K. Dahiya et al. / Open Journal of Obstetrics and Gynecology 1 (2011) 242-244
Copyright © 2011 SciRes. OJOG
244
[3] Gupta, N.P. and Ansari, M.S. (2002) Mayer-Rokitansky-
Kuster-Hauser (MRKH) syndrome—A review. Indian
Journal of Urology, 18, 111-116.
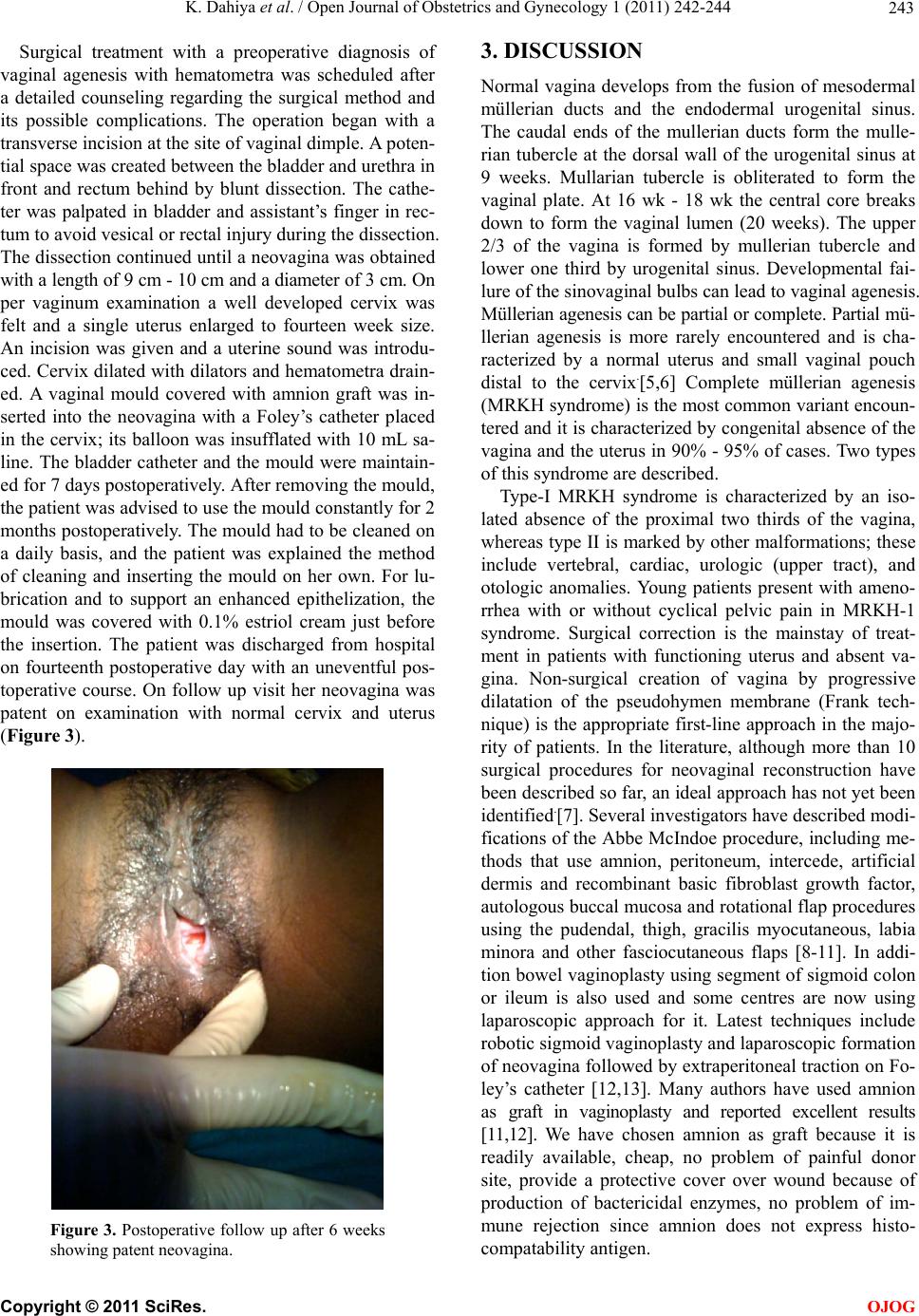
In such patients the commonly used technique com-
bining McIndoe Vaginoplasty along with an abdominal
approach to drain the hematometra has been reported
with good results. In this case we have used only peri-
neal approach to dissect a neovagina and identify the ce-
rvix with formation of a patent drainage tract and a total
vaginal length of 9 cm. The morbidity of the patient was
decreased with relief of symptoms, formation of a func-
tional vagina and absence of an abdominal scar with no
breach in the integrity of uterus. Using an appropriate
vaginal mould is one of the keys to achieving a success-
ful result in neovaginal reconstruction. Vaginal moulds
which are used to prevent re-stenosis of created neova-
gina may be associated with a lot of problems. Poor dra-
inage, graft maceratio n, sloughing, and graft detachment
may be caused by non ideal vaginal moulds and lead to
an unsatisfactory reconstruction [8,9].
