Paper Menu >>
Journal Menu >>
 Psychology, 2010, 1: 9-16 doi:10.4236/psych.2010.11002 Published Online April 2010 (http://www.SciRP.org/journal/psych) Copyright © 2010 SciRes PSYCH 9 Sensitivity and Specificity of the CDC Empirical Chronic Fatigue Syndrome Case Definition Leonard A. Jason, Meredyth Evans, Abigail Brown, Molly Brown, Nicole Porter, Jessica Hunnell, Valerie Anderson, Athena Lerch DePaul University, Chicago, American. Email: Ljason@depaul.edu Received February 10th, 2010; revised March 7th, 2010; accepted March 8th, 2010. ABSTRACT In an effort to bring mo re standardization to the chron ic fatigue syndrome (CFS) Fukuda et al. case definition [1], the Centers for Disease Control and Prevention (CDC) has developed an empirical case definition [2] that specifies crite- ria and instruments to diagnose CFS. The pr esent study investiga ted the sens itivity and specificity o f this CFS emp irical case definition with diagnosed individuals with CFS from a community based study that were compared to non-CFS cases. All participants completed questionnaires measuring disability (Medical Outcome Survey Short-Form-36) [3], fatigue (the Multidimensional Fatigue Inventory) [4], and symptoms (CDC Symptom Inventory) [5]. Findings of the present study indica ted sensitivity and specificity problems with the CDC empirical CFS case definition. Keywords: Chronic Fatigue Syndrome, Empirical Case Definition, Centers for Disease Control and Prevention, Fukuda Criteria 1. Sensitivity and Specificity of the CDC Empirical Case Definiti on The Centers for Disease Control and Prevention (CDC) has developed an empirical case definition for chronic fatigue syndrome (CFS) that involves assessment of symptoms, disability, and fatigue [2]. The CDC empiri- cal CFS case definition assesses three specific areas to determine whether a person meets criteria for this illness including: 1) disability, using the Medical Outcomes Survey Short Form-36 (SF-36) [3], 2) fatigue, using the Multidimensional Fatigue Inventory (MFI) [4], and 3) symptoms, using the CDC Symptom Inventory (SI) [5]. The authors of this empirical case definition feel that the specification of instruments and cut-off points will result in a more reliable and valid approach for the assessment of CFS. The disability criterion for the Reeves et al. empirical CFS case definition [2] would be met by scoring below the 25th percentile on any one of the following four SF-36 sub-scales [3]: Physical Functioning (less than or equal to 70), Role Physical (less than or equal to 50), Social Functioning (less than or equal to 75), or Role Emotional (less than or equal to 66.7). Because a person could meet the disability criterion for the empirical CFS case definition by only showing impairment in one or more of these four areas, a person could meet the disabil- ity CFS criterion by only having an impairment in role emotional areas (e.g., problems with work or other daily activities as a result of emotional problems). Ware et al. [3] found that the mean for Role Emotional for a clinical depression group was 38.9, indicating that almost all those with clinical depression would meet the CFS dis- ability criterion, as they would be within the lower 25th percentile on this sub-scale. To meet the fatigue criterion, the Reeves et al. empiri- cal case definition [2] requires a score on the MFI [4] of greater than or equal to 13 on the General Fatigue sub- scale, or greater than or equal to 10 on the Reduced Ac- tivity sub-scale. In one study of three groups with CFS [6], the mean MFI General Fatigue scores ranged from 18.3 to 18.8 and these scores are clearly higher than the Reeves et al. cutoff of 13. In addition, Reduced Activity items refer to issues that a person with depression might easily endorse. If a person indicated that the following two items were entirely true: “I get little done,” and “I think I do very little in a day”; they would meet criterion for fatigue on this sub-scale. The SI [5] assesses information about the presence, frequency, and intensity of fatigue related symptoms during the past one month. The frequency and severity scores were multiplied for each of the eight critical Fu- kuda et al. [1] symptoms and were then summed. To meet the Reeves et al. [2] symptom criterion, a person  Sensitivity and Specificity of the CDC Empirical Chronic Fatigue Syndrome Case Definition Copyright © 2010 SciRes PSYCH 10 needed to have four or more symptoms and a total score greater or equal to 25 on the SI. This overall level of symptoms seems relatively low for patients with classic CFS symptoms (the criterion would be met if an indi- vidual rated only 2 core symptoms as occurring all the time, and if one was of moderate and the other of severe severity). In addition, the 8 case definition symptoms for the empirical case definition were based on a time period comprising the last month compared to what is specified in the Fukuda