 Advances in Infectious Diseases, 2011, 1, 20-26 doi:10.4236/aid.2011.12003 Published Online December 2011 (http://www.SciRP.org/journal/aid) Copyright © 2011 SciRes. AID Protocol of Determining the Effect of Selenium Supplementation on CD4 + T Lymphocyte Count in HIV/AIDS Patients: A Randomized Double Blind Placebo Controlled Trial Sahar Yousefi1, Azar Hadadi2, Afshin Ostovar3, Behnaz Edalat Noor1, Mehrnaz Rasoolinejad4, Mahboobeh Haji Abdolbaghi4, Hossien Khalili5 1Tehran University of Medical Sciences, Tehran, Iran; 2Internal Medicine Ward, Sina Hospital, Iranian Research Center for HIV/AIDS, Tehran University of Medical Sciences, Tehran, Iran; 3School of Public Health Knowledge Utilization Research Centre, Tehran University of Medical Sciences, Tehran, Iran; 4Department of Infectious Diseases, Imam Khomeini Hospital, Iranian Re- search Center for HIV/AIDS, Tehran University of Medical Sciences, Tehran, Iran; 5Department of Clinical Pharmacy, School of Pharmacy, Tehran University of Medical Sciences, Tehran, Iran. Email: hadadiaz@tums.ac.ir, afshinostovar@yahoo.com, edalatnoor.behnaz@ymail.com, mehrnaz.rn@gmail.com, saharyousef@rocketmail.com, mahboubeh_hajiabdo@yahoo.com, khalilih@sina.tums.ac.ir Received August 29th, 2011; revised October 10th, 2011; accepted October 26th, 2011. ABSTRACT Background: Acquired immune deficiency syndrome (AIDS) is believed to be both among major epidemics and a criti- cal global health issue. The administration of antiretroviral therapy is recently proposed for all patients with CD4 + T cell count of ≤ 350/μlit in different studies. The accessibility of combination therapy has been restricted due to high costs of drugs, particularly in low and middle income countries. In Iran, according to WHO, drugs were distributed among only 6% of adults and 4% - 14% of children in 2009. Moreover, new strains are created and therefore, resis- tance to the current medication along with a considerable risk of ART-related toxic adverse effects points out the need for more affordable, effective and safer treatments. The use of antioxidants such as Selenium (Se) has been indicated to be beneficial in these patients. Method: In a double-blind randomized placebo control trial, 100 HIV positive, HAART-receiving patients will be selected from more than 2000 individuals covered under IRCHA (Iranian Referral HIV/AIDS Re- search Centre). They are then randomized to receive daily Se supplement of 200 μgr elemental Se and placebo for 6 months. The baseline assessment of the patients who meet the inclusion and exclusion criteria includes doing some lab tests to determine the absolute count of CD4 + T lymphocyte and the plasma levels of Se. The incidence of opportunistic infection will be assessed during the monthly visits in the first six months of the follow-up and the one performed at the end of the 9th month. For evaluating the trend of CD4 + T cells changes, the absolute count of CD4 + T lymphocyte will be measured every 3 months in the 5th, 8th, and 9th visits. The plasma levels of Se will be measured in the final follow-up session and compared with the baseline value. Keywords: Supplementation, HIV, AIDS, Lymphocyte Count, Randomized Clinical Trial 1. Introduction Acquired immune deficiency syndrome (AIDS) that is currently believed to be a critical global health problem [1]. According to WHO statistics (World Health Organi- zation), 33.3 million (31.4 - 35.3 million) people suffered from HIV worldwide in 2009. [2] Until 2008, the cumu- lative number of people died of AIDS was estimated to be more than 33 million [3]. The unpublished data in Iran until December 2009 show