Open Journal of Obstetrics and Gynecology
Vol.08 No.13(2018), Article ID:88426,8 pages
10.4236/ojog.2018.813143
Uterine Didelphys in a Pregnant Mother
Omeed Paknejad1,2, Dana Bryant2*, Carla Peterkin2, Wendy Wilcox2
1Saint George’s University School of Medicine, St. George, Grenada
2New York City Health and Hospitals Corporation: Kings County Hospital Obstetrics, Gynecology, and Women’s Health, Brooklyn, NY, USA

Copyright © 2018 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY 4.0).
http://creativecommons.org/licenses/by/4.0/



Received: September 26, 2018; Accepted: November 10, 2018; Published: November 13, 2018
ABSTRACT
Background: Uterine Didelphys is a rare congenital condition and it can affect both mother and fetus. A 24 year-old patient presented to the emergency room with pelvic pain and a pelvic ultrasound confirmed the presence of Uterine Didelphys. She subsequently became pregnant and was first seen at 21 weeks gestation. She was designated as a high-risk patient during the second trimester when she experienced irregular contractions. She was monitored weekly with Non-Stress Tests and eventually was delivered by Cesarean Section. Uterine Didelphys can be detected in-utero in affected individuals, and clinical findings vary among individuals. Some may be asymptomatic, whereas others will experience dyspareunia, and still others may present with concurrent renal agenesis. Serial sonograms are performed throughout their pregnancy to evaluate fetal growth and well-being, as well as cervical length. Unlike many uterine anomalies, Uterine Didelphys does not affect fertility but can affect labor, fetal growth, placentation, fetal viability and fetal outcome. Uterine Didelphys frequently results in recurrent miscarriages and may cause preterm labor and necessitate cesarean section. The presentation, associated symptoms, methods of detection and management options for Uterine Didelphys will be discussed.
Keywords:
Uterine Didelphys and Pregnancy, Uterine Anomaly and Pregnancy

1. Introduction
Grigoris estimates that congenital uterine malformations may occur in up to 4.3% of women. It is reported that less than half of all pregnancies in patients with Uterine Didelphys (UD) result in a live birth. Up to 1 in 3 pregnancies end in abortion, about half end in premature deliveries, and the overall chance of a pregnancy reaching term is about 1 in 5 [1] - [6] . This report will focus on the importance of properly identifying and managing pregnant mothers with UD in order to maximize the likelihood of these mothers delivering a healthy baby at full-term.
2. Case(s)
A 24 year-old patient developed pelvic pain and the evaluation included a pelvic sonogram which revealed UD. When examined, she was found to have two full uteri and two full cervices but only one vagina and no vaginal septum.
Shortly after that, the patient became pregnant. She presented at 21 weeks gestation at which time the fetus was noted to be growing normally in the right uterine horn. During the second trimester, she experienced several episodes of irregular contractions and was treated for a urinary tract infection. At 31 weeks she presented for weekly Non-Stress Testing and repeated ultrasounds for fetal growth.