et al. criteria, which states that: “There needs to be the concurrent occurrence of 4 or more of the following symptoms, and all must be persistent or recur- rent during 6 or more months of the illness and not pre- date the fatigue.” Jason, Najer, Porter, and Reh [7] recently investigated this CFS empirical case definition with 27 participants with a diagnosis of CFS and 37 participants with a diag- nosis of a Major Depressive Disorder (MDD). All par- ticipants completed questionnaires measuring disability (SF-36), fatigue (MFI), and symptoms (SI). Jason et al. found that 38% of those with a diagnosis of MDD were misclassified as having CFS using the new CDC empiri- cal case definition. Jason, Evans, et al. [8] later used this same sample to examine issues of sensitivity and speci- ficity for the three instruments along with their cut-off points. Sensitivity is the probability that the test correctly classifies a person with CFS as positive, whereas specificity is the probability that a test correctly classifies a person without CFS as negative. When Jason, Evans, et al. used a Receiver Operating Characteristic (ROC) curve analysis with the Reeves et al. criteria [2], they found the disability, fatigue and symptom criteria had serious specificity and/or sensitivity problems. They concluded that the Reeves et al. criteria would not be considered a good diagnostic method for selecting CFS cases among a sample of CFS and MDD cases. Reeves, Gurbaxani, Lin, and Unger [9] critiqued the study by Jason et al. [7] by stating that the study should have relied on better methods to diagnose the sample, including a medical and psychiatric examination. An- other criticism brought up by Reeves et al. was the focus on MDD, particularly as some persons with CFS also suffer from MDD. Some individuals with CFS do have MDD, but the key issue is that MDD can be confused with CFS, as it has some overlapping symptoms with CFS. For example, it is possible that some patients with MDD also have chronic fatigue and four CFS Fukuda et al. [1] symptoms that can occur with depression (e.g., unrefreshing sleep, joint pain, muscle pain, impairment in concentration). Yet, CFS and MDD are different dis- orders, and they can be differentiated by use of appropri- ate assessment instruments [10]. Great care needs to be exercised when determining which scales, with which cut off points, should indicate that CFS criteria has been reached for CFS samples. For example, Jason, Brown, et al. [11] examined published studies using the SF-36 [3] which contrasted CFS with controls. The largest differences emerged for the Role Physical, Social Functioning, and Vitality SF-36 sub- scales. Rather than arbitrarily selecting the lower 25% for four SF-36 sub-scales, as was recommended by the au- thors of the empirical CDC CFS case definition [2], Ja- son, Brown, et al. used Receiver Operating Characteris- tics (ROC) to determine sub-scales that best discriminate CFS from Controls in two well defined samples, one involving a community data base collected in the mid 1990s, and the other a tertiary data base collected in the mid 2000s. Vitality, Social Functioning, and Role Physi- cal had the highest AUCs, with good sensitivity and specificity. Because the Jason, Brown, et al. study [11] only had data on the SF-36, these investigators were not able to examine the Reeves et al. [2] recommendations on fa- tigue or symptom criteria. In addition, the Jason et al. [7] sample, which had all three Reeves et al. measures, had been criticized as not having formal medical and psychi- atric examinations to select cases. The present study in- cludes the disability, fatigue, and symptom measures as recommended by Reeves et al. in a carefully defined sample. In this study, we employed an ROC to determine the sensitivity and specificity of the Reeves et al. criteria in a well characterized community-based CFS sample. This study included formal medical and psychiatric tests to determine CFS status. 2. Method The present project was carried out in two stages. In Stage 1, we attempted to re-contact the 213 adults who were medically and psychiatrically evaluated from a community-based sample from 1995-1997. These adults were previously evaluated in our original Wave 1 CFS epidemiology project [12]. Stage 2 of the study encom- passed a structured psychiatric assessment, a complete physical examination and a structured medical history. The original Wave 1 sample collected from 1995-1997 is a stratified random sample of several neighborhoods in Chicago specifically selected to contain individuals from different ethnic and socioeconomic profiles. As a whole, Chicago, Illinois is an ethnically and socioeconomically diverse city. We sampled in eight Chicago community locations, including low socioeconomic areas such as West Garfield Park, middle-socioeconomic areas such as Bridgeport and Armour Park, gentrifying areas such as the