D. Can et al. / Open Journal of Pediatrics 1 (2011) 90-93
92
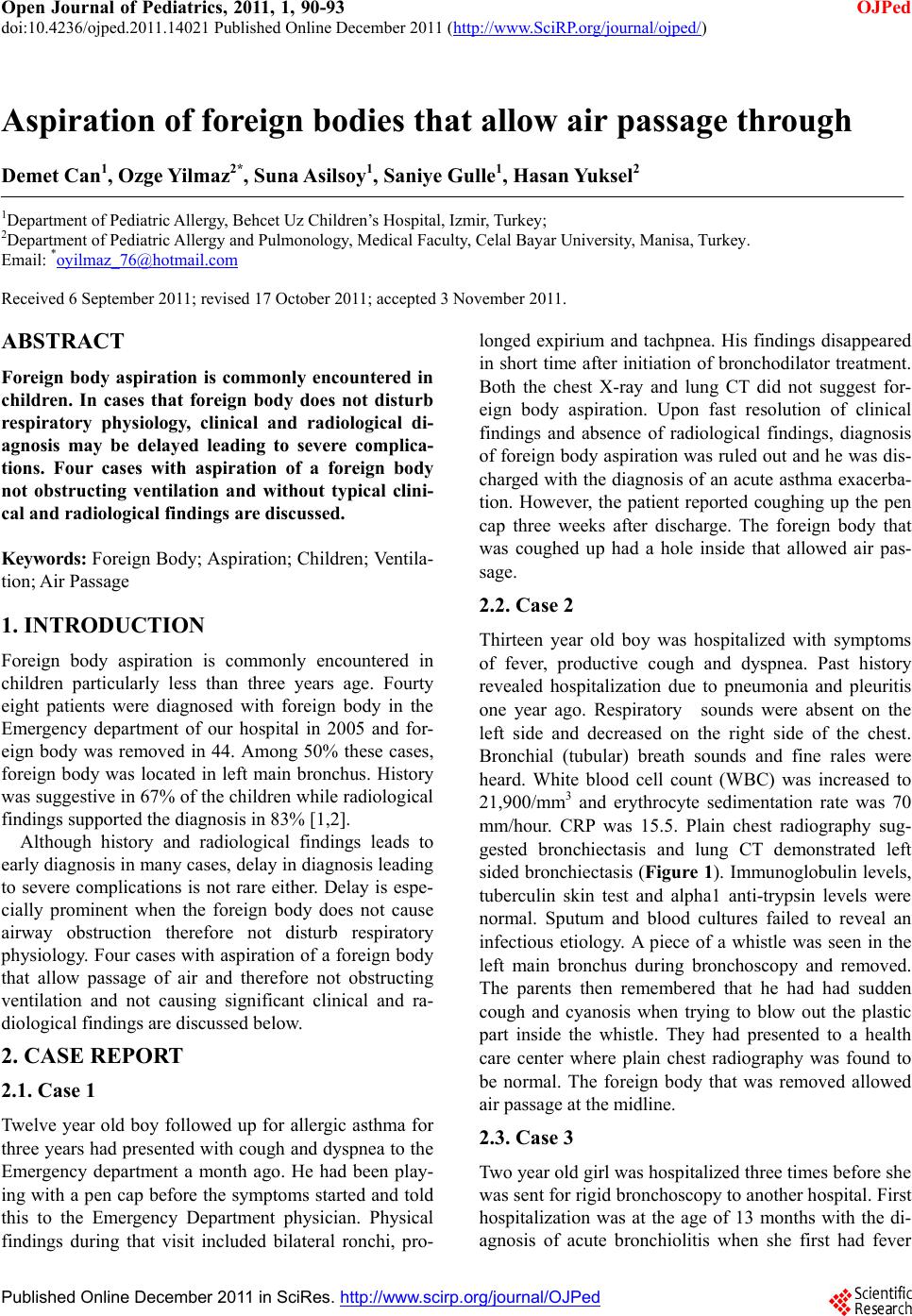
shift. Bronchial wall irregularity was seen in the seg-
mental bronchus of the right upper lobe anterior segment
and main bronchus of the right middle lobe. Flexible
fiberoptic bronchoscopy was performed for diagnostic
purposes and foreign body lodged right below enterance
of right middle lobe was suspected. Pediatric surgery
was called in during the same session for rigid broncho-
scopy since the patient had received general anesthesia.
