A. Meberg et al. / Open Journal of Pediatrics 1 (2011) 45-50 49
Most of the patients with hypothermia (body tem-
perature <36˚C) at arrival were low birthweight infants,
caused by insufficient temperature regulation and in-
creased heat loss because of a large body surface to
weight ratio in these patients. Our experiences are in
agreement with other studies [8]. Temperature monitor-
ing, best performed continuously with a rectal probe,
thus is an important procedure in neonatal transports.
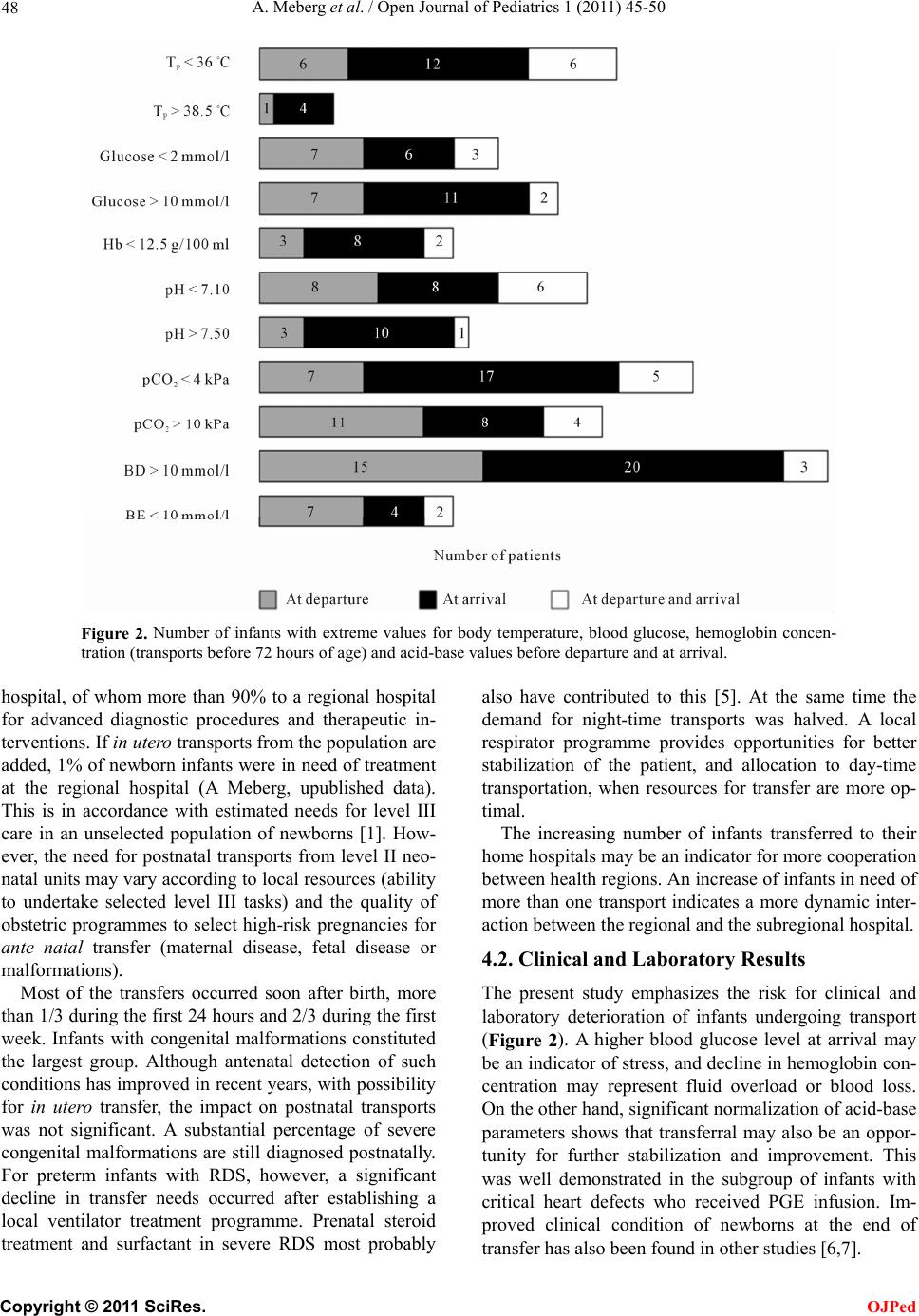
There was a trend for more infants with extreme val-
ues for body temperature, blood glucose, hemoglobin,
and acid-base parameters at arrival (Figure 2). It is a
matter of concern that some patients with extreme values
at departure also had extreme values at arrival. This sug-
gests insufficient stabilization, or that the condition
could not be stabilized. When a specialized retrieval
team carries out the transport, the quality of transports
has been shown to be improved compared to local ad
hoc teams [9,10]. A special challenge is pulmonary hy-
pertension, causing severe hypoxia and metabolic acido-
sis. The risk for death or sequelae is high in these pa-
tients, who may need ventilation with nitric oxide to
reduce pulmonary vascular resistance [11] or extractor-
poral membrane oxygenation to ensure oxygenation [12].