Her estimated due date was determined from her ultrasound evaluation at 21 weeks. At this visit at 31 weeks, the patient confirmed fetal movement but denied any vaginal bleeding or loss of fluids. She denied any pelvic pain or discomfort, abdominal pain, dyspareunia, or any previous miscarriages. She denied the presence of other medical problems, other surgical history, and any hospitalizations. She was taking only prenatal vitamins. She denied smoking, drinking, drug use, and denied any medicinal or seasonal allergies. The review of systems was normal for all systems. On physical exam, the patient was found to have normal vital signs and her physical exam was remarkable only for the gravid uterus which extended 32 cm. above the symphysis pubis. The lower extremities were not edematous.
The remainder of the pregnancy progressed without incident. She presented at 39 weeks 3 days gestation to the labor room and a tracing showed good fetal reactivity. An induction of labor was attempted but the tracing grew increasingly worrisome and the patient complained of decreased fetal movement. A fetal tracing now showed variable decelerations. She was consented for Cesarean Section, an epidural was placed, and a “J” incision was made on the uterus to access the infant. The pediatricians were present to assist with the delivery of the infant weighing 2725 grams and the APGAR scores were 9 at one minute and 9 at five minutes. Uterine atony was noted after delivery and the patient was treated with Pitocin, Methergine, Cytotec, and Hemabate with a good results. The placenta was consistent with a late term placenta; the cord was trivascular; and an infarct involving less than 5% of the placenta was noted. The patient had a prolonged hospital course and was discharged home on post-operative day nine.
At the first postnatal visit, she was noted to be in good spirits with a normal incision and a report that the baby was doing well.
3. Discussion
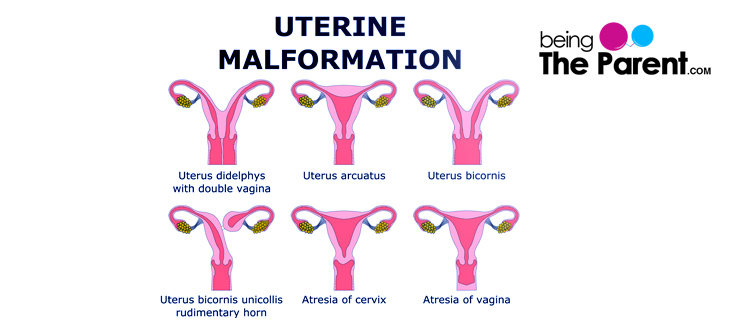
Uterine Didelphys is a rare congenital condition occurring in up to 4.3% of the women in the general population, and it can affect a mother and her fetus [1] [7] [8] [9] . UD is part of a broader classification of congenital defects known as Mullerian Duct Anomalies which occur during initial organogenesis. Failure of fusion of the Mullerian Ducts in any degree or subsequent failure of resorption of the tissue results in a spectrum of malformations. The actual cause of most Mullerian Duct Anomalies is unknown and, most likely, multifactorial [2] [10] . See Figure 1. UD is due to failure of midline fusion of the Mullerian ducts to form a single uterine body and cervix. This results in a double uterus with two separate cervices―rarely there may also be a duplicated vagina. UD primarily affects the viability of a pregnancy by causing cervical insufficiency but can further cause or contribute to other complications such as ectopic pregnancies, intrauterine growth restriction, abnormal placentation and/or fetal malpresentation. See Figure 2.
3.1. Classification
There are two main UD variations: UD unicollis and UD bicollis. Unicollis is more common, and it describes affected individuals where two uteri are connected to each-other within the cervix with only one vagina. Bicollis describes an individual that has two uterine cavities, each with its own cervix and vagina and no communication between them [7] [11] . See Figure 3. Our patient had a variant in which she had two full uteri with cervices, but did not have a vaginal septum.
UD is commonly associated with Renal Agenesis or other abnormalities like

