J. B. Granild-Jensen et al. / Open Journal of Pediatrics 1 (2011) 64-66
Copyright © 2011 SciRes. OJPed
66
5. ACKNOWLEDGEMENTS
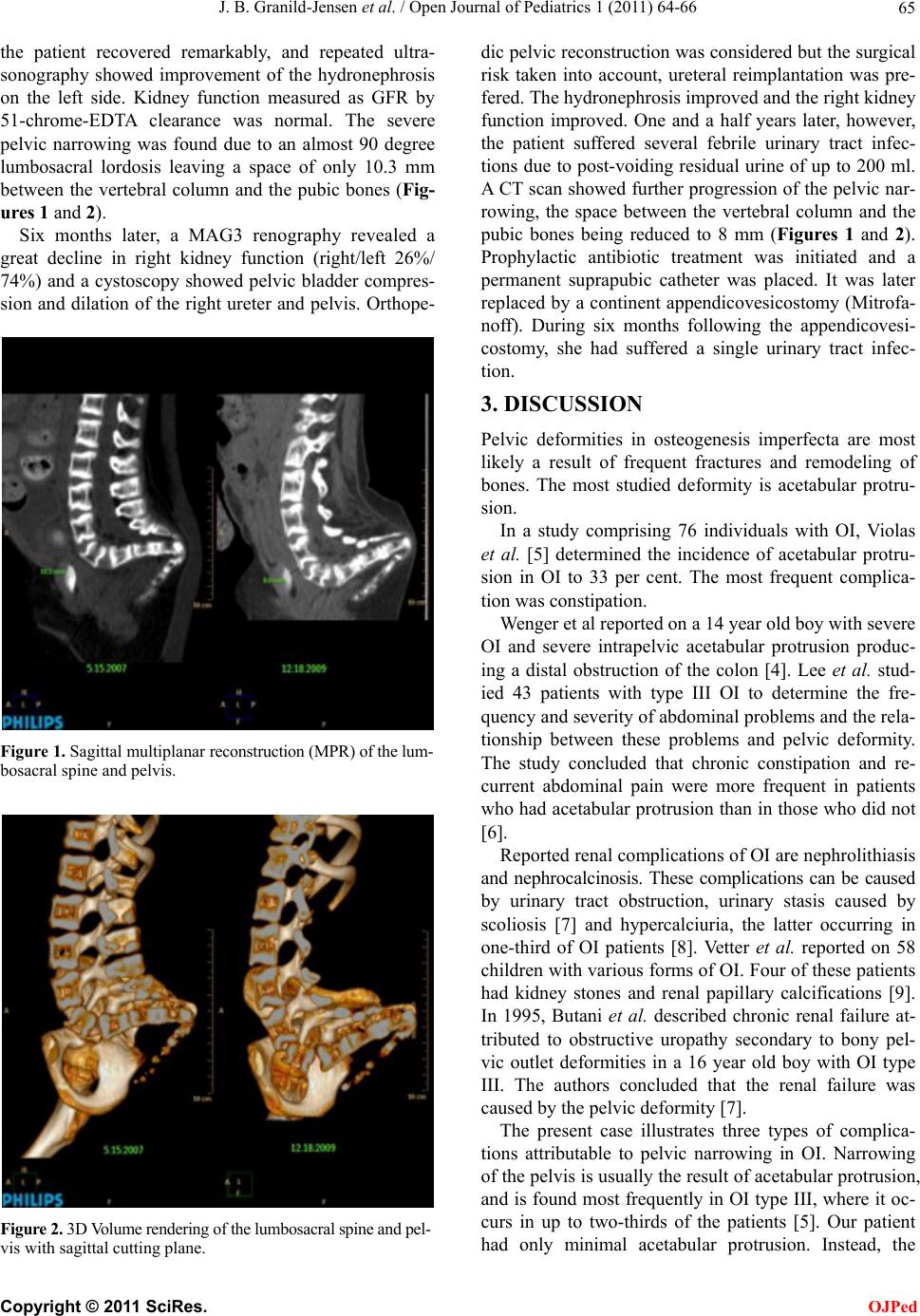
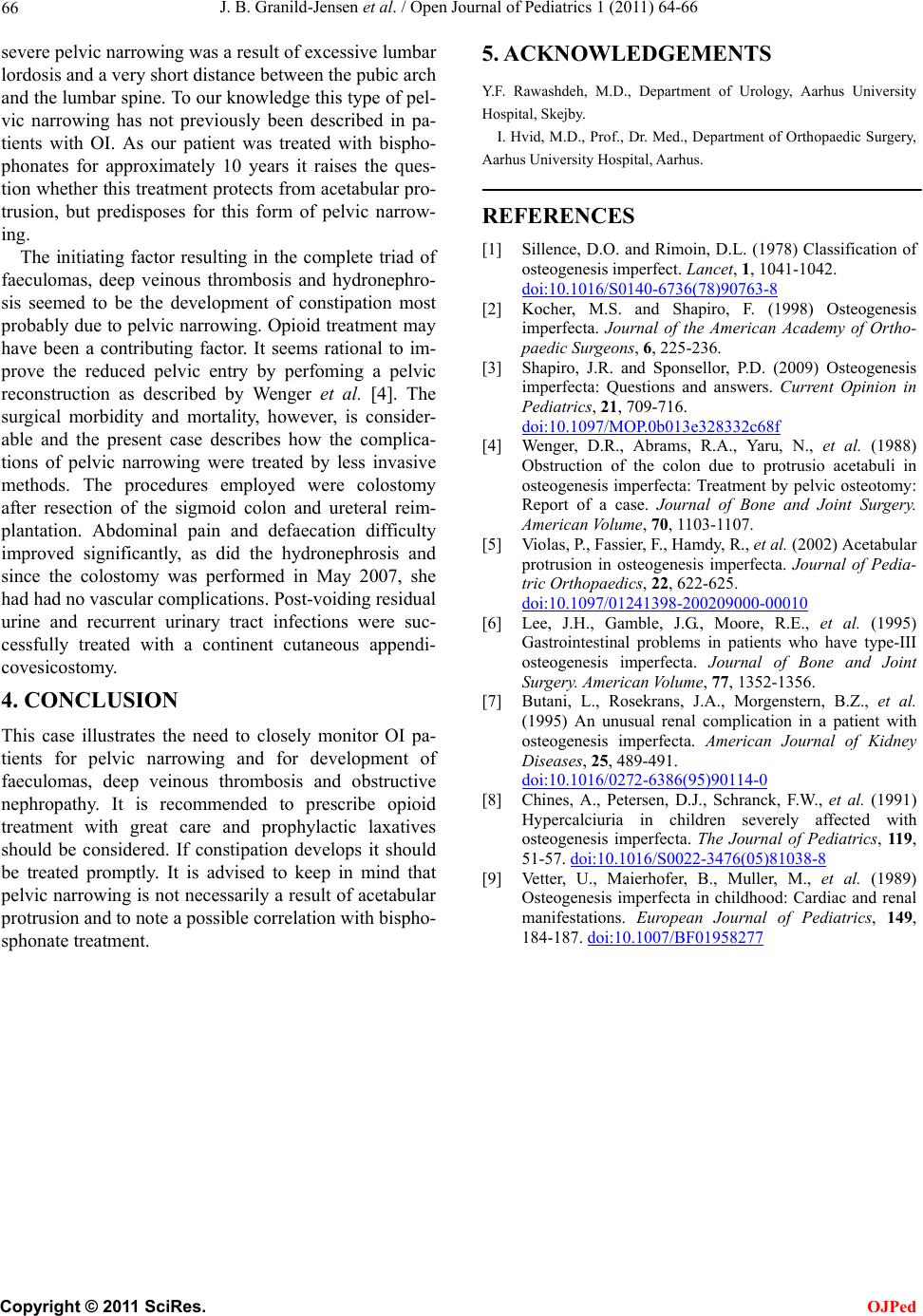
severe pelvic narrowing was a result of excessive lumbar
lordosis and a very short distance between the pubic arch
and the lumbar spine. To our knowledge this typ e of pel-
vic narrowing has not previously been described in pa-
tients with OI. As our patient was treated with bispho-
phonates for approximately 10 years it raises the ques-
tion whether this treatment protects from acetabular pro-
trusion, but predisposes for this form of pelvic narrow-
ing.