They could not reach the foreign body in that session
and interpreted the image as granulation tissue. However,
upon questioning of the family again for foreign body
aspiration, the child remembered swallowing a plastic
pencil tip seven years ago. They had presented to a phy-
sician but aspiration was not thought at that time because
plain radiography was normal. Upon this information,
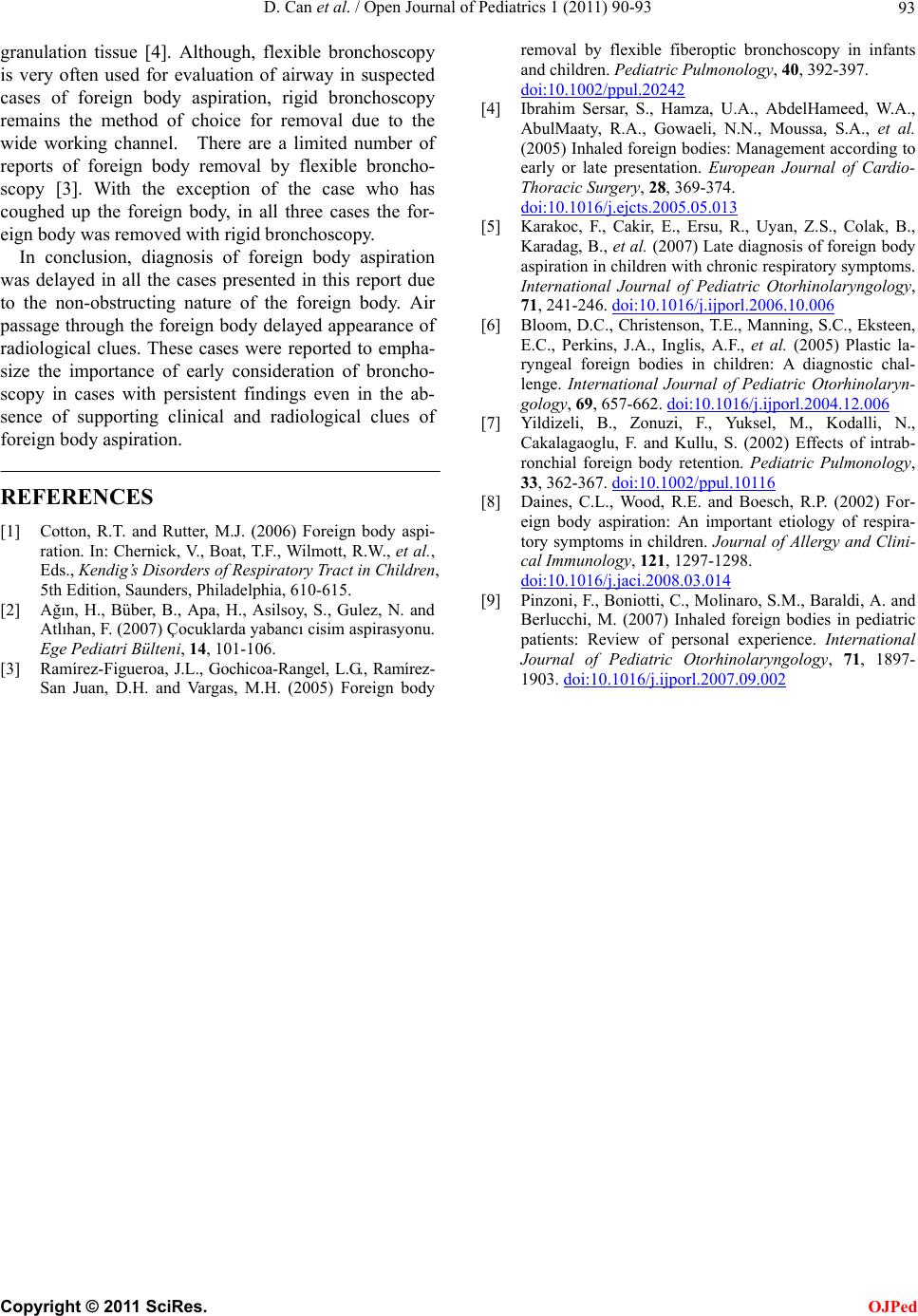
rigid bronchoscopy was performed once again and the
foreign body was removed (Fi gure 3).