near West Side, and high socioeconomic areas such as the Loop and the near North Side. Racial data indicate that the sample consists of 20.0% African-Americans, 52.6% Caucasians, 18.7% Latinos, 0.5% Native Ameri- cans, 5.5% Asian Americans, 1.4% multiracial individu- als, and 1.3% individuals of other races [12]. The tele- phone numbers comprising the stratified random sample  Sensitivity and Specificity of the CDC Empirical Chronic Fatigue Syndrome Case Definition Copyright © 2010 SciRes PSYCH 11 were obtained from Survey Sampling, Incorporated. This company generated random telephone numbers using valid Chicago exchanges, resulting in a sample of both listed and unlisted numbers (as well as business and non-working numbers). In the first stage of data collec- tion in the original study, procedures developed by Kish [13] were used to select one adult from each household for subsequent screening for CFS-like illness. Birth dates for each adult were gathered and the person with the most recent birthday was selected to be interviewed us- ing the Stage 1 CFS Screening Questionnaire. The final sample of respondents consisted of 18,675 households. 2.1 Stage 1 The CFS Screening Questionnaire consists of two parts and was administered to all participants that could be located for this follow-up study. It assessed partici- pants’ sociodemographic characteristics and fatigue characteristics to determine whether any changes have occurred since the first wave of data collection in the original study. Basic demographic data included age, ethnicity, socioeconomic status, work status, marital status, parental status (including number of children) and gender. Consistent with the procedures followed in the original CFS epidemiology study [12] the CFS Screening Questionnaire contains questions measuring more specific aspects of fatigue and health status. In addition, questions assessed the level of impairment that fatigue and illness cause to daily activities, as well as the frequency and duration of the fatigue. Respondents were also asked if they have ever been diagnosed with any other medical or psychiatric conditions associated with chronic fatigue and what current treatments they were receiving. A version of the screening scale used in the present study was evaluated by Jason et al. [14]. They recruited four groups of subjects (i.e., those diag- nosed with CFS, lupus, and multiple sclerosis, and a healthy control group). All subjects were interviewed with a screening instrument twice over a two-week pe- riod of time. The screening scale exhibited high dis- criminant validity and excellent test-retest and in- ter-rater reliability. Hawk et al. [10] revised this CFS Screening Questionnaire, and administered the ques- tionnaire to three groups (those with CFS, MDD, and healthy controls). The revised instrument, which was used in the present study, evidences good test-retest reliability and has good sensitivity and specificity. 2.2 Stage 2 In Stage 2, the Structured Clinical Interview for the DSM-IV (SCID) [15] was administered to assess current psychiatric diagnoses as defined on Axis I of the Diag- nostic and Statistical Manual of Mental Disorders – Fourth Edition (DSM-IV) [16]. The SCID is a valid and reliable semi-structured interview guide that approxi- mates a traditional psychiatric interview [17]. It has been successfully used to assess psychiatric disorders in sam- ples of people with CFS [18]. Following the structured psychiatric interview, par- ticipants were provided a medical history interview and complete medical examination. Prior to the physical ex- amination, the interviewer who accompanied participants and provided transportation to the medical exam admin- istered the Medical Questionnaire at the physician’s of- fice to assess current and past medical history. The Medical Questionnaire is a modified version of The Chronic Fatigue Questionnaire, a structured instrument developed by Komaroff and Buchwald [19] that was used in a study by Komaroff et al. [20]. This comprehen- sive instrument assesses symptoms related to CFS and chronic fatigue, as well as other medical and psychiatric symptoms, in order to help rule out exclusionary condi- tions such as HIV/AIDS, active malignancies, iatrogenic conditions resulting from the side effects of medication, unresolved cases of hepatitis, and active substance use. In addition, the Medical Questionnaire measures fatigue severity, fatigue-related social role impairment, psycho- social stressors, job satisfaction, toxic exposures prior to CFS onset, chemical sensitivities, presence of CFS or chronic fatigue in other network members, and family medical history. Because sleep disturbances are often reported by individuals with CFS and chronic fatigue, the Sleep Disturbance Questionnaire, which has been vali- dated experimentally in a sleep laboratory [21], has been incorporated into the medical questionnaire to help