Paper Menu >>
Journal Menu >>
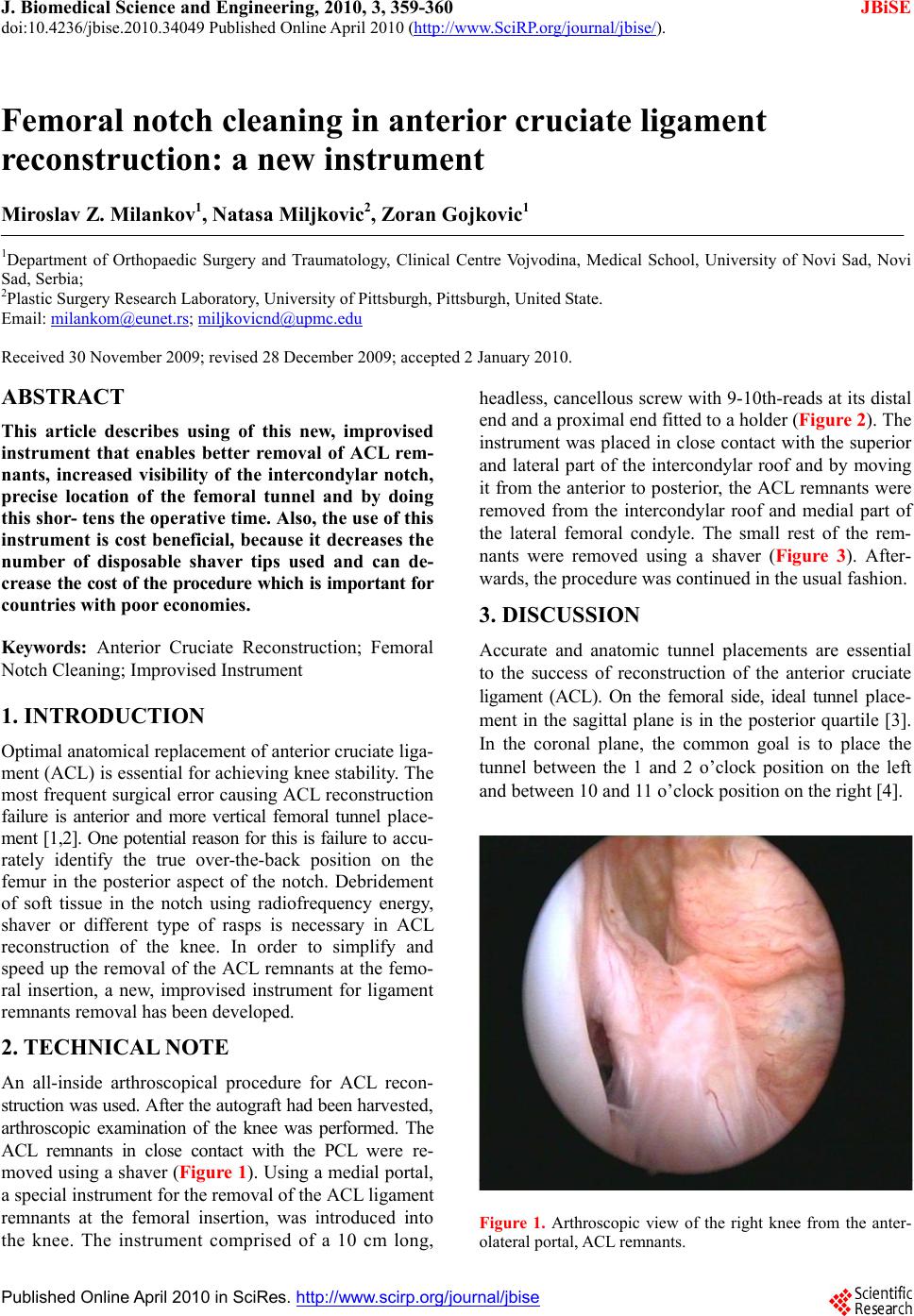 J. Biomedical Science and Engineering, 2010, 3, 359-360 JBiSE doi:10.4236/jbise.2010.34049 Published Online April 2010 (http://www.SciRP.org/journal/jbise/). Published Online April 2010 in SciRes. http://www.scirp.org/journal/jbise Femoral notch cleaning in anterior cruciate ligament reconstruction: a new instrument Miroslav Z. Milankov1, Natasa Miljkovic2, Zoran Gojkovic1 1Department of Orthopaedic Surgery and Traumatology, Clinical Centre Vojvodina, Medical School, University of Novi Sad, Novi Sad, Serbia; 2Plastic Surgery Research Laboratory, University of Pittsburgh, Pittsburgh, United State. Email: milankom@eunet.rs; miljkovicnd@upmc.edu Received 30 November 2009; revised 28 December 2009; accepted 2 January 2010. ABSTRACT This article describes using of this new, improvised instrument that enables better removal of ACL rem- nants, increased visibility of the intercondylar notch, precise location of the femoral tunnel and by doing this shor- tens the operative time. Also, the use of this instrument is cost beneficial, because it decreases the number of disposable shaver tips used and can de- cr ea se the cost of the procedure which is impor tant for countries with poor economies. Keywords: Anterior Cruciate Reconstruction; Femoral Notch Cleaning; Improvised Instrument 1. INTRODUCTION Optimal anatomical replacement of anterior cruciate liga- ment (ACL) is essential for achieving knee stability. The most frequent surgical error causing ACL reconstruction failure is anterior and more vertical femoral tunnel place- ment [1,2]. One po tential reason for this is failur e to a ccu - rately identify the true over-the-back position on the femur in the posterior aspect of the notch. Debridement of soft tissue in the notch using radiofrequency energy, shaver or different type of rasps is necessary in ACL reconstruction of the knee. In order to simplify and speed up the removal of the ACL remnants at the femo- ral insertion, a new, improvised instrument for ligament remnants removal has been developed. 2. TECHNICAL NOTE An all-inside arthroscopical procedure for ACL recon- struction was used. After the autograf t had been harv e st e d, arthroscopic examination of the knee was performed. The ACL remnants in close contact with the PCL were re- moved using a shaver (Figure 1). Using a medial portal, a special instrument for the removal of the ACL ligament remnants at the femoral insertion, was introduced into the knee. The instrument comprised of a 10 cm long, headless, cancellous screw with 9-10th-reads at its distal end and a proximal end fitted to a hold er (Figure 2). The instrument was placed in close contact with the superior and lateral part of the intercondylar roof and by moving it from the anterior to posterior, the ACL remnants were removed from the intercondylar roof and medial part of the lateral femoral condyle. The small rest of the rem- nants were removed using a shaver (Figure 3). After- wards, the procedure was continued in the usual fashion. 