that 92.7% of the total 20547 HIV-infected individuals are male. From among this population, 2221 have been diagnosed with AIDS and 3543 died secondary to the complications. Recent studies suggest antiretroviral therapy for patients with CD4 + T cell count ≤ 350/μlit [4]. Despite the broader coverage of antiretroviral therapy since 2003 [5], more than 30 million people were diag- nosed with HIV in low and middle-income countries in 2009 [6] and from among them, only 36% with CD4 T cell count ≤ 350 /μlit received antiretroviral therapy in  Protocol of Determining the Effect of Selenium Supplementation on CD4 + T Lymphocyte Count in 21 HIV/AIDS Patients: A Randomized Double Blind Placebo Controlled Trial the same year [7]. Iranian the government offers free ART (antiretroviral therapy) to HIV and AIDS patients; the point is that only 6% of the adults and 4 to 14% of the children managed to receive the drugs regularly in 2009 [8]. Apart from the toxic effects of ART, the development of new strains of the virus and subsequently resistance to available medi- cations, especially in areas with acceptable coverage of the therapy, indicate that in addition to ART, other alter- native therapies are needed in this regard [9]. Many studies have reported that in a highly oxidative state, the progress of HIV infection can be promoted to the host [10]. Thus, treating the patients with antioxidants since early stages of the disease is believed to be benefi- cial. Selenium (Se) is a micronutrient with antioxidant and immunoregulatory properties [10]. According to the re- sults of several studies, lower serum Se levels correlates with a smaller total number of CD4 + T cells, more ad- vanced stages of infection and higher rates of mortality caused by HIV [13-21]. Many studies have pointed out the effect of depleted antioxidant agent-like glutathione peroxides- resources which is a result of HIV infection in promoting virus replication and CD4 + T cell count de- scent [22-24]. As the infection develops, serum Se con- centration diminishes progressively due to several causes including malabsorption caused by chronic infection, infectious diarrhea and HIV-related enteropathy, protein- calorie malnutrition and the inadequate intake of Se through diets [24,25]. Moreover, HIV contributes to the development of an enzyme with a glutathione peroxide- like structure—Se is a part of this enzyme structure— which comprises Se. Hypothetically, virus replication leads to the consumption of Se resources of infected T cells, through the development of the abovementioned enzyme [26]. There was a positive correlation between serum Se level and CD4 + T cell count, CD4 CD8 ratio and a negative correlation between this variable and indices of HIV infection progression, i.e. activity of Thymidine ki- nase and level of 2 microglobulin. There was also a positive correlation between serum Se concentration and hematocrit and serum albumin. In a cross sectional survey conducted in the Iranian re- search center for HIV/AIDS, Se deficiency (serum Se level < 85 μgr/lit) was reported in 38% of the HIV positive individuals. This is while a healthy male in the control group had significantly lower mean serum Se concentra- tions [19]. Not many researches have been trials with Se in humans (Table 1). Delmas-Beavieux chose 52 HIV positive patients randomly and supplied them with Se and beta carotene supplements and placebo daily for 12 months. They failed to report any improvement in CD4 + T cell count, as for the placebo group. However, glutathione levels—an antioxidant factor were significantly higher, whereas malondialdehyde levels—an