Figure 1. This figure shows that failure of fusion of the Mullerian ducts e or subsequent failure of resorption of the uterine septum results in a spectrum of uterine malformation. https://www.beingtheparent.com/wp-content/uploads/2017/09/didelphys-uterus-complications.jpg
{kind=link}

Figure 2. A septate uterus has a normal fundal contour but is characterized by a persistent longitudinal septum that partially divides the uterine cavity. Bicornuate uterus is a partial failure of fusion of the Mullerian ducts, resulting in a uterus divided into two horns. https://i.pinimg.com/originals/c1/e5/70/c1e57089e77b6ebfd33aa310a9964f01.jpg
{kind=link}

Figure 3. A Uterine Didelphys can be classified as bicollis or unicollis. https://wearesurrogacy.com/wp-content/uploads/2018/04/uterus-didelphys-bicollis-vs-unicollis.png
{kind=link}
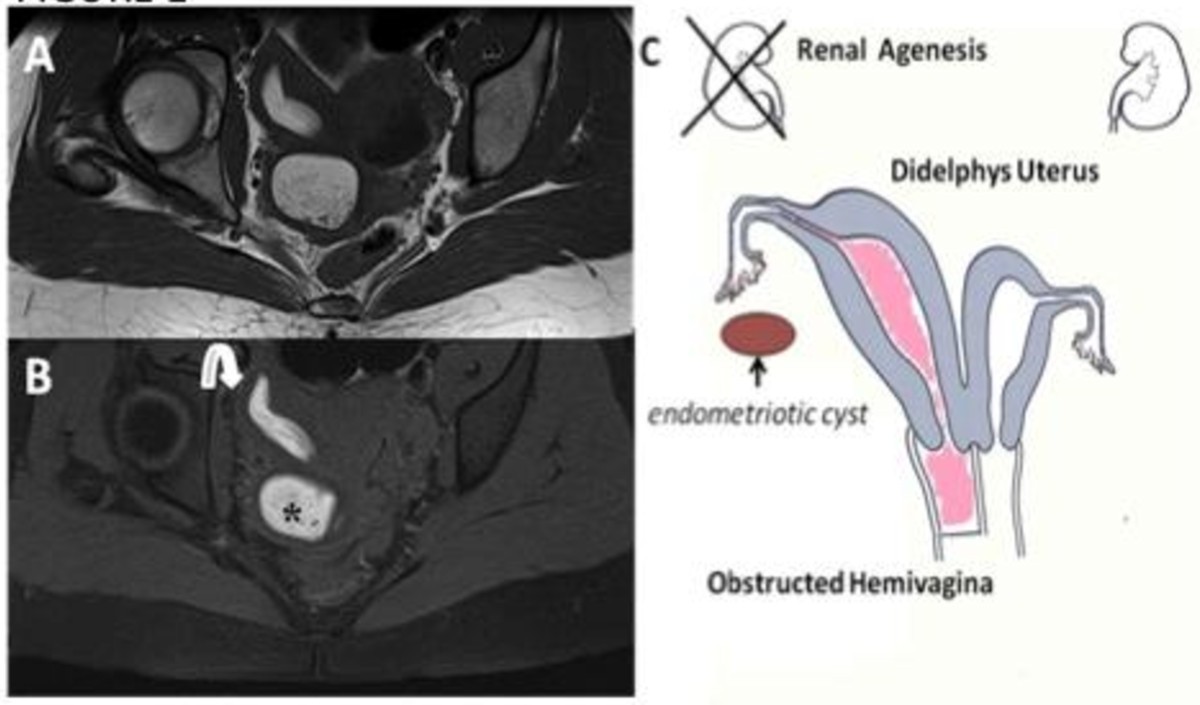
pelvic kidney. A vaginal septum is present in 75% of UD patients, and if the septum is transverse within the vaginal canal then it can cause obstruction of labor [12] . Herlyn-Werner-Wunderlich Syndrome in UD, also known as Obstructed Hemi-Vagina and Ipsilateral Renal Agenesis (OHVIRA) is a rare condition that is closely correlated with UD [13] . It occurs in puberty and exhibits non-specific and variable symptoms, with pelvic pain shortly following menarche [7] . See Figure 4.
3.2. Differential Diagnosis
UD can resemble other congenital malformations on physical examination, particularly a septate uterus or a bicornuate uterus. There are a few key differences that can help differentiate the latter two conditions from UD. A septate uterus has a normal fundal contour but has a persistent longitudinal septum which can partially (partial) or completely (complete) divide the uterine cavity. A bicornuate uterus is a partial failure of fusion of the ducts which then results in one uterus divided into two horns. Similar to a septate uterus, a bicornuate uterus can be designated as complete or partial and can additionally be categorized as bicollis and unicollis. See Figure 5.
3.3. Detection
UD is primarily detected via hysterosalpingogram (HSG) as it is a readily available and cost-effective detection method. Some complications may occur with HSG, most notably bleeding and/or infection. An ultrasound may also be utilized for UD detection as it is readily available and cost-effective, but the image provided is not as clear as with an HSG. An MRI is the gold standard for UD detection, but it is less commonly performed due to it being less accessible and having

Figure 4. Herlyn-Werner-Wunderlich Syndrome aka Uterine Didelphys with OHVIRA Syndrome presents with a triad of Uterine Didelphys, Obstructed Hemi-Vagina and Ipsilateral Renal Agenesis. It occurs at puberty and exhibits non-specific and variable symptoms with pelvic pain shortly following menarche. https://media.springernature.com/full/springer-static/image/art%3A10.1186%2F1471-2342-12-4/MediaObjects/12880_2011_Article_130_Fig1_HTML.jpg
{kind=link}

Figure 5. A septate uterus and bicornuate uterus have many similarities to Uterine Didelphys. Septate uterus has a normal fundal contour but is characterized by a persistent longitudinal septum that partially divides the uterine cavity. A bicornuate uterus is a partial failure of fusion of the ducts, resulting in a uterus divided into two horns. https://ars.els-cdn.com/content/image/1-s2.0-S0378603X14000631-gr1.jpg
{kind=link}

