M. O. THOMAS ET AL.
2
3) Definitive surgery in the theatre.
Procedures for damage control include aortic cross-
clamping, hilar clamping, major vessel ligation, pulmo-
nary tractotomy, simultaneously stapled pneumonectomy
or lobectomy, cardiac stapling, balloon catheter tampo-
nade, temporary intraluminal shunt, towel packing, towel
clip closure, single en masse closure of the chest wall
among others.
ET might also be indicated in definitive treatmen t as in
conditions like pericardial tamponade, many cases of
intra-thoracic bleeding, systemic air embolism, some lung
contusions, lung lacerations and so on. Kaiser and his
colleagues [3] at Irvine Medical Centre, California came
up with early independent predictions of the need for
emergency surgery to include prolonged extrication (odds
ratio (OR) 2.3), no loss of consciousness (OR 2.8), intu-
bation (OR 1.7), central line placement (OR1.7) and
blood transfus ion (OR 2.1) in all P < 0.05.
Emergency room thoracotomy saves about one in five
patients with isolated penetrating cardiac injury [1]. Mul-
tiple studies have shown that patients with isolated pene-
trating chest trauma have better outcomes than patients
who suffer blunt chest trauma without signs of life at the
scene or in the emergency department [5]. This is further
corroborated by the work of Ahmad and his team in Ka-
rachi [6]. In their series, post-thoracotomy mortality was
13.3% in penetrating injuries and 18.2% in patients who
suffered blunt injuries. In the same series, the combined
survival of emergency thoracotomy in 475 patients was
95.58%. They therefore concluded that early recognition
of treatable injuries and an aggressive approach in man-
agement of patients who need emergency thoracotomy
can increase chances of survival of patients suffering
from severe chest trauma.
Resuscitative thoracotomy (RT) is a time tested prac-
tice that gives direct access to the heart during cardio-
pulmonary resuscitation. The procedure has been and is
still very relevant in modern day practice. RT is also
considered to be more successful in penetrating cardiac
trauma than in blunt injuries of the heart with cardiovas-
cular collapse [8].
Wise and his colleagues [10] have gone further to
simplify instrumentation for ET. Specifically, they stated
that a clamshell incision performed using a big scalpel,
large scissors, large clamp and a gigli saw will suffice for
ET.
In all the works mentioned above, a common phe-
nomenon is the various positions taken by different prac-
titioners on the various aspects of emergency thora-
cotomy from definition to treatment. Therefore, further
literature enrichment would highlight various aspects of
ET.
Our study was conducted to highlight the indications
and management challenges of ET in a developing coun-
try. It was also to further enrich the literature in the all
important search for a common ground in the whole sub-
ject of emergency thoracotomy.
2. Methodology
The study period spanned 7 years from 2000 January to
December 2006. A protocol was designed to accommo-
date details of all thoracotomies performed in the first 24
hours of admission into Lagos University Teaching Hos-
pital, in Nigeria.
We noted patients’ bio-data to include ages and sexes,
specific indications for surgery, timing, clinical features,
operations performed, specific details of postoperative
care including complications and interventions.
The cases that met the criteria for emergency thora-
cotomy were extracted from the lot. Inclusion criteria
were thoracotomy performed within 24hours of patient
admission and all cases of re-thoracotomies. The patients
were followed up on admission taking specific note of
postoperative care to include blood transfusion needs,
absolute indication for postoperative ventilation and the
need for re-thoracotomy. Our criteria for absolute indica-
tion for postoperative ventilation was persistently low
SpO2 (<80%) with intra-nasal ox ygen.
The data so collected were analysed normally looking
at population distribution, dispersion, correlation of post-
operative events (mortality) with elective or emergency
thoracotomy.