indicator of lipid peroxidation were significantly lower in both treated groups [20]. In a clinical trial, 19 HIV and AIDS patients received 400 μgr Se supplements per day. After 70 days, some subjective improvements in the bowel function, appetite and severity of oral condidiasis as well as a de- cline in the incidence rate of opportunistic infections were achieved [21]. In another trial, taking Se supplements, which contained lower amounts of elemental Se (80μgr daily) for two months, significantly improved serum Se levels in HIV and AIDS patients; it, however, had no Table 1. Summary of clinical trials with Se. Studies in which administration of Se supplement led to an insignificant improvement in CD4 + T cell count. Studies in which administration of Se supplement led to a significant improvement in CD4 + T cell count. 1) Delmas-Beavieux supplied 52 HIV patients with 250 µgr Se or 30 mgr beta carotene for 12 months, no improvement in CD4 + T cell count was achieved. Gl utathione levels- an antioxidant factor were significantly higher, whereas malondialdehyde levels—an indicator of lipid peroxidation were significantly lower in both treated groups. 2) Cirelli administered 80 µgr Se and 25 mgr vit E to 11 HIV patients for two months. No improvement in CD4 + T cell count was achieved. 3) Look supplied 24 HIV patients with 600 mgr N-acetylcystein to- gether with 500 µgr Se for 24 weeks, no improvement was achieved in absolute CD4 + T cell count, but there was an increase in CD + T cell percentage and CD4 + T/CD8 + T cell ratio. 4) Burbano investigated the effect of 200 µgr daily Se supplement on CD4 + T cell count and hospital admissions of 186 HIV patients. No improvement was achieved in CD4 + T cell count, but there was a decrease in the rate of patients’ hospital admissions due to HIV com- plications. Hurwitz investigated the effect of 200 µgr daily Se supplement on CD4 + T cell count of 174 HIV patients for 9 months. In the end, there was a significant increase in CD4 + T cell count. Copyright © 2011 SciRes. AID  Protocol of Determining the Effect of Selenium Supplementation on CD4 + T Lymphocyte Count in 22 HIV/AIDS Patients: A Randomized Double Blind Placebo Controlled Trial effect on CD4 + T cell count, CD4 T CD8T ratio, serum al- bumin, hemoglobin or ESR (Erythrocyte sedimentation rate). Lower amounts of Se, compared to other similar trials, may have contributed to the finding [27]. Similarly, taking 200 μgr daily Se supplements for 2 years consid- erably improved Se levels but had no effect on CD4+T cell count. The number of patients with a decline in CD4 + T cell count of ≤50/μlit, however, was significantly greater in the placebo treated group (46% in contrast with 24% in Se treated group). Hospital admissions due to opportunistic infections were significantly more common in the placebo group (94% in contrast to 42% in the Se group) [28]. A recent trial, stressed that individuals who experienced an increase of at least 26μgr/lit in serum Se levels following the administration of 200μgr daily Se supplements for 9 months (Se responders) were more likely to have a higher CD4 + T count, but a lower viral load. Despite the fact that the effect of Se supplement on CD4 + T cell count was secondary to and a consequence of its impact on viral loud, there was no significant change in CD4 + T count in Se nonresponders and the placebo group [29]. In another trial, 24 asymptomatic HIV patients were supplied with 1800 mgr N-acetyl cys- tein along with 500 μgr Sodium Selenite daily. In the end, total CD8 + T cell count and its proportion decreased and the proportion of CD4 + T cell and CD4T cell count CD8T cell count ratio increased significantly. No improvement was achie- ved in CD4 + T cell absolute count. In 9 accidentally cho- sen patients, the number of HIV RNA copies/μlit did not differ; in 44% of them, however, this value was steady (no increase) after this time [30]. Considering the results of these studies, more documents regarding the beneficial effects of Se supplementation in HIV + /AIDS patients are needed. 