iden- tify participants with sleep disorders. Participants also filled out the Medical Outcome Sur- vey Short-Form-36 (SF-36) [3]. This 36-item instrument is composed of multi-item scales that assess functional impairment in eight areas: limits in physical activities (physical functioning), limits in one’s usual role activi- ties due to physical health (role physical), limits in one’s usual role activities due to emotional health (role emo- tional), bodily pain, general health perceptions (general health), energy and fatigue (vitality), social functioning, and general mental health. Scores in each area reflect ability to function and higher values indicate better func- tioning. Reliability and validity studies have demon- strated high reliability and validity in a wide variety of patient populations for this instrument [22]. According to Reeves et al. [2] significant reductions in occupational, educational, social, or recreational activities were defined as scores lower than the 25th percentile on Physical Func- tioning (less than or equal to 70), or Role Physical (less than or equal to 50), or Social Functioning (less than or equal to 75), or Role Emotional (less than or equal to 66.7). A person would meet the disability criterion for the empirical CFS case definition by showing impair- ment in one or more of these four areas. Participants also completed the CDC Symptom Inven-  Sensitivity and Specificity of the CDC Empirical Chronic Fatigue Syndrome Case Definition Copyright © 2010 SciRes PSYCH 12 tory (SI) [5]. The SI assesses information about the presence, frequency, and intensity of 19 fatigue related symptoms during the past one month. For each of the eight Fukuda et al. [1] symptoms, participants were asked to report the frequency (1 = a little of the time, 2 = some of the time, 3 = most of the time, 4 = all of the time) and severity (the ratings were transformed to the follow- ing scale: 0 = symptom not reported, 1 = mild, 2.5 = moderate, 4 = severe)1. The frequency and severity scores were multiplied for each of the eight critical Fu- kuda et al. symptoms and were then summed. Individuals having four or more symptoms and scoring greater or equal to 25 would meet symptom criterion on this in- strument according to the CDC empirical case definition. Additionally, the participants completed the Multidi- mensional Fatigue Inventory (MFI) [4]. This instrument is a 20-item self-report instrument consisting of five scales: general fatigue, physical fatigue, reduced activity, reduced motivation, and mental fatigue. Each scale con- tains four items rated from 1 to 5 with the scale score of 1= completely true and the scale score of 5 = no, not true. Reeves et al. [2] employed the MFI to measure severe fatigue, and to do this, they used only two of the five subscales; General Fatigue and Reduced Activity. Using the CDC empirical case definition standards, severe fa- tigue was defined as greater than or equal to 13 on Gen- eral Fatigue or greater than or equal to ten on Reduced Activity. Following the medical history interview, the physician conducted a detailed medical examination. This exami- nation was carried out in order to rule out exclusionary medical conditions and detect evidence of diffuse ade- nopathy, hepatosplenomegaly, synovitis, neuropathy, myopathy, cardiac or pulmonary dysfunction, or any other medical disorder. An 18-tender-point examination was used to test for Fibromyalgia [23]. Laboratory tests administered to all participants included a chemistry screen (glucose, calcium, electrolytes, uric acid, liver function tests, and renal function tests), complete blood count with differential and platelet count, T4 and TSH, erythrocyte sedimentation rate, arthritic profile (which includes rheumatoid factor and antinuclear antibody), hepatitis B surface antigen, CPK, HIV screen, and uri- nalysis. An intra-dermal, intermediate-strength PPD skin test was applied, and a posterior-anterior chest x-ray was completed, if it was not already obtained by the partici- pant within eight months of entering the study. At the time of evaluation, the examining physician was blinded to participants’ status with respect to initial classification based upon the Stage 1 screen. Participants were reim- bursed $100.00 for the time and effort involved in par- ticipation. Participants also signed the Human Subjects Consent Form (See Jason, Porter, Hunnell, Rademaker, & Richman [24] for more details). At the end of Stage 2, a team of physicians was re- sponsible for making final diagnoses. Two physicians independently rated each file according to the current U.S. definition of CFS. Files that did not meet CFS crite- ria were rated as either idiopathic chronic fatigue (ICF), exclusionary for CFS due to medically/psychiatrically explained chronic fatigue [1], or control (participants with no exclusionary illness and less than 6 months of fatigue). Those with ICF had at least