3. Results
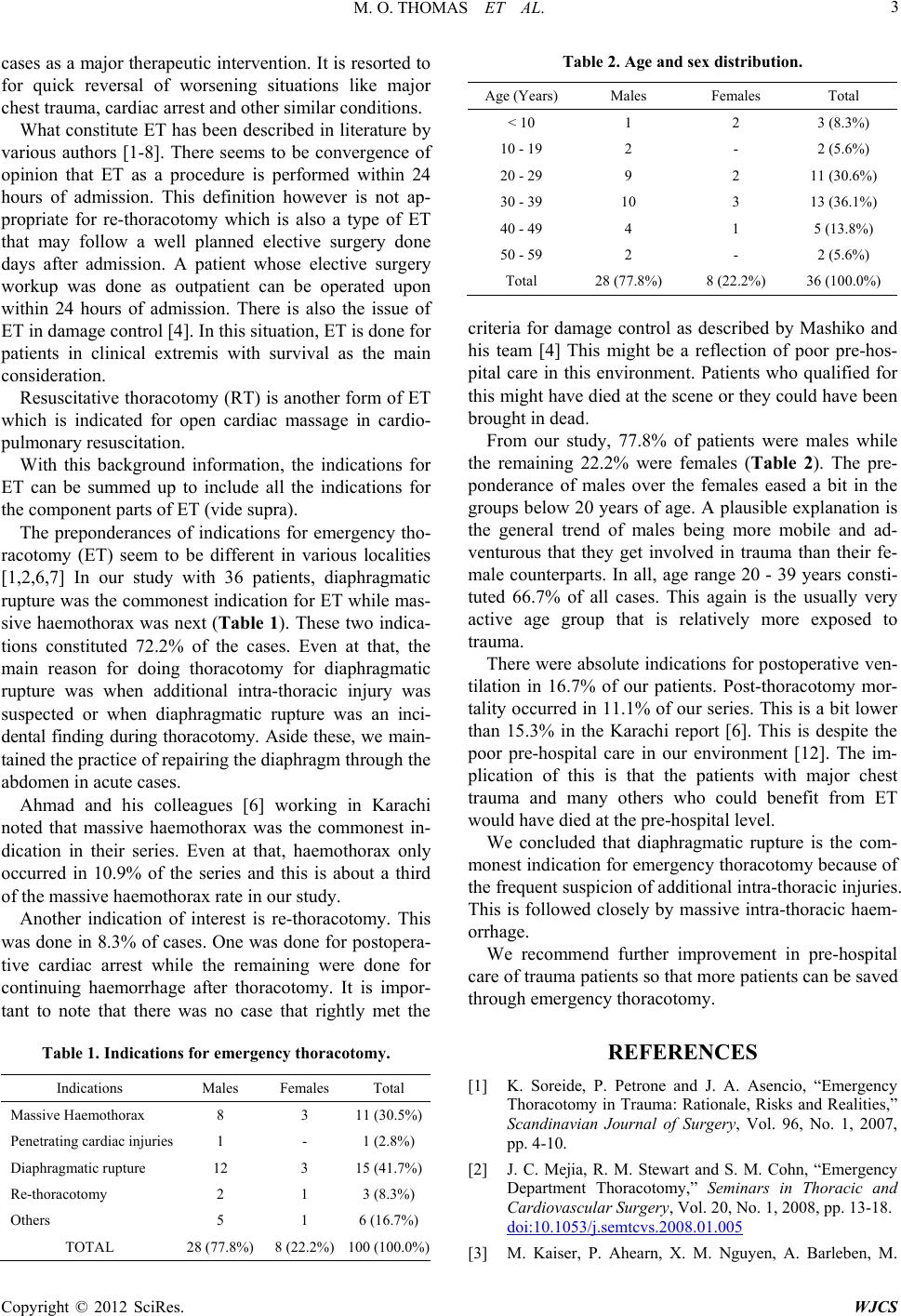
There were 36 patients for emergency thoracotomies
within the study period. They comprised of 28 males and
8 females giving a male to female ratio of 3.5:1. Within
the 20 - 39 year age range, there were 24 patients consti-
tuting 66.7% of the population. Age 19 and below pro-
duced only 5 patients constituting 13.9% of the cases.
The mean age was 33.7 ± 12.1 years and the median
was 32.1years. The mean and median were fairly close in
value giving a tendency to being a normal distribution
but the distribution was fairly platykurtic with Pearson
Skewness of +0. 39 .