Figure 6. Hysterosalpingogram (USG) (top) is the primary imaging modality for making the diagnosis of Uterine Didelphys. With HSG the uterus is filled with water-soluble dye and a spot radiograph is taken. Notable complications of HSG include bleeding and infection. Ultrasound is a cost-effective and readily available method of imaging Uterine Didelphys but the diagnosis is more difficult to appreciate than that visualized with HSG and MRI. MRI has become the gold standard technique for diagnosis. Here the MRI shows two symmetric, widely divergent uterine horns and two cervixes, with an enlarged cavity filled by bloody/proteinaceous fluid due to haematocolpos are seen above. HSG: https://www.slideshare.net/airwave12/hysterosalpingography-33184676/22; US: https://en.wikipedia.org/wiki/Uterus_didelphys#/media/File:Ultrasound_Scan_ND_152.jpg; MRI: http://eu-csite-storage-prod.s3.amazonaws.com/www-eurorad-org/mediafiles/0000014563/000005_web.jpg.
{kind=link}
{kind=link}
a higher associated cost to perform [3] . See Figure 6. The intercornual distance, the distance between the distal ends of the uterine horns, is often calculated in conjunction with an HSG as it is helpful in differentiating a UD from a septate uterus and a bicornuate uterus; an intercornual distance greater than 4 cm is suggestive of UD [3] .
4. Conclusion
In pregnancy, a patient with a uterine anomaly should be referred and followed by a maternal fetal medicine specialist. The patient should be counseled about premature labor, abnormal placentation, abnormal lie, fetal growth restriction, abnormal labor progression, and possible Cesarean section. Serial sonograms should be performed on a monthly basis in order to evaluate fetal well-being and growth, and to assess the mother’s cervical length. Weekly non-stress tests are recommended in the third trimester. Through early detection and proper management, a UD mother optimizes her chances of having a full-term pregnancy.
Acknowledgements
We would like to thank our patient who agreed to having her story told and Michele Follen, MD, PhD, for her teaching and encouragement.
Conflicts of Interest
The authors declare no conflicts of interest regarding the publication of this paper.
Cite this paper
Paknejad, O., Bryant, D., Peterkin, C. and Wilcox, W. (2018) Uterine Didelphys in a Pregnant Mother. Open Journal of Obstetrics and Gynecology, 8, 1423-1430. https://doi.org/10.4236/ojog.2018.813143
References
- 1. Grimbizis, G.F., Camus, M., et al. (2001) Clinical Implications of Uterine Malformations and Hysteroscopic Treatment Results. Human Reproduction Update, 7, 161-174. https://doi.org/10.1093/humupd/7.2.161
- 2. Jahromy, M. and Ansari, I. (2018) Double Uterus with Single Cervix: A Case Report. https://cdn.neoscriber.org/cdn/serve/3144c/245fc24cc3d3087f0d240cc012bcefa52214fe28/amhsr-In_Press-In_Press-64494.pdf
- 3. Gaillard, F. (n.d.) Uterus Didelphys | Radiology Reference Article. https://radiopaedia.org/articles/uterus-didelphys
- 4. Katke, R.D., Acharya, S. and Mourya, S. (2017) Uterus Didelphys with Pregnancy and Its Different Maternal and Perinatal Outcomes. http://www.ijrcog.org/index.php/ijrcog/article/view/2801
- 5. AlWahab Abo Dewan, K., Hefeda, M., et al. (2014) Septate or Bicornuate Uterus: Accuracy of Three-Dimensional Trans-Vaginal Ultrasonography and Pelvic Magnetic Resonance Imaging. The Egyptian Journal of Radiology and Nuclear Medicine, 45, 987-995. https://doi.org/10.1016/j.ejrnm.2014.04.001
- 6. Pankaja, S., Ip, P. and O’Mahony, F. (2016) Successful Pregnancy with Uterus Didelphys. Journal of Andrology & Gynecology, 4, 3.
- 7. Sawai, D., Sharma, S.K., Sawai, D.S., Sawai, U., Sharma, S. and Sharma, A. (2017) Pregnancy in Uterus Didelphys Delivered by Caesarean Section: A Case Report. http://www.ijrcog.org/index.php/ijrcog/article/view/3669
- 8. Sneha, R., Anitha, G.S. and Chandralekha, P. (2016) Pregnancy in Uterus Didelphys Delivered by Caesarean Delivery: Case Report. https://doi.org/10.18203/2320-1770.ijrcog20162143
- 9. Ng’ang’a, N., Ratzersdorfer, J. and Abdelhak, Y. (2017) Vaginal Birth after Two Previous Caesarean Deliveries in a Patient with Uterus Didelphys and an Interuterine Septal Defect. https://europepmc.org/abstract/med/28584004
- 10. Rezai, S., Bisram, P., et al. (2015) Didelphys Uterus: A Case Report and Review of the Literature. Case Reports in Obstetrics and Gynecology, 2015, Article ID: 865821. https://www.hindawi.com/journals/criog/2015/865821/ https://doi.org/10.1155/2015/865821
- 11. Med.firecracker.me. (2018) Firecracker. https://med.firecracker.me/app#/tree/1/1-27-61-136-812
- 12. Mesquita, R.D., Sousa, M., et al. (2017) The Clinical Relevance of Anatomical Variants! http://www.eurorad.org/case.php?id=14563
- 13. Vescovo, D.R., et al. (2012) Herlyn-Werner-Wunderlich Syndrome: MRI Findings, Radiological Guide (Two Cases and Literature Review), and Differential Diagnosis. http://bmcmedimaging.biomedcentral.com/articles/10.1186/1471-2342-12-4