six months duration of fatigue, but with insufficient symptoms or fatigue to meet the case definition of CFS. The exclusionary group had chronic fatigue for at least six months duration, but with active medical conditions that explain chronic fa- tigue (e.g., untreated hypothyroidism), previously diag- nosed medical disorders whose resolution has not been documented beyond reasonable clinical doubt, and whose continued activity may explain the chronic fatiguing ill- ness (e.g., unresolved cases of hepatitis C). The exclu- sionary group also included those with chronic fatigue for at least six months duration, but with psychiatric ex- planations of the fatigue (e.g., delusional disorders, schizophrenia, etc). Controls had no exclusionary ill- nesses and less than 6 months of fatigue. Reviewing phy- sicians had access to all information gathered on each participant during each of the phases of the study. The review panel was also provided with all results from the physical exam. If a disagreement occurred during the physician review process regarding whether a participant should receive a diagnosis of CFS, ICF, exclusionary due to medically/psychiatrically explained chronic fatigue, or control, the participant’s file was rated by a third physi- cian reviewer, and the diagnosis was determined by ma- jority rule. We used refinements of the Fukuda et al. cri- teria as recommended by an International Research group and the CDC [25]. 2.3 Sample Characteristics In Wave 1, 213 adults were medically and psychiatrically evaluated from the community-based sample. For the follow-up study, data was available on 24 individuals diagnosed with CFS and 84 who did not have CFS. Wave 1 differences were examined between those we were able versus those we were not able to re-evaluate at Wave 2, and we did not find any significant sociodemographic differences for age, gender, race, marital status, number of children, or education (See Jason, Porter, et al., [24] for more details). 2.4 Statistical Analysis The statistical software package used for data analysis was PASW (formerly SPSS) for Windows, version 17.0. A Receiver Operating Characteristic (ROC) curve analy- sis [26] was used to evaluate the ability of the scales to 1The scale we used had five choices, and we needed to convert the ratings to a four point scale in order to conform to Wagner et al.’s (2005) severity scaling system. 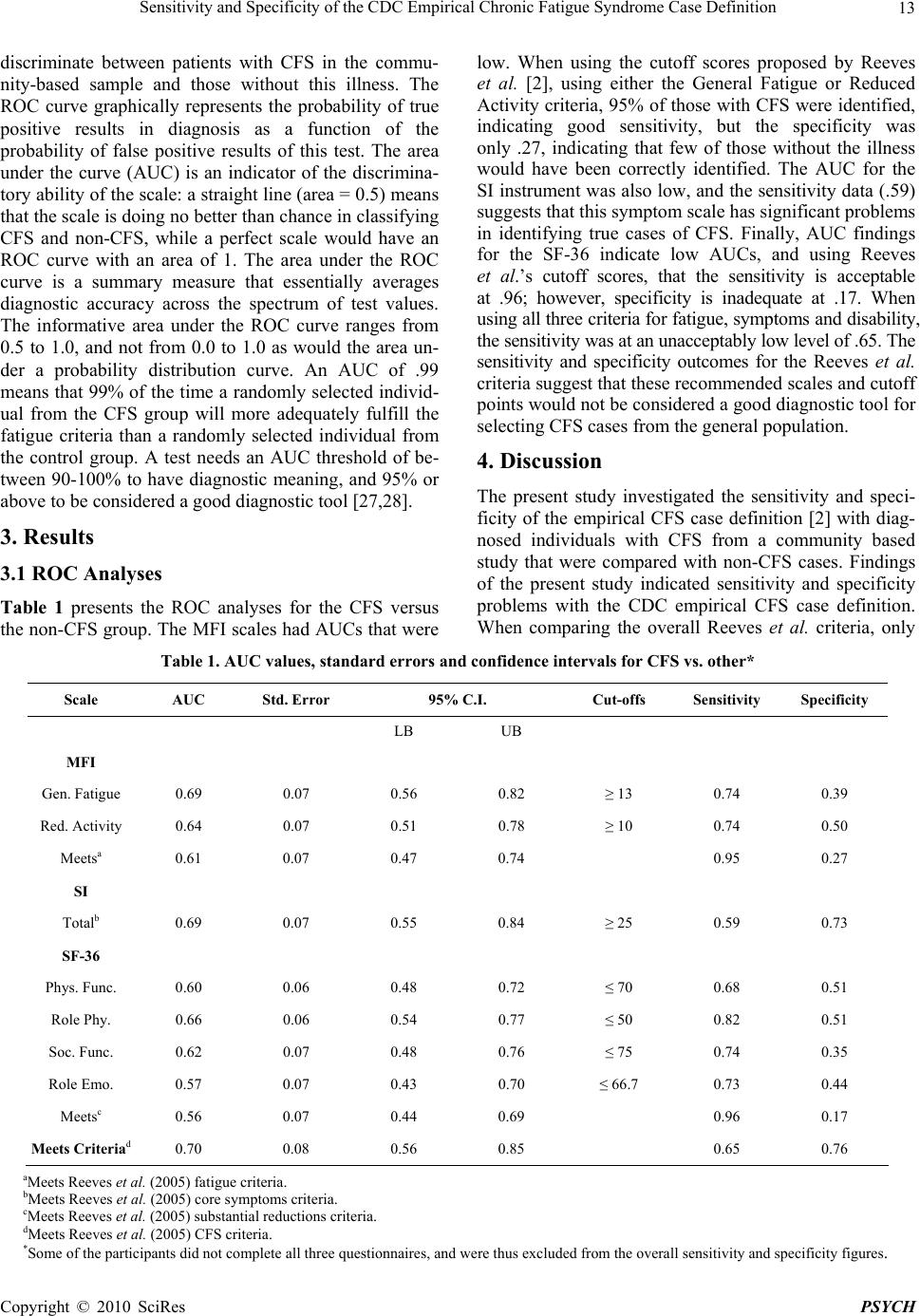 Sensitivity and Specificity of the CDC Empirical Chronic Fatigue Syndrome Case Definition Copyright © 2010 SciRes PSYCH 13 discriminate between patients with CFS in the commu- nity-based sample and those without this illness. The ROC curve graphically represents the probability of true positive results in diagnosis as a function of the probability of false positive results of this test. The area under the curve (AUC) is an indicator of the discrimina- tory ability of the scale: a straight line (area = 0.5) means that the scale is doing no better than chance in classifying CFS and non-CFS, while a perfect scale would have an ROC curve with an area of 1. The area under the ROC curve is a summary measure that essentially averages diagnostic accuracy across the spectrum of test values. The informative area under the ROC curve ranges from 0.5 to 1.0, and not from 0.0 to 1.0 as would the area un- der a probability distribution curve. An AUC of .99 means that 99% of the time a randomly selected individ- ual from the CFS group will more adequately fulfill the fatigue criteria than a randomly selected individual from the control group. A test needs an AUC threshold of be- tween 90-100% to have diagnostic meaning, and 95% or above to be considered a good diagnostic tool [27,28]. 3. Results 3.1 ROC Analyses Table 1 presents the ROC analyses for the CFS versus the non-CFS group. The MFI scales had AUCs that were low. When using the cutoff scores proposed by Reeves et al. [2], using either the General Fatigue or Reduced Activity criteria, 95% of those with CFS were identified, indicating good sensitivity, but the specificity was only .27, indicating that few of those without the illness would have been correctly identified. The AUC for the SI instrument was also low, and the sensitivity data (.59) suggests that this symptom scale has significant problems in identifying true cases of CFS. Finally, AUC findings for the SF-36 indicate low AUCs, and using Reeves et al.’s cutoff scores, that the sensitivity is acceptable at .96; however, specificity is inadequate at .17. When using all three criteria for fatigue, symptoms and disability, the sensitivity was at an unacceptably low level of .65. The sensitivity and specificity outcomes for the Reeves et al. criteria suggest that these recommended scales and cutoff points would not be considered a good diagnostic tool for selecting CFS cases from the general population. 