2. Aim Determining the effect of Se supplementation on CD4 + T lymphocyte count in HIV patients 3. Objectives Determining the effects of Se supplementation on CD4 + T lymphocyte count in HIV patients; Body mass index (BMI) values of HIV patients; Hb levels of HIV patients; The rate of developing opportunistic infections in HIV patients. 4. Study Population From among 2000 HIV + /AIDS patients covered under the Iranian Research Center for HIV/AIDS (IRCHA), one hundred HIV seropositive HAART-receiving individuals will be selected. IRCHA, located in Imam Khomeini hospital in Tehran is working under the supervision of Tehran University of Medical Sciences. It offers free services such as para-clinical and clinical treatment and consultation to about 2000 HIV positive individuals as well as others at risk of developing HIV or any other sexually transmitted disease. 5. Recruitment Subjects of the study consist of individuals diagnosed with HIV through Western blotting test. Eligible patients meeting the inclusion criteria will be recruited and the others will be excluded (see Table 2). We will recruit 100 HIV infected patients with either sufficient or inadequate serum levels of Se (the deficiency criterion is having serum Selenium levels of 85 µg/dl or lower). A detailed written explanation of the study process, names of indi- viduals and institutions in charge, possible benefits and probable adverse effects of the interventions is given to the participants and additional information would be pro- vided upon request. Informed participants will be asked to sign a written informed consent. After baseline as- sessment completion and signing the informed consent, all patients will be randomized based on age, sex, HIV infection and AIDS by permuted block randomization with 4 numbers block into two groups, each consisting of 50 HIV positive patients. One group will receive placebo, whereas the other will receive Se supplements. The patients and the researchers are both blinded (see Figure 1). 6. Baseline Assessments In their first visit all participants are required to complete a questionnaire on their demographic information, route Table 2. Inclusion and exclusion criteria. Inclusion Criteria Age 18 to 60 years Confirmed HIV-1 infection with western blotting test Signing an informed written consent Receiving HAART treatment Exclusion criteria Pregnancy Consumption of any other supplements except for those under investigation in the present study History of Hypersensitivity reaction to Se supplement History of chronic kidney disease or cirrhosis Active HBV infection with liver enzyme > 100 unit/µlit of serum Acute or chronic diarrhea or any acute illness with anorexia Copyright © 2011 SciRes. AID 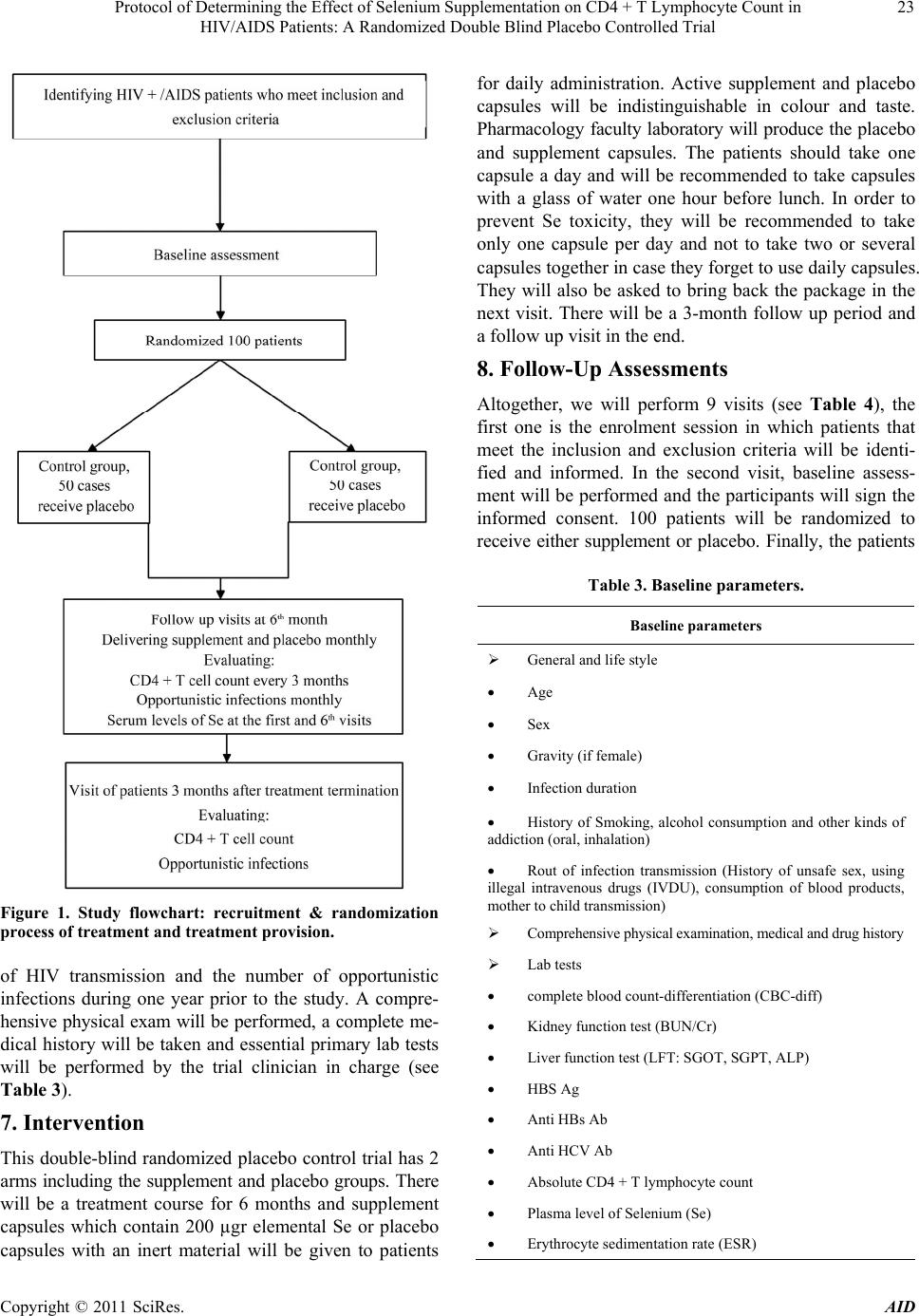 Protocol of Determining the Effect of Selenium Supplementation on CD4 + T Lymphocyte Count in 23 HIV/AIDS Patients: A Randomized Double Blind Placebo Controlled Trial Figure 1. Study flowchart: recruitment & randomization process of treatment and treatment provision. of HIV transmission and the number of opportunistic infections during one year prior to the study. A compre- hensive physical exam will be performed, a complete me- dical history will be taken and essential primary lab tests will be performed by the trial clinician in charge (see Table 3). 