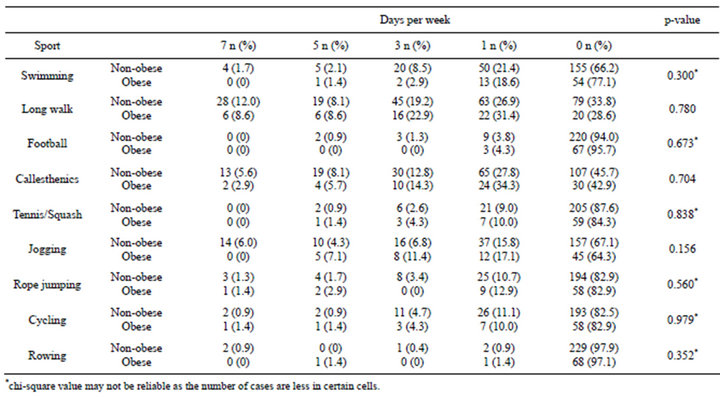
Table 3. Weekly frequency of indulging in sports by non-obese (BMI < 25 Kg/m2) and obese (BMI ≥ 25 Kg/m2) Kuwaiti college women (n = 304).
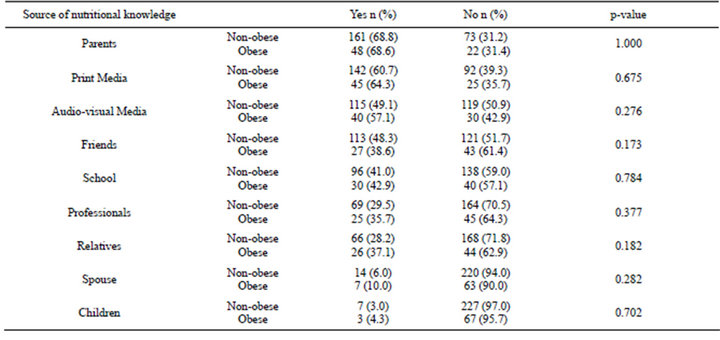
Table 4. Non-obese (BMI < 25 Kg/m2) and obese (BMI ≥ 25 Kg/m2) Kuwaiti college women’s sources of nutritional knowledge (n = 304).
such as hypertension, obesity, coronary heart disease, stroke, colon, breast cancer and depression [23]. A number of these diseases usually have their origins in childhood, which can be aided by physical activity early in life [32]. Especially for females, early intervention could help to improve bone health, and thus preventing osteoporosis. Research showed that physical activity can contribute to reduction in anxiety and depression in adolescents. Obesity has been indeed one of the most frequent causes of complications during pregnancy. Therefore, gaining an understanding of how to engage in a healthy lifestyle can help university students who wish to take action to protect themselves from the potential lifethreatening diseases [31].
The most frequently mentioned suggestion for helping university students to adopt healthier lifestyles has been offering health classes on campus to encourage the incorporation of an active lifestyle into their busy university learning routines [33]. There was sufficient evidence to support that individually focused weight management, healthy eating, and active lifestyle interventions in university settings must be implemented in conjunction with environmental-level interventions and modifications to facilitate students’ behaviour change [34]. As such, a course on healthy lifestyle could be added to first year students’ curriculum, which would include a daily onehour physical activity class with trained instructors. An important part of the course should be on promoting healthy nutrition and adequate physical activity. Such programs should be aimed at the aquisition of health benefits. The available literature showed that proximity of exercise facilities is a determinant factor of healthy lifestyles of undergraduate students [35]. Therefore, developing women-friendly university health facilities would be another viable policy for consideration [36]. A special focus should be given to promoting femalefriendly sports.
Environmental determinants of obesity must be addressed through healthy university internal policies that promote the availability and accessibility of a variety of low fat, high-fibre foods, fruits, and vegetables. These policies should aim at providing infrastructure for physical activity. Behavioural determinants of obesity must be addressed through the promotion of personal awareness, attitudes, beliefs, and skills that motivate and enable university students to modify unhealthy eating habits. Healthy lifestyles need to be supported by continuous and sustainable culturally appropriate education, awareness, and health promotion programs. Effective support for the maintenance or loss of weight among those already affected is also necessary.