[4] ACOG Committee Opinion (2002) Nonsurgical diagnosis
and management of vaginal agenesis. International Jou-
rnal of Gynecology and Obstetrics, 79, 167-170.
doi:10.1016/S0020-7292(02)00326-0
[5] Jones, H.W. JR. and Scott, W.M. (1958) Hermaphroditism,
genital anomalies, and related endocrine disorders. 2nd
Edition, Williams & Wilkins Co., Baltimore, 327.
[6] Jones, H.W. Jr. and Wheeless, C.R. (1969) Salvage of the
reproductive potential of women with anomalous devel-
opment of the muellerian ducts. American Journal of Ob-
stetrics and Gynecology, 104, 348-352.
[7] Seccia, A., Salgarello, M., Sturla, M., Loreti, A., Latorre,
S. and Farallo, E. (2002) Neovaginal reconstruction with
the modified mcIndoe technique: A review of 32 cases.
Annals of Plastic Surgery, 49, 379-384.
doi:10.1097/00000637-200210000-00008
[8] McIndoe, A. (1950) The treatment of congenital absence
and obliterative conditions of the vagina. British Journal
of Plastic Surgery, 2, 254-267.
Here we use a vaginal mould made of dental material
hollow from inside. An intrauterine placement of Foley’s
catheter allows continuous drainage and maintains a
patent tract in early post-operative period. On follow up
visits the patient was seen to have a total vaginal length
of 9 cm with epithelised patent vagina. She was advised
to use the mould coated with estradiol cream continuou-
sly for 2 months with use of a disinfectant for cleaning.
Mould was to be removed only while urinating or defe-
cating. Later she was told to use it for another 3 months
at night.
[9] Yu, K.J., Lin, Y.S., Chao, K.C., Chang, S.P., Lin, L.Y.
and Bell, W. (2004) A detachable porous vaginal mould
facilitates reconstruction of a modified mcIndoe ne-
ovagina. Fertility and Sterility, 81, 435-439.
doi:10.1016/j.fertnstert.2003.06.032
[10] Chohan, A., Burr, F., Mansoor, H. and Falak, T. (2006)
Amnion graft in vaginoplasty—An experience at 3 teach-
ing hospitals of Lahore. Biomedica, 22, 21-24.
[11] Fotopoulou, C., Sehouli, J., Gehrmann, N., Schoenborn, I.
and Lichtenegger, W. (2009) Functional and anatomical
results of amnion vaginoplasty in young women with
May er-Rokitansky-Kuster-Hauser syndrome. Fertility and
Sterility, (Epub ahead of print).
Preservation of the uterus should always be attempted
in patients with in patients of vaginal agenesis with he-
matometra. Thus reproductive capacity is preserved, al-
though the patients should be aware of the fact that al-
though the possibility of spontaneous pregnancy exists,
assisted reproduction techniques may eventually be ne-
cessary. Repeated episodes of hematometra, endometrio-
sis have been reported in conservative management of
such cases. In some cases, however due to the recurrent
obstruction, radical treatment by hysterectomy has been
reported as a last option [13-15].
[12] Fedele, L., Bianchi, S., Zanconato, G. and Raffaelli, R.
(2000) Laparoscopic creation of neovagina in patients
with rokitansky syndrome: Analysis of 52 cases. Fertility
and Sterility, 74, 384-389.
doi:10.1016/S0015-0282(00)00620-8
[13] Cai, B., Zhang, J.R., Xi, X.W., Yan, Q. and Wan, X.P.
(2007) Laparoscopically assisted sigmoid colon vagino-
plasty in women with Mayor-Rokitansky-Kuster-Hauser
syndrome: Feasibility and shortterm results. British
Journal of Obstetrics and Gynaecology, 114, 1486-1492.
d oi: 10 .1111 /j .1 471 -0528.2007.01514.x
[14] Rana, A., Gurung, G., Begum, S.H., Adhikari, S. and
Neupane, B.B. (2007) Hysterectomy for hematometra in
a 15-year-old mentally handicapped girl with congenital
cervicovaginal agenesis and concomitant ovarian ade-
noma. Journal of Obstetrics and Gynecology, 34,
105-107. d oi: 10 .1111/ j. 1447-0756.2007.00726.x
REFERENCES
[1] Saxena, A.K. and Herman, M.I. (2009) Vaginal Atresia.
Webpage. Cited June 02, 2009.
http://emedicine.medscape.com/article/954110-print [15] Roszaman, R. and Ghazali, I. (2006) Vaginal and cervical
agenesis—Hysterectomy in a young girl. Internal Medi-
cine Journal, 5.
[2] Saraf, S. and Saraf, P. (2007) McIndoe vaginoplasty:
Revisited. International Journal of Gynecology and Ob-
stetrics, 6, Online Journal.