7. Intervention This double-blind randomized placebo control trial has 2 arms including the supplement and placebo groups. There will be a treatment course for 6 months and supplement capsules which contain 200 µgr elemental Se or placebo capsules with an inert material will be given to patients for daily administration. Active supplement and placebo capsules will be indistinguishable in colour and taste. Pharmacology faculty laboratory will produce the placebo and supplement capsules. The patients should take one capsule a day and will be recommended to take capsules with a glass of water one hour before lunch. In order to prevent Se toxicity, they will be recommended to take only one capsule per day and not to take two or several capsules together in case they forget to use daily capsules. They will also be asked to bring back the package in the next visit. There will be a 3-month follow up period and a follow up visit in the end. 8. Follow-Up Assessments Altogether, we will perform 9 visits (see Table 4), the first one is the enrolment session in which patients that meet the inclusion and exclusion criteria will be identi- fied and informed. In the second visit, baseline assess- ment will be performed and the participants will sign the informed consent. 100 patients will be randomized to receive either supplement or placebo. Finally, the patients Table 3. Baseline parameters. Baseline parameters General and life style Age Sex Gravity (if female) Infection duration History of Smoking, alcohol consumption and other kinds of addiction (oral, inhalation) Rout of infection transmission (History of unsafe sex, using illegal intravenous drugs (IVDU), consumption of blood products, mother to child transmission) Comprehensive physical examination, medical and drug history Lab tests complete blood count-differentiation (CBC-diff) Kidney function test (BUN/Cr) Liver function test (LFT: SGOT, SGPT, ALP) HBS Ag Anti HBs Ab Anti HCV Ab Absolute CD4 + T lymphocyte count Plasma level of Selenium (Se) Erythrocyte sedimentation rate (ESR) Copyright © 2011 SciRes. AID 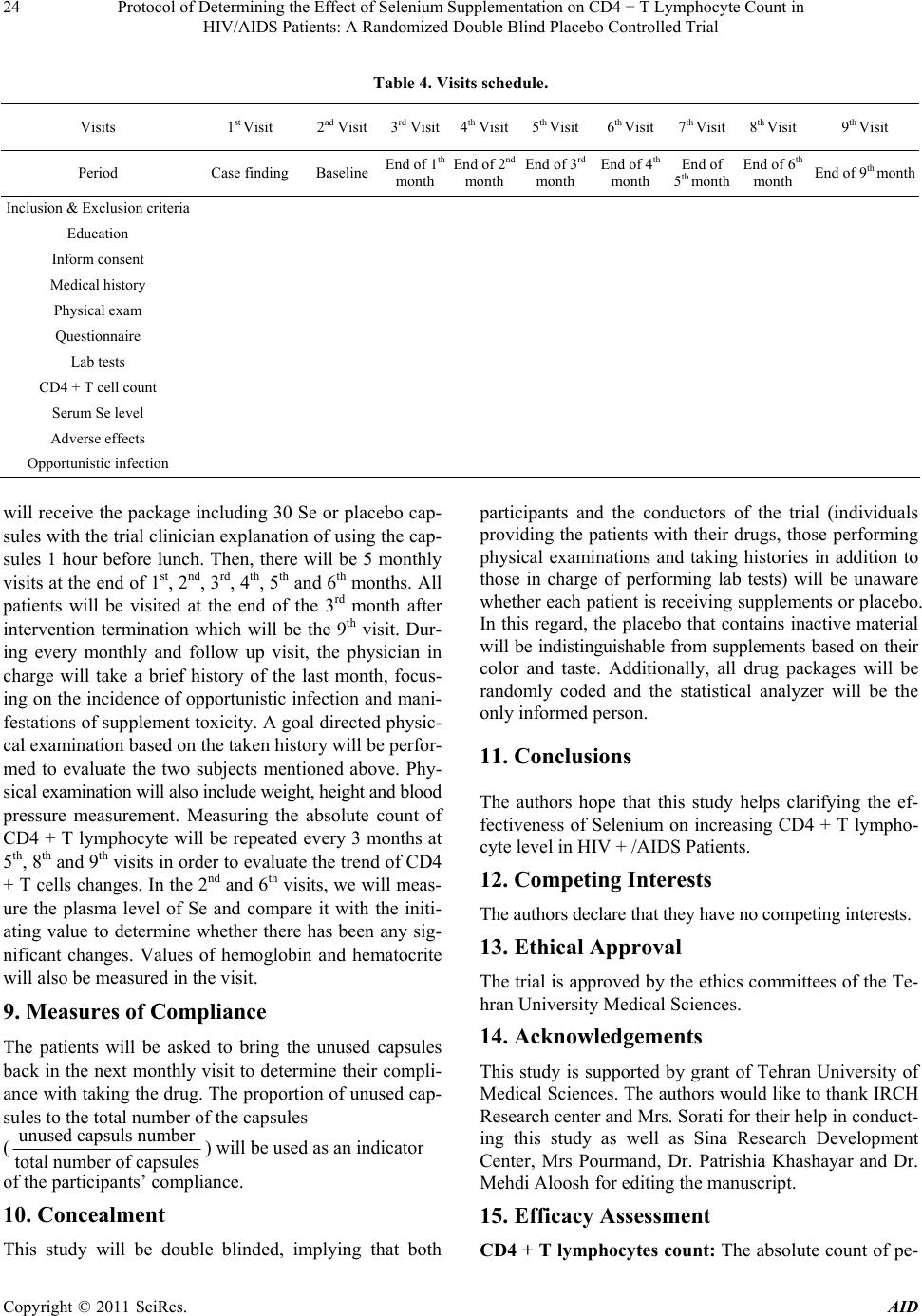 Protocol of Determining the Effect of Selenium Supplementation on CD4 + T Lymphocyte Count in HIV/AIDS Patients: A Randomized Double Blind Placebo Controlled Trial Copyright © 2011 SciRes. AID 24 Table 4. Visits schedule. Visits 1st Visit 2nd Visit3rd Visit4th Visit5th Visit 6th Visit 7th Visit 8th Visit 9th Visit Period Case finding BaselineEnd of 1th month End of 2nd month End of 3rd month End of 4th month End of 5th month End of 6th month End of 9th month Inclusion & Exclusion criteria Education Inform consent Medical history Physical exam Questionnaire Lab tests CD4 + T cell count Serum Se level Adverse effects Opportunistic infection will receive the package including 30 Se or placebo cap- sules with the trial clinician explanation of using the cap- sules 1 hour before lunch. Then, there will be 5 monthly visits at the end of 1st, 2nd, 3rd, 4th, 5th and 6th months. All patients will be visited at the end of the 3rd month after intervention termination which will be the 9th visit. Dur- ing every monthly and follow up visit, the physician in charge will take a brief history of the last month, focus- ing on the incidence of opportunistic infection and mani- festations of supplement toxicity. A goal directed physic- cal examination based on the taken history will be perfor- med to evaluate the two subjects mentioned above. Phy- sical examination will also include weight, height and blood pressure measurement. Measuring the absolute count of CD4 + T lymphocyte will be repeated every 3 months at 5th, 8th and 9th visits in order to evaluate the trend of CD4 + T cells changes. In the 2nd and 6th visits, we will meas- ure the plasma level of Se and compare it with the initi- ating value to determine whether there has been any sig- nificant changes. Values of hemoglobin and hematocrite will also be measured in the visit. 