Changes in lifestyle behaviours should be based on cultural and religious practises and can be used in enforcing policy changes [37]. The Prophet Muhammad (peace may be upon him) encouraged sporting activities and advised to eat only when hungry and to stop eating before becoming fully satiated. Importantly, the Amman Declaration on an Islamic Perspective on Health, supported and published by the World Health Organization, is an important resource for the university students as a guide for healthy living practices in Islamic countries [37,38].
In summary, there is a generalised need for college students to be educated in the areas of proper eating hab-

Table 5. Dietary and health habits of non-obese (BMI < 25 Kg/m2) and obese (BMI ≥ 25 Kg/m2) Kuwaiti college women (n = 304).
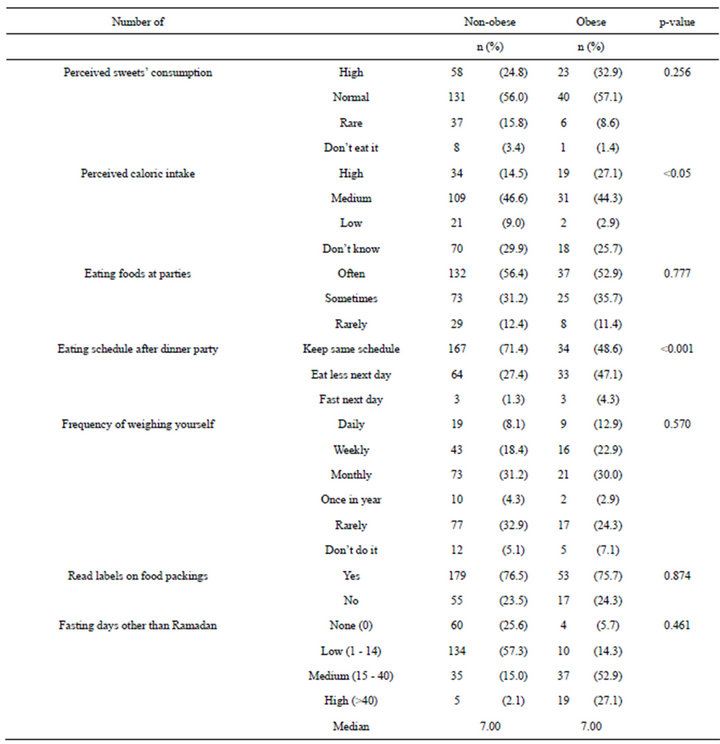
Table 6. Dietary and health habits of non-obese (BMI < 25 Kg/m2) and obese (BMI ≥ 25 Kg/m2) Kuwaiti college women (n = 304).
its and exercise, combined with annual physical examinations to assess their health in order to prevent the onset of obesity. Following the onset of this pathophysiological condition, it becomes more difficult to alter both eating habits and to engage in exercise. As this study population being the most knowledgeable of the country’s population, they remain the best group of individuals to promote health conscious ideals. They may in turn pass on their knowledge of healthy eating and exercise to future generations.
The limitation of the present study is that the sample size was not large enough to be representative for the sake of generalization.