3. DISCUSSION
Foreign body aspiration that is most commonly encoun-
tered in pre-school children, is a life threatening emer-
gency, however, it may go unrecognized for prolonged
periods of time due to vague clinical and radiological
findings in some cases [3,4]. Considering that most
commonly aspirated foreign bodies in children include
organic material including peanuts not causing complete
obstruction, careful evaluation is especially important
for prompt diagnosis [3].
Aspiration of a foreign body may result in immediate
choking when lodged in larynx or may lead to complete
obstruction of air entry into a lung segment [5,6]. Re-
tained foreign body in the airway leads to local me-
chanical effects, chemical reactions and inflammation.
An animal study has demonstrated that initial reaction to
the presence of foreign body in the airway is polymer-
phonuclear leukocyte infiltration and edema which is
followed by mononuclear leukocyte and macrophage
infiltration. These findings have been interpreted as ini-
tiation of acute inflammation as early as three days after
aspiration and progression to chronic inflammation as
Figure 3. Foreign body aspirated by case 4.
early as ten days. Moreover, bronchiectatic changes were
observed when a month has passed after aspiration [7].
Presenting symptoms of foreign body aspiration may
vary from vague to specific and include cough, wheeze,
dyspnea and fever. Physical examination may reveal
focal wheezing or decreased air entry but the findings
may also reveal generalized wheezing or it may be com-
pletely normal [8]. Similarly plain radiographs of chest
may reveal unilateral hyperinflation, atelectasis, con-
solidation or mediastinal shift if there is complete ob-
struction of airflow by the foreign body or they may be
normal especially if there is no obstruction to airflow [5,
8]. Therefore, it is impossible to exclude diagnosis of
foreign body aspiration with a normal radiograph [9]. In
the presented cases, two of them had findings suggestive
of bronchiectasis in plain radiographs which was con-
firmed by computerized tomography (CT). Two patients
had normal plain radiography findings. One of the latter
two had persistent findings on physical examination and
therefore underwent CT that demonstrated focal atelec-
tasis.
Diagnosis of foreign body aspiration is usually sug-
gested with clinical history and radiological findings [3].
Foreign body is encountered only in 5% of cases that
undergo flexible bronchoscopy without a prior suspicion
of aspiration [3,5]. Considering that early removal of
aspirated foreign bodies is necessary to avoid the patho-
logical progress from inflammation that initiates at third
day to development of bronchiectasis after 30 days, high
suspicion even in cases with vague clinical or radiologi-
cal findings is required [7,8]. Four cases presented in
this report highlight the importance of aspiration of for-
eign bodies that do not cause complete obstruction since
these cases may easily be overlooked and bronchoscopy
may be delayed. In three of these cases clinical findings
were not suggestive of foreign body aspiration due to the
nature of the foreign body that allowed air passage. One
patient was lucky to cough up the aspirated material but
the other three presented with bronchiectasis, pneumonia
or bronchoconstriction findings [8]. Although the clini-
cal findings may be milder without complete airway
obstruction, induction of inflammation is still expected
to progress thus making early and prompt diagnosis es-
sential for prevention of complications. Therefore, high
clinical suspicion and use of flexible bronchoscopy as
the initial technique of evaluation in patients with sus-
pected foreign body aspiration is prompted. Moreover,
Flexible bronchoscopy provides detailed information
about the nature and localization of the foreign body as
well as the characteristics of airway mucosa [3].
Detection of a foreign body aspirated into the airway
should be followed by removal as soon as possible to
prevent the inflammatory reaction and development of
C
opyright © 2011 SciRes. OJPed