9. Measures of Compliance The patients will be asked to bring the unused capsules back in the next monthly visit to determine their compli- ance with taking the drug. The proportion of unused cap- sules to the total number of the capsules (unused capsuls number total number of capsules) will be used as an indicator of the participants’ compliance. 10. Concealment This study will be double blinded, implying that both participants and the conductors of the trial (individuals providing the patients with their drugs, those performing physical examinations and taking histories in addition to those in charge of performing lab tests) will be unaware whether each patient is receiving supplements or placebo. In this regard, the placebo that contains inactive material will be indistinguishable from supplements based on their color and taste. Additionally, all drug packages will be randomly coded and the statistical analyzer will be the only informed person. 11. Conclusions The authors hope that this study helps clarifying the ef- fectiveness of Selenium on increasing CD4 + T lympho- cyte level in HIV + /AIDS Patients. 12. Competing Interests The authors declare that they have no competing interests. 13. Ethical Approval The trial is approved by the ethics committees of the Te- hran University Medical Sciences. 14. Acknowledgements This study is supported by grant of Tehran University of Medical Sciences. The authors would like to thank IRCH Research center and Mrs. Sorati for their help in conduct- ing this study as well as Sina Research Development Center, Mrs Pourmand, Dr. Patrishia Khashayar and Dr. Mehdi Aloosh for editing the manuscript. 15. Efficacy Assessment CD4 + T lymphocytes count: The absolute count of pe-  Protocol of Determining the Effect of Selenium Supplementation on CD4 + T Lymphocyte Count in 25 HIV/AIDS Patients: A Randomized Double Blind Placebo Controlled Trial ripheral blood CD4 + T lymphocytes is measured by flowcytometric method Opportunistic infections: all infectious diseases and malignancies detected in immune compromised individu- als like HIV infected individuals and is rare with normal immune system function and is clinically or par clinically diagnosed. In our study, these would be HSV infection, mycobacterial infections, Hairy leukoplakia, oral can- didiasis, recurrent bacterial pneumonia, Kaposi’s sar- coma and cervical cancer. BMI: An index which is explained in 2 weight kg height(m) , the measuring accuracy would be 0.01. Hemoglobin: Blood tetrapyrrolic protein which car- ries O2 and is measured in gr/dl. REFERENCES [1] Understanding HIV/AIDS, Nantional Institute of Allergy and Infectious Diseases. http://www.niaid.nih.gov/topics/hivaids/understanding/Pa ges/Default.aspx [2] WHO: Global Summary of AIDS Epidemic, 2009. http://www.who.int/hiv/data/2009_global_summary.png [3] How HIV Causes AIDS, National Nantional Institute of Allergy and Infectious Diseases. http://www.niaid.nih.gov/topics/HIVAIDS/Understanding /howHIVCausesAIDS/Pages/howhiv.aspx [4] S. M. Hammer, J. Eron Jr, P. Reiss, R. T. Schooley, M. A. Thompson, S. Walmsley, P. Cahn, M. A. Fischl, J. M. Gatell and M. S. Hirsch, “Antiretroviral Treatment of Adult