Few hospitals have the possibility to provide such treat-
ment during transport, and will need help from sentral-
ized transport systems with advanced technology.
4.3. Technical Mishaps
Technical errors occurred in some of the transports. This
emphasizes the importance of a high-quality work with
focus on technical details, especially in the pretransport
stabilization period. Proper fixation of the tracheal tube,
X-ray control of tube position and necessary correction
before departure, sedation of active infants (e.g. when
mechanically ventilated) are important points in order to
avoid tube dislocation. The same principles apply for
umbilical vessel catheters.
4.4. Mortality
The transport-related mortality (dead during the first 24
hours after arrival) was low (3%), with nearly half dying
from letal malformations. Better diagnostics could pos-
sibly have avoided some of these futile transports.
A considerable decline in mortality of transported in-
fants occurred without contemporary increasing mortal-
ity in the referring hospital (A Meberg, unpublished
data). The reason for this is multifactorial, reflecting
progress of neonatal care. Better organization of trans-
ports, and better stabilization and treatment of the pa-
tients are important factors. An indicator for this may be
the reduced percentage of night-time transports follow-
ing improvements in the local intensive care programme.
However, in spite of high quality postnatal transports, in
utero transfer is, when possible, the better choice [13,
14].
5. CONCLUSIONS
Neonatal transport carries risks, but also an opportunity
for further stabilization and improvement. A local respi-
rator programme reduced the need for transfer of pre-
mature infants with RDS as well as for transports during
night-time.
6. ACKNOWLEDGEMENTS
The study was supported by a grant from Vestfold Hospital Trust.
REFERENCES
[1] Neonatal Care in Norway (1990) Helsedirektoratets
utredningsserie nr. 2/1990. The Norwegian Health Di-
rectorate, Oslo.
[2] Mohamed, M.A. and Aly, H. (2010) Transport of prema-
ture infants is associated with increased risk for intraven-
tricular haemorrhage. Archives of Disease in Childhood
Fetal Neonatal Edition, 95, F403-F407.
doi:10.1136/adc.2010.183236
[3] Lang, A., Brun, H., Kaaresen, P.I. and Klingenberg, C.
(2007) A population based 10-year study of neonatal air
transport in North Norway. Acta Paediatrica, 96, 995-
999. doi:10.1111/j.1651-2227.2007.00320.x
[4] Shenai, J.P., Major, C.W., Gaylord, M.S., Blake, W.W.,
Simmons, A., Oliver, S., et al. (1991) A successful dec-
ade of regionalized perinatal care in Tennessee: The
neonatal experience. Journal of Perinatology, 11, 137-
143.
[5] Mildenhall, L.F.J., Pavuluri, N.N. and Bowman, E.D.
(1999) Safety of synthetic surfactant use before preterm
newborn transport. Journal of Paediatrics and Child
Health, 35, 530-535.
doi:10.1046/j.1440-1754.1999.00414.x
[6] Hellström-Westas, L., Hanséus, K., Jögi, P,. Lundström,
N.R. and Svenningsen, N. (2001) Long-distance trans-
ports of newborn infants with congenital heart disease.
Pediatric Cardiology, 22, 380-384.
[7] Mullane, D., Byrne, H., Clarke, T.A., Gorman, W.,
Griffin, E., Ramesh, K., et al. (2004) Neonatal transpor-
tation: The effects of a national neonatal transportation
programme. Irish Journal of Medical Science, 173, 105-
108. doi:10.1007/BF02914569
[8] Holt, J. and Fagerli, I. (1999) Air transport of the sick
newborn infant: Audit from a sparsely populated county
in Norway. A cta Pædiatrica, 88, 66-71.
doi:10.1111/j.1651-2227.1999.tb01271.x
[9] Yoder, B.A. (1992) Long distance perinatal transport.
American Journal of Perinatology, 9, 75-79.
doi:10.1055/s-2007-994675
[10] Arrøe, M., Steensgård, J. and Greisen, G. (2001) Emer-
gency transport of new-born infants—Fetch or bring?
Ugeskrift for Læger, 163, 1093-1097.
[11] Kinsella, J.P. (1995) Inhaled nitric oxide treatment for
stabilization and emergency medical transport of criti-
cally ill newborns and infants. Pediatrics, 95, 773-776.
C
opyright © 2011 SciRes. OJPed