Y.F. Rawashdeh, M.D., Department of Urology, Aarhus University
Hospital, Skejby.
I. Hvid, M.D., P rof., Dr. Med., Department of Orthop aedic Surgery,
Aarhus University Hospital, Aarhus.
REFERENCES
[1] Sillence, D.O. and Rimoin, D.L. (1978) Classification of
osteogenesis imperfect. Lancet, 1, 1041-1042.
doi:10.1016/S0140-6736(78)90763-8
The initiating factor resulting in the complete triad of
faeculomas, deep veinous thrombosis and hydronephro-
sis seemed to be the development of constipation most
probably due to pelvic narrowing. Opioid treatment may
have been a contributing factor. It seems rational to im-
prove the reduced pelvic entry by perfoming a pelvic
reconstruction as described by Wenger et al. [4]. The
surgical morbidity and mortality, however, is consider-
able and the present case describes how the complica-
tions of pelvic narrowing were treated by less invasive
methods. The procedures employed were colostomy
after resection of the sigmoid colon and ureteral reim-
plantation. Abdominal pain and defaecation difficulty
improved significantly, as did the hydronephrosis and
since the colostomy was performed in May 2007, she
had had no vascular complications. Post-voiding residual
urine and recurrent urinary tract infections were suc-
cessfully treated with a continent cutaneous appendi-
covesicostomy.
[2] Kocher, M.S. and Shapiro, F. (1998) Osteogenesis
imperfecta. Journal of the American Academy of Ortho-
paedic Surgeons, 6, 225-236.
[3] Shapiro, J.R. and Sponsellor, P.D. (2009) Osteogenesis
imperfecta: Questions and answers. Current Opinion in
Pediatrics, 21, 709-716.
doi:10.1097/MOP.0b013e328332c68f
[4] Wenger, D.R., Abrams, R.A., Yaru, N., et al. (1988)
Obstruction of the colon due to protrusio acetabuli in
osteogenesis imperfecta: Treatment by pelvic osteotomy:
Report of a case. Journal of Bone and Joint Surgery.
American Volume, 70, 1103-1107.
[5] Violas, P., Fassier, F., Hamdy, R., et al. (2002) Acetabular
protrusion in osteogenesis imperfecta. Journal of Pedia-
tric Orthopaedics, 22, 622-625.
doi:10.1097/01241398-200209000-00010
[6] Lee, J.H., Gamble, J.G., Moore, R.E., et al. (1995)
Gastrointestinal problems in patients who have type-III
osteogenesis imperfecta. Journal of Bone and Joint
Sur gery. American Volume, 77, 1352-1356.
4. CONCLUSION [7] Butani, L., Rosekrans, J.A., Morgenstern, B.Z., et al.
(1995) An unusual renal complication in a patient with
osteogenesis imperfecta. American Journal of Kidney
Diseases, 25, 489-491.
doi:10.1016/0272-6386(95)90114-0
This case illustrates the need to closely monitor OI pa-
tients for pelvic narrowing and for development of
faeculomas, deep veinous thrombosis and obstructive
nephropathy. It is recommended to prescribe opioid
treatment with great care and prophylactic laxatives
should be considered. If constipation develops it should
be treated promptly. It is advised to keep in mind that
pelvic narrowing is not necessarily a result of acetabular
protrusion and to note a possible correlation with bispho-
sphonate treatment.
[8] Chines, A., Petersen, D.J., Schranck, F.W., et al. (1991)
Hypercalciuria in children severely affected with
osteogenesis imperfecta. The Journal of Pediatrics, 119,
51-57. doi:10.1016/S0022-3476(05)81038-8
[9] Vetter, U., Maierhofer, B., Muller, M., et al. (1989)
Osteogenesis imperfecta in childhood: Cardiac and renal
manifestations. European Journal of Pediatrics, 149,
184-187. doi:10.1007/BF01958277