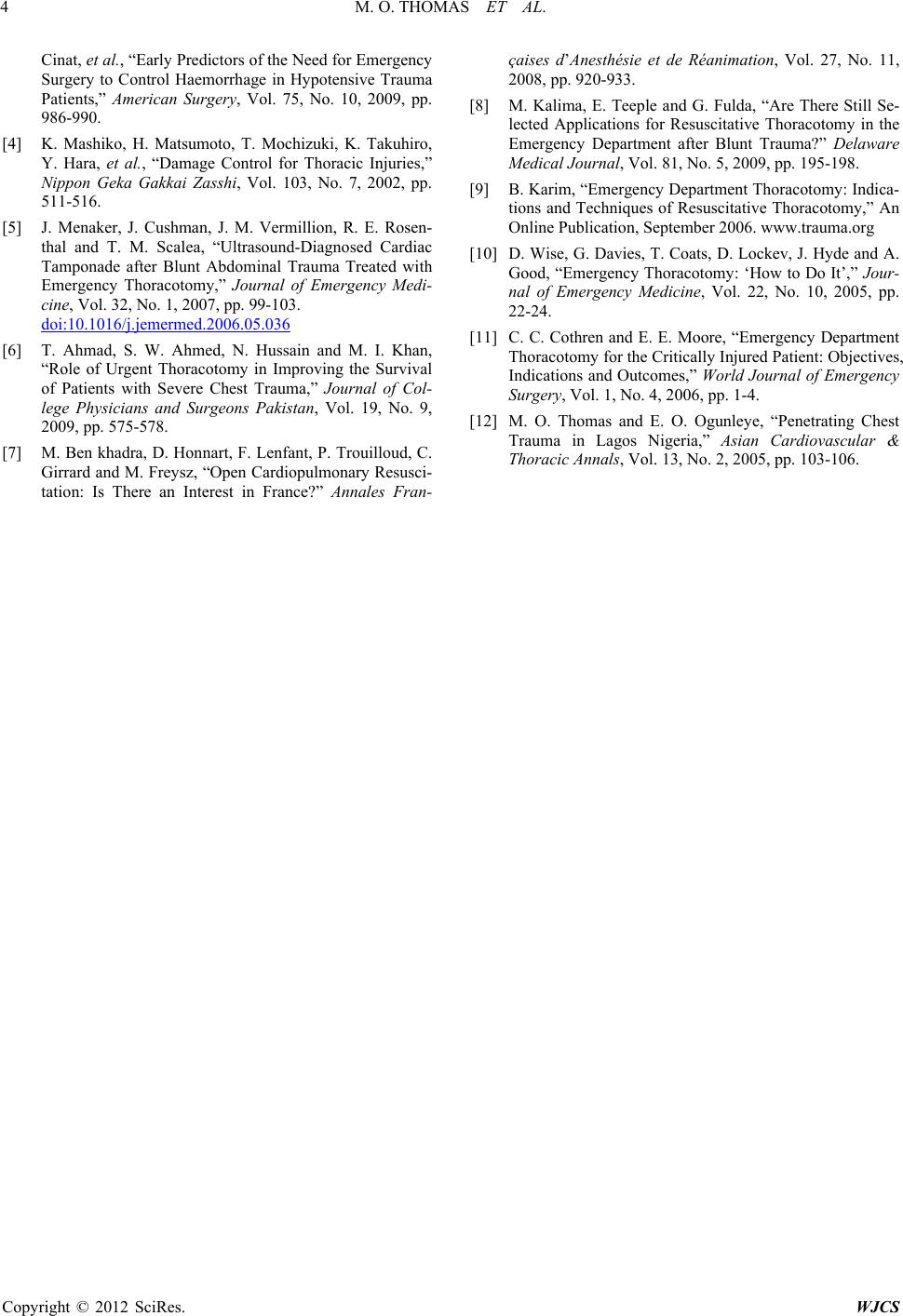
Massive Haemothorax was the indication in 11 (30.5%)
patients while diaphragmatic rupture occurred in 15
(41.7%) patents. Re-thoracotomy was the reason in 3
patients. Thoracotomy was done for 35 patients while
sternotomy was done for one patient who suffered pene-
trating cardiac trauma. Postoperative mortality occurred
in 4 (11.1%) of the patients. There were absolute indica-
tions for postoperative ventilatio n in 6 (16.7%) patients.
4. Discussion
In emergency situations, thoracotomy is done in most
Copyright © 2012 SciRes. WJCS