HIV Infection: Recommendations of the Interna- tional AIDS Society-USA Panel,” Journal of the Ameri- can Medical Association, Vol. 300, No. 5, 2008, p. 555. doi:10.1001/jama.300.5.555 [5] WHO: HIV/AIDS. http://www.who.int/features/qa/71/en/index.html [6] WHO: Classification of Low- and Middle-Income Coun- tries by Income Level, Epidemic Level, and Geographical UNAIDS, UNICEF and WHO Regions. http://www.who.int/hiv/data/tuapr2010_annex7.xls [7] WHO: Treated Patients in Low- and Middle-Income Countries by Income Level, Epidemic Level, and Geo- graphical UNAIDS, UNICEF and WHO Regions. http://www.who.int/hiv/data/tuapr_2010_figures_slideset. pps [8] WHO: Reported Number of People Receiving Antiretro- viral Therapy in Low- and Middle-Income Countries by Sex and by Age, and Estimated Number of Children Re- ceiving and Needing Antiretroviral Therapy and Cover- age Percentages, 2009. http://www.who.int/hiv/data/tuapr2010_annex4.xls [9] Adherence and Drug Resistance, Nantional Institute of Allergy and Infectious Diseases. http://www.niaid.nih.gov/topics/HIVAIDS/Understanding /Treatment/Pages/adherence.aspx [10] L. Patrick, “Nutrients and HIV: Part One—Beta Carotene and Selenium,” Alternative Medicine Review: A Journal of Clinical Therapeutic, Vol. 4, No. 6, 1999, p. 403. [11] K. Schwarz and C. M. Foltz, “Selenium as an Integral Part of Factor 3 against Dietary Necrotic Liver Degenera- tion,” Journal of the American Chemical Society, Vol. 79, No. 12, 1957, pp. 3292-3293. doi:10.1021/ja01569a087 [12] P. R. Hoffmann and M. J. Berry, “The Influence of Sele- nium on Immune Responses,” Molecular Nutrition & Food Research, Vol. 52, No. 11, 2008, pp. 1273-1280. doi:10.1002/mnfr.200700330 [13] M. P. Look, J. K. Rockstroh, G. S. Rao, K. A. Kreuzer, U. Spengler and T. Sauerbruch, “Serum Selenium Versus Lymphocyte Subsets and Markers of Disease Progression and Inflammatory Response in Human Immunodeficiency Virus-1 Infection,” Biological Trace Element Research, Vol. 56, No. 1, 1997, pp. 31-41. doi:10.1007/BF02778982 [14] M. K. Baum, G. Shor-Posner, S. Lai, G. Zhang, H. Lai, M. A. Fletcher, H. Sauberlich and J. B. Page, “High Risk of HIV-Related Mortality is Associated with Selenium De- ficiency,” Journal of Acquired Immune Deficiency Syn- dromes, Vol. 15, No. 5, 1997, p. 370. doi:10.1097/00042560-199708150-00007 [15] R. Kupka, G. I. Msamanga, D. Spiegelman, S. Morris, F. Mugusi, D. J. Hunter and W. W. Fawzi, “Selenium Status is Associated with Accelerated HIV Disease Progression among HIV-1-Infected Pregnant Women in Tanzania,” The Journal of Nutrition, Vol. 134, No. 10, 2004, p. 2556. [16] C. B. Stephensen, G. S. Marquis, S. D. Douglas, L. A. Kruzich and C. M. Wilson, “Glutathione, Glutathione Peroxidase, and Selenium Status in HIV-Positive and HIV-Negative Adolescents and Young Adults,” The American Journal of Clinical Nutrition, Vol. 85, No. 1, 2007, p. 173. [17] G. Shor-Posner, M. J. Miguez, L. M. Pineda, A. Rodri- guez, P. Ruiz, G. Castillo, X. Burbano, R. Lecusay and M. Baum, “Impact of Selenium Status on the Pathogenesis of Mycobacterial Disease in HIV-1-Infected Drug Users during the Era of Highly Active Antiretroviral Therapy,” Journal of Acquired Immune Deficiency Syndromes, Vol. 29, No. 2, 2002, p. 169. [18] J. Constans, J. L. Pellegrin, C. Sergeant, M. Simonoff, I. Pellegrin, H. Fleury, B. Leng and C. Conri, “Serum Sele- nium Predicts Outcome in HIV Infection,” Journal of Acquired Immune Deficiency Syndromes, Vol. 10, No. 3, 1995, p. 392. doi:10.1097/00042560-199511000-00015 [19] H. Khalili, A. Soudbakhsh, M. Hajiabdolbaghi, S. Dashti- Khavidaki, A. Poorzare, A. Saeedi and R. Sharififar, “Nu- tritional