4. Discussion The present study investigated the sensitivity and speci- ficity of the empirical CFS case definition [2] with diag- nosed individuals with CFS from a community based study that were compared with non-CFS cases. Findings of the present study indicated sensitivity and specificity problems with the CDC empirical CFS case definition. When comparing the overall Reeves et al. criteria, only Table 1. AUC values, standard errors and confidence intervals for CFS vs. other* Scale AUC Std. Error 95% C.I. Cut-offs Sensitivity Specificity LB UB MFI Gen. Fatigue 0.69 0.07 0.56 0.82 ≥ 13 0.74 0.39 Red. Activity 0.64 0.07 0.51 0.78 ≥ 10 0.74 0.50 Meetsa 0.61 0.07 0.47 0.74 0.95 0.27 SI Totalb 0.69 0.07 0.55 0.84 ≥ 25 0.59 0.73 SF-36 Phys. Func. 0.60 0.06 0.48 0.72 ≤ 70 0.68 0.51 Role Phy. 0.66 0.06 0.54 0.77 ≤ 50 0.82 0.51 Soc. Func. 0.62 0.07 0.48 0.76 ≤ 75 0.74 0.35 Role Emo. 0.57 0.07 0.43 0.70 ≤ 66.7 0.73 0.44 Meetsc 0.56 0.07 0.44 0.69 0.96 0.17 Meets Criteriad 0.70 0.08 0.56 0.85 0.65 0.76 aMeets Reeves et al. (2005) fatigue criteria. bMeets Reeves et al. (2005) core symptoms criteria. cMeets Reeves et al. (2005) substantial reductions criteria. dMeets Reeves et al. (2005) CFS criteria. *Some of the participants did not complete all three questionnaires, and were thus excluded from the overall sensitivity and specificity figures.  Sensitivity and Specificity of the CDC Empirical Chronic Fatigue Syndrome Case Definition Copyright © 2010 SciRes PSYCH 14 about 65% of true CFS cases were identified. In other words, these criteria are not able to identify an acceptable high percentage of individuals who have this illness. If samples of CFS are not identified with sensitivity and specificity, it will be difficult to compare samples from different studies, and the search for biological markers will be compromised. Using the Reeves et al. criteria [2], the estimated rates of CFS have increased to 2.54% [29], rates that are about ten times higher than prior CDC estimates [30] and prevalence estimates of other investigators [31]. It is at least possible that the increases in the United States are due to a broadening of the case definition and possible inclusion of cases with primary psychiatric conditions. Chronic fatigue occurs in about 4-5% of the population [32]. If about 5% of the population has 6 or more months of fatigue, and about half of this is due to clear medical or psychiatric reasons [31], then the critical question is how many of the re- maining 2.5% have CFS. The empirical CFS case defini- tion estimates that 2.54% do have this illness, so that research group would suggest that almost all of the re- maining 2.5% would fall within the CFS category. However, Jason et al. [7] believe that within this 2.54% are mood disorders, which are one of the most prevalent psychiatric disorders (one-month prevalence rate of ma- jor depressive episode is 2.2%) [33]. As an example, one mood disorder is MDD, which can be confused with CFS, as it has some overlapping symptoms with CFS. It is possible that some patients with MDD also have chronic fatigue and four CFS Fukuda et al. [1] symptoms that can occur with depression (e.g., unrefreshing sleep, joint pain, muscle pain, impairment in concentration). Fatigue and these four minor symptoms are also defining criteria for CFS, so it is possible that some patients with a primary affective disorder could be misdiagnosed as having CFS. Yet, these are distinct illnesses, as several CFS symp- toms are not commonly found in depression, including prolonged fatigue after physical exertion, night sweats, sore throat, and swollen lymph nodes. Illness onset with CFS often occurs over a few hours or days, whereas pri- mary depression generally shows a more gradual onset. Biological findings also differentiate the two conditions [34]. Including the latter type of patients in the current CFS case definition could confound the interpretation of epidemiologic and treatment studies, and complicate ef- forts to identify biological markers for this illness. It is important for screening tests to have high sensi- tivity and specificity, particularly for disorders with low prevalence rates such as CFS (about 4.2 in a thousand) [31]. As an example, in a city of 1,000,000, with a true CFS rate of 4.2 per thousand, there would be 4,200 CFS cases. According to Bayes’ theorem [35] if a diagnostic test had a 95% rate of sensitivity, the screening test would correctly identify 3,990 of these cases. However, if the test had 95% specificity, there would be 49,790 individuals who did not have CFS but were identified as having it using the test. Clearly, being able to identify true negatives with precision is of high importance in the diagnostic process. We provide two case studies that illustrate several of the problems with the Reeves et al. [2] criteria. For ex- ample, one person who we diagnosed with CFS did not meet the Reeves et al. empirical case definition due to not meeting the frequency/severity