REFERENCES
- Galgani, J. and Ravussin, E. (2010) Energy metabolism, fuel selection and body weight regulation. International Journal of Obesity, 32, S109-S119. doi:10.1038/ijo.2008.246
- Williams, P.T. (2011) Evidence that obesity risk factor potencies are weight dependent, a phenomenon that may explain accelerated weight gain in western societies. PLoS One, 6, e27657. doi:10.1371/journal.pone.0027657
- WHO (2009) Global health risks. http://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_part2.pdf
- Preston, S.H. and Stokes, A. (2011) Contribution of obesity to international differences in life expectancy. American Journal of Public Health, 101, 2137-2143. doi:10.2105/AJPH.2011.300219
- Manson, J.E., Willett, W.C., Stampfer, M.J., Colditz, G.A., Hunter, J.A., Hankinson, S.E., Hennekens, C.H. and Speizer, F.E. (1995) Body weight and mortality among women. The New England Journal of Medicine, 333, 677-685. doi:10.1056/NEJM199509143331101
- Gortmaker, S.L., Swinburn, B.A., Levy, D., Carter, R., Mabry, P.L., Finegood, D.T., Huang, T., Marsh, T. and Moodie, M.L. (2011) Changing the future of obesity: Science, policy, and action. Lancet, 378, 838-847.
- Filer, L.J., Lauer, R.M. and Leupker, R.V. (1994) Prevention of atherosclerosis and hypertension beginning in youth. Lea & Febiger, New York.
- Baranowski, T. (1997) Families and health actions. In: Gochman, D.S., Ed., Handbook of Health Behaviour Research, Personal and Social Determinants, Plenum, New York, 197-206.
- Al-Isa, A.N., Campbell, J. and Desapriya, E. (2013) Factors associated with overweight and obesity among Kuwaiti men. Asia-Pacific Journal of Public Health, 25, 63- 73.
- Al-Isa, A.N., Campbell, J., Desapriya, E. and Wijesinghe, N. (2011) Social and health factors associated with physical activity among Kuwait college students. Journal of Obesity, Article ID: 512363. doi:10.1155/2011/512363
- Ratanasiripong, P. and Burkey, H. (2011) Body mass index and body size perception: A normalizing of overweight and obesity among diverse college students. Californian Journal of Health Promotion, 9, 18-24.
- Abolfotouh, M.A., Bassiouni, F.A., Mounir, G.M. and Fayyad, R.C. (2007) Health related lifestyles and risk behaviours among students living in Alexandria university hostels. Eastern Mediterranean Health Journal, 13, 376- 391.
- Steptoe, A., Wardle, J., Cui, W., Bellisle, F., Zotti, A.M., Baranyai, R. and Sanderman, R. (2002) Trends in smoking, diet, physical exercise, and attitudes toward health in European university students from 13 countries, 1990-2000. Preventive Medicine, 35, 97-104. doi:10.1006/pmed.2002.1048
- Sakamaki, R., Toyama, K., Amamoto, R., Liu, C. and Shinfuku, N. (2005) Nutritional knowledge, food habits and health attitude of Chinese university students—A cross sectional study. Nutrition Journal, 4, 4. doi:10.1186/1475-2891-4-4
- Al-Ansari, M. and Al-Mannai, M. (2000) Body weights of university students in Baharain. Baharain Medical Bulletin, 22, 1-2.
- Yahia, N., Achkar, A., Abdallah, A. and Rizk, S. (2008) Eating habits and obesity among Lebanese university students. Nutrition Journal, 7, 32. doi:10.1186/1475-2891-7-32
- Al-Isa, A.N. (2006) Registrar’s office. Kuwait University, Kuwait City.
- Al-Isa, A.N., Campbell, J., Desapriya, E. and Wijesinghe, N. (2010) Factors associated with overweight and obesity among Kuwaiti elementary male school children aged 6 - 10 years. International Journal of Pediatrics, 2010, 1-7. doi:10.1155/2010/459261
- WHO Expert Committee (1995) Physical status: The use and interpretation of anthropometry. WHO Technical Report Series No. 854, WHO, Geneva.
- Huang, T., Harris, K.J., Lee, R.E., Nazir, N., Born, W. and Kaur, H. (2010) Assessing overweight, obesity, diet, and physical activity in college students. Journal of American College Health, 52, 83-86. doi:10.1080/07448480309595728
- Al-Rathaiaa, A.S., Fahmy, A.-E.A. and Al-Shawaiyat, N.M. (2010) Obesity and eating habits among college students in Saudi Arabia: A cross sectional study. Nutrition Journal, 9, 39. doi:10.1186/1475-2891-9-39
- Olusi, S.O., Al-Awadi, A.M. and Abraham, M. (2003) Baseline population survey data on the prevalence of risk factors for coronary disease among Kuwaitis aged 15 years and older. Annals of Saudi Medicine, 23, 162-166.