Status and Serum Zinc and Selenium Levels in Iranian HIV Infected Individuals,” BMC Infectious Dis- eases, Vol. 8, No. 1, 2008, p. 165. doi:10.1186/1471-2334-8-165 [20] M. C. Delmas-Beauviaux, E. Peuchant, A. Couchouron, J. Constans, C. Sergeant, M. Simonoff, J. L. Pellegrin, B. Leng, C. Conri and M. Clerc, “The Enzymatic Antioxi- dant System in Blood and Glutathione Status in Human Copyright © 2011 SciRes. AID  Protocol of Determining the Effect of Selenium Supplementation on CD4 + T Lymphocyte Count in HIV/AIDS Patients: A Randomized Double Blind Placebo Controlled Trial Copyright © 2011 SciRes. AID 26 Immunodeficiency Virus (HIV)-Infected Patients: Effects of Supplementation with Selenium or Carotene,” Ameri- can Journal of Clinical Nutrition, Vol. 64, No. 1, 1996, pp. 101-107. [21] L. Olmsted, G. N. Schrauzer, M. Flores-Arce and J. Dowd, “Selenium Supplementation of Symptomatic Hu- man Immunodeficiency Virus Infected Patients,” Bio- logical Trace Element Research, Vol. 20, No. 1, 1989, pp. 59-65. doi:10.1007/BF02919098 [22] P. A. Sandstrom, J. Murray, T. M. Folks and A. M. Dia- mond, “Antioxidant Defenses Influence HIV-1 Replica- tion and Associated Cytopathic Effects,” Free Radical Biology and Medicine, Vol. 24, No. 9, 1998, pp. 1485-1491. doi:10.1016/S0891-5849(98)00023-9 [23] M. Kameoka, T. Kimura and K. Ikuta, “Superoxide En- hances the Spread of HIV-1 Infection by Cell-To-Cell Transmission,” FEBS Letters, Vol. 331, No. 1-2, 1993, pp. 182-186. doi:10.1016/0014-5793(93)80322-L [24] W. Dröge, H. P. Eck, H. Gmünder and S. Mihm, “Re- quirement for Prooxidant and Antioxidant States in T Cell Mediated Immune Responses—Relevance for the Patho- genetic Mechanism of AIDS?” Journal of Molecular Medicine, Vol. 69, No. 21, 1991, pp. 1118-1122. [25] B. E. Hurwitz, N. G. Klimas, M. M. Llabre, K. J. Maher, J. S. Skyler, M. S. Bilsker, S. McPherson-Baker, P. J. Lawrence, A. R. LaPerriere and J. M. Greeson, “HIV, Metabolic Syndrome X, Inflammation, Oxidative Stress, and Coronary Heart Disease Risk,” Cardiovascular Toxi- cology, Vol. 4, No. 3, 2004, pp. 303-315. doi:10.1385/CT:4:3:303 [26] E. W. Taylor, R. G. Nadimpalli and C. S. Ramanathan, “Genomic Structures of Viral Agents in Relation to the Biosynthesis of Selenoproteins,” Biological Trace Ele- ment Research, Vol. 56, No. 1, 1997, pp. 63-91. doi:10.1007/BF02778984 [27] A. Cirelli, M. Ciardi, C. De Simone, F. Sorice, R. Giordano, L. Ciaralli and S. Costantini, “Serum Selenium Concentration and Disease Progress in Patients with HIV Infection,” Clinical Biochemistry, Vol. 24, No. 2, 1991, pp. 211-214. doi:10.1016/0009-9120(91)90601-A [28] X. Burbano, M. Miquez-Burbano, K. McCollister, G. Zhang, A. Rodriguez, P. Ruiz, R. Lecusay and G. Shor-Posner, “Impact of a Selenium Chemoprevention Clinical Trial on Hospital Admissions of HIV-Infected Participants,” HIV Clinical Trials, Vol. 3, No. 6, 2002, pp. 483-491. doi:10.1310/A7LC-7C9V-EWKF-2Y0H [29] B. E. Hurwitz, J. R. Klaus, M. M. Llabre, A. Gonzalez, P. J. Lawrence, K. J. Maher, J. M. Greeson, M. K. Baum, G. Shor-Posner and J. S. Skyler, “Suppression of Human Immunodeficiency Virus Type 1 Viral Load with Sele- nium Supplementation,” Arch International Medicine, Vol. 167, 2007, pp. 148-154. doi:10.1001/archinte.167.2.148 [30] M. P. Look, J. Rockstroh, G. Rao, S. Barton, H. Lemoch, R. Kaiser, B. Kupfer, T. Sudhop, U. Spengler and T. Sau- erbruch, “Sodium Selenite and N-Acetylcysteine in An- tiretroviralnaive HIV-1-Infected Patients: A Randomized, Controlled Pilot Study,” European Journal of Clinical Investigation, Vol. 28, No. 5, 1998, pp. 389-397. doi:10.1046/j.1365-2362.1998.00301.x
|