requirement for the Symptom Inventory (SI). Yet, this person indicated that she had experienced a 95% decrease in daily activities over the past 6 months and an 80% decrease in daily en- ergy level over the last 6 months. The person also re- ported having experienced 6 months of fatigue and more than 4 core symptoms. On a different scale from the medical questionnaire, using a 100 point scale, with higher scores indicating more problems, the person had a score of 80 on impaired memory and 85 on un-refreshing sleep. Our physician panel clearly felt that this person met all CFS Fukuda et al. [1] criteria, but the person was not included as a CFS case using the Reeves et al. crite- ria. In contrast, another person who we classified as ICF met the Reeves et al. empirical case definition. This person only had a 30% reduction in daily activity in the last 6 months and a 30% reduction of daily energy levels in the last 6 months. Our physician panel did not diag- nose this participant has having CFS, yet the person was counted as a CFS case using the Reeves et al . criteria. There are several limitations in this study. First, the community-based study of participants was relatively small. Clearly, these results need to be replicated by other investigators with larger samples. However, when the Reeves et al. [2] disability criteria were evaluated on a tertiary care setting [11], the findings also pointed to sensitivity and specificity problems. Another study using psychiatric controls also found the empirical case defini- tion to be problematic due to specificity issues [7]. In summary, the scientific enterprise depends on reli- able and valid ways of classifying patients into diagnos- tic categories, and this critical research activity can en- able investigators to better understand etiology, patho- physiology, and treatment approaches for CFS and other disorders [36]. When diagnostic categories lack reliabil- ity and accuracy, the quality of treatment and clinical research can be significantly compromised. If CFS is to be diagnosed reliably across health care professionals, it is imperative to provide specific thresholds and scoring rules for the symptomatic criteria. REFERENCES [1] K. Fukuda, S. E. Straus, I. Hickie, M. C. Sharpe, J. G. Donnibs and A. Komaroff, “The Chronic Fatigue Syn- drome: A Comprehensive Approach to Its Definition and Study,” Annals of Internal Medicine, Vol. 121, 1994, pp. 953-958.  Sensitivity and Specificity of the CDC Empirical Chronic Fatigue Syndrome Case Definition Copyright © 2010 SciRes PSYCH 15 [2] W. C. Reeves, D. Wagner, R. Nisenbaum, J. F. Jones, B. Gurbaxani, L. Solomon, et al., “Chronic Fatigue Syn- drome– A Clinically Empirical Approach to Its Definition and Study,” BMC Medicine, Vol. 3, 2005. http://www. biomedcentral.com/1741-7015/3/19 [3] J. E. Ware, K. K. Snow and M. Kosinski, “SF-36 Health Survey: Manual and Interpretation Guide,” Quality Met- ric Incorporated, 2000. [4] E. M. Smets, B. J. Garssen, B. Bonke and J. C. DeHaes, “The Multidimensional Fatigue Inventory (MFI): Psy- chometric Properties of an Instrument to Assess Fatigue,” Journal of Psychosomatic Research, Vol. 39, 1995, pp. 315-325. [5] D. Wagner, R. Nisenbaum, C. Heim, J. F. Jones, E. R. Unger and W. C. Reeves, “Psychometric Properties of the CDC Symptom Inventory for Assessment of Chronic Fa- tigue Syndrome,” Population Health Metrics, Vol. 3, 2005. http://www.pophealthmetrics.com/content/3/1/8 [6] L. A. Tiersky, R. J. Matheis, J. DeLuca, G. Lange and B. H. Natelson, “Functional Status, Neuropsychological Functioning, and Mood in Chronic Fatigue Syndrome,” Journal of Nervous and Mental Disease, Vol. 191, 2003, pp. 324-331. [7] L. A. Jason, N. Najar, N. Porter and C. Reh, “Evaluating the Centers for Disease Control’s Empirical Chronic Fa- tigue Syndrome Case Definition,” Journal of Disability Policy Studies, Vol. 20, 2009, pp. 93-100. [8] L. A. Jason, M. Evans, M. Brown, N. Porter, A. Brown, J. Hunnell, et al., “Fatigue Scales and Chronic Fatigue Syn- drome: Issues of Sensitivity and Specificity,” Manuscript Submitted for Publication, 2010. [9] W. C. Reeves, B. M. Gurbaxani, J. S. Lin and E. R. Un- ger, “A Response to Jason et al., ‘Evaluating the Centers for Disease Control’s Empirical Chronic Fatigue Syn- drome Case Definition,” Journal of Disability Policy Studies Online First, 2009. http://dps.sagepub.com/cgi/ rapidpdf/1044207309346310v1.pdf [10] C. Hawk, L. A. Jason and S. Torres-Harding, “Differen- tial Diagnosis of Chronic Fatigue Syndrome and Major Depressive Disorder,” International Journal of Behav- ioral Medicine, Vol. 13, 2006, pp. 244-251. [11] L. A. Jason, M. Brown, M. Evans, V. Anderson, A. Lerch, A. Brown, et al., “Measuring Substantial Reduction in Functioning with CFS,” Manuscript Submitted for Publi- cation, 2010. [12] L. A. Jason, K. M. Jordan, J. A. Richman, A. W. Rade- maker, C. Huang, W. McCready, et al., “A Commu- nity-Based