- Siddiqi, Z., Tiro, J.A. and Shuval, K. (2011) Understanding impediments and enablers to physical activity among African American adults: A systematic review of qualitative studies. Health Education Research, 26, 1010-1024. doi:10.1093/her/cyr068
- Arab, M. (2007) Barriers to exercise: Kuwaiti individuals with and without physical disabilities. Oregon State University, Corvallis.
- Meester, F.D., Dyck, D.V., Bourdeaudhuij, I.D., Deforche, B., Sallis, J.F. and Cardon, J. (2012) Active living neighborhoods: Is neighborhood walkability a key element for Belgian adolescents? BMC Public Health, 12, 7. doi:10.1186/1471-2458-12-7
- Steptoe, A. and Wardle, J. (2001) Health behaviour risk awareness and emotional well-being in students from Eastern Europe and Western Europe. Social Science & Medicine, 53, 1621-1630. doi:10.1016/S0277-9536(00)00446-9
- Kahan, D. (2003) Islam and physical activity: Implications for American sport and physical educators. Journal of Physical Education, Recreation and Dance, 74, 48-54. doi:10.1080/07303084.2003.10608470
- Zaman, H. (1997) Islam, well-being and physical activity: Perceptions of Muslim young women. In: Clarke, G. and Humberstone, B., Eds., Researching Women and Sport, Macmillan Press, Baringstoke, 50-68.
- Fakhouri, H. (2010) Early marriages and reasons for large families. Middle East Today. http://mid-east-today.blogspot.com/2010/08/early-marriages-and-reasons-for-large.html
- Galal, O. (2003) Nutrition-related health patterns in the Middle East. Asia Pacific Journal of Clinical Nutrition, 12, 337-343.
- WHO (2000) Workshop on obesity prevention and control strategies in the Pacific. http://www.wpro.who.int/internet/resources.ashx/NUT/Obesity+report.pdf
- WHO (2005) Girls’ participation in physical activities and sports: Benefits, patterns, influences and ways forward. World Health Organisation, Geneva.
- Davies, J., McCrae, B.P., Frank, J., Dochnahl, A., Pickering, T., Harrison, B., Zakrzewski, M. and Wilson, K. (2000) Identifying male college students’ perceived health needs, barriers to seeking help, and recommendations to help men adopt healthier lifestyles. Journal of American College Health, 48, 259-267. doi:10.1080/07448480009596267
- Greaney, M.L., Less, F.D., White, A.A., Dayton, S.F., Riebe, D., Blissmer, B., Shoff, S., Walsh, J.R. and Greene, G.W. (2009) College students’ barriers and enablers for healthful weight management: A qualitative study. Journal of Nutrition Education and Behavior, 41, 281-286. doi:10.1016/j.jneb.2008.04.354
- Reed, J.A. and Phillips, D.A. (2005) Relationship between physical activity and the proximity of exercise facilities and home exercise equipment used by undergraduate university students. Journal of American College Health, 53, 67-74. doi:10.3200/JACH.53.6.285-290
- Wendel-Vos, W., Droomers, M., Kremers, S., et al. (2007) Potential environmental determinants of physical activity in adults: A systematic review. Obesity Reviews, 8, 425- 440. doi:10.1111/j.1467-789X.2007.00370.x
- Dean, E. (2008) The crisis of lifestyle conditions in the Middle East with special attention to Kuwait: An unequivocal evidence-based call to action. Kuwait Medical Journal, 40, 184-190.
- WHO (1997) Health: An Islamic perspective. The Right Path to Health: Health Education through Religion, Regional Office for the Eastern Mediterranean, Alexandria.