Study of Prolonged and Chronic Fatigue,” Journal of Health Psychology, Vol. 4, 1999, pp. 9-26. [13] L. Kish, “Survey Sampling,” John Riley and Sons, In- corporated, 1965. [14] L. A. Jason, M. T. Ropacki, N. B. Santoro, J. A. Richman, W. Heatherly, R. Taylor, et al., “A Screening Instrument for Chronic Fatigue Syndrome: Reliability and Validity,” Journal of Chronic Fatigue Syndrome, Vol. 3, No. 1, 1997, pp. 39-59. [15] R. L Spitzer, J. B. W. Williams, M. Gibbon and M. B. First, “Structured Clinical Interview for DSM-IV- Non-Patient Edition (SCID-NP, Version 2.0),” American Psychiatric Press, 1995. [16] “Diagnostic and Statistical Manual of Mental Disorders,” Forth Edition, American Psychiatric Association, 1994. [17] M. B. First, R. L. Spitzer, M. Gibbon and J. B. W. Wil- liams, “Structured Clinical Interview for DSM-IV Axis I Disorders-Patient Edition,” Biometrics Research De- partment, 1995. [18] R. R. Taylor and L. A. Jason, “Comparing the DIS with the SCID: Chronic Fatigue Syndrome and Psychiatric Comorbidity,” Psychology and Health: The International Review of Health Psychology, Vol. 13, 1998, pp. 1087- 1104. [19] A. L. Komaroff and D. S. Buchwald, “Symptoms and Signs of Chronic Fatigue Syndrome,” Reviews of Infec- tious Diseases, Vol. 13, 1991, pp. 8-11. [20] A. L. Komaroff, L. R. Fagioli, A. M. Geiger, T. H. Doo- little, J. Lee, R. J. Kornish, et al., “An Examination of the Working Case Definition of Chronic Fatigue Syndrome,” The American Journal of Medicine, Vol. 100, 1996, pp. 56-64. [21] D. Buchwald, R. Pascualy, C. Bombardier and P. Kith, “Sleep Disorders in Patients with Chronic Fatigue,” Clin- ical Infectious Diseases, Vol. 18, 1994, pp. S68-S72. [22] A. L. Stewart, S. Greenfield, R. D. Hayes, K. Wells, W. H. Rogers, S. D. Berry, et al., “Functional Status and Well-Being of Patients with Chronic Conditions: Results from the Medical Outcomes Study,” Journal of the American Medical Association, Vol. 262, No. 7, 1989, pp. 907-913. [23] P. Goodnick and R. Sandoval, “Treatment of Chronic Fatigue Syndrome and Related Disorders: Immunological Approaches,” In P. Goodnick and N. Klimas Eds., Chronic Fatigue and Related Immune Deficiency Syn- dromes, American Psychiatric Press, 1993, pp. 131-161. [24] L. A. Jason, N. Porter, J. Hunnell, A. Rademaker and J. Richman, “CFS Prevalence and Risk Factors Over Time,” Manuscript Submitted for Publication, 2010. [25] W. C. Reeves, A. Lloyd, S. D. Vernon, N. Klimas, L. A. Jason, G. Bleijenberg, et al., “Identification of Ambiguities in the 1994 Chronic Fatigue Syndrome Research Case Defini- tion and Recommendations for Resolution,” BMC Health Servic es Resea rch, Vol. 3, 2003. http://www.biomedcentral. com/content/pdf/1472-6963-3-25.pdf [26] J. A. Hanley and B. J. McNeil, “The Meaning and Use of the Area under a Receiver Operating Characteristics (ROC) Curve,” Radiology, Vol. 143, 1982, pp. 29-36. [27] K. H. Zou, A. J. O’Malley and L. Mauri, “Receiver- Operating Characteristic Analysis for Evaluating Diag- nostic Tests and Predictive Models,” Circulation, Vol. 115, 2007, pp. 654-657. [28] M. H. Zweig and G. Campbell, “Receiver-Operating Characteristic (ROC) Plots: A Fundamental Evaluation Tool in Clinical Medicine,” Clinical Chemistry, Vol. 39, 1993, pp. 561-577.  Sensitivity and Specificity of the CDC Empirical Chronic Fatigue Syndrome Case Definition Copyright © 2010 SciRes PSYCH 16 [29] W. C. Reeves, J. J. Jones, E. Maloney, C. Heim, D. C. Hoaglin, R. Boneva, et al., “New Study on the Preva- lence of CFS in Metro, Urban and Rural Georgia Popu- lations,” Population Health Metrics, Vol. 5, 2007. http:// www.pophealthmetrics.com/content/5/1/5 [30] M. Reyes, R. Nisenbaum, D. C. Hoaglin, E. R. Unger, C. Emmons, B. Randall, et al., “Prevalence and Incidence of Chronic Fatigue Syndrome in Wichita, Kansas,” Archives of Internal Medicine, Vol. 163, 2003, pp. 1530-1536. [31] L. A. Jason, J. A. Richman, A. W. Rademaker, K. M. Jordan, A. V. Plioplys, R. Taylor, et al., “A Commu- nity-Based Study of Chronic Fatigue Syndrome,” Ar- chives of Internal Medicine, Vol. 159, 1999, pp. 2129- 2137. [32] L. A. Jason, M. Evans, M. Brown and N. Porter, “What is Fatigue? Pathological and Non-Pathological Fatigue,” Manuscript Submitted for Publication, 2010. [33] D. A. Regier, J. H. Boyd and J. D. Burke Jr., “One Month Prevalence of Mental Disorders in the United States: Based on Five Epidemiological Catchment Rea Sites,” Archives of General Psychiatry, Vol. 45, 1988, pp. 977- 986. [34] L. A. Jason, K. Corradi, S. Torres-Harding, R. R. Taylor and C. King, “Chronic Fatigue Syndrome: The Need For Subtypes,” Neuropsychology Review, Vol. 15, 2005, pp. 29-58. [35] E. T. T. Jaynes, “Probability Theory: The Logic of Sci- ence,” G. L. Bretthorst Ed., Cambridge University Press, 2003. [36] C. King and L. A. Jason, “Improving the Diagnostic Cri- teria and Procedures for Chronic Fatigue Syndrome,” Bi- ological Psychology, Vol. 68, 2005, pp. 87-106. |