3. DISCUSSION Accurate and anatomic tunnel placements are essential to the success of reconstruction of the anterior cruciate ligament (ACL). On the femoral side, ideal tunnel place- ment in the sagittal plane is in the posterior quartile [3]. In the coronal plane, the common goal is to place the tunnel between the 1 and 2 o’clock position on the left and between 10 and 11 o’clock position on the right [4]. Figure 1. Arthroscopic view of the right knee from the anter- olateral portal, ACL remnants.  M. Z. Milankov et al. / J. Biomedical Science and Engineering 3 (2010) 359-360 Copyright © 2010 SciRes. JBiSE 360 Figure 2. New, improvised instrument for ACL remnants re- moval. The instrument comprised of a 10 cm long, headless, cancellous screw with 9-10 threads at its distal end and a proximal end fitted to a holder. Figure 3. Arthroscopic view of the right knee from the anter- olateral portal after using instrument. ACL remnants were re- moved from the intercondylar roof and medial part of the lat- eral femoral condyle. The notch doesn’t have ACL remnants. Tunnel placement based on lateral intercondylar ridge and lateral bifurcate ridge, is a more reliable approach [5-8]. The lateral intercondylar ridge is the superior bor- der of the ACL with the knee in 90o of flexion, and the anterior border of the ACL with the knee in full exten- sion [6,7]. The lateral bifurcate ridge separates the femoral attachment of the AM and PL bundles [6,7]. The visualization of these landmarks requires meticulous rem- nant removal. Failure to recognize these bone land marks, leads to nonanatomic placement of the femoral tunnel and, therefore, premature failure of reconstructions. In older patients with poor bone quality, one has to be very careful not to overdo with the ACL remnant removal, since this can result in a sign ificant bone indentation. Up till now, we have used this instrument in over 200 ar- throscopic ACL reconstruction procedures without any difficulty or complications. 4. CONCLUSIONS The use of this new, improvised instrument enables bet- ter removal of ACL remnants, increased visibility of the intercondylar notch and precise location of the femoral tunnel and by doing this shortens the operative time. Also, the use of this instrument is cost beneficial, be- cause it decreases the number of disposable shaver tips used and can decrease the cost of the procedure which is important for countries with poor economies. REFERENCES [1] Carson, E.W., Simonian, P.T., Wickiewicz, T.L. and War- ren, R.F. (1998) Revision anterior cruciate ligament re- construction. Instructional Course Lectures, 47, 361-368. [2] Sommer, C., Friederich, N.F. and Müller, W. (2000) Im- properly placed anterior cruciate ligament grafts: Corre- lation between radiological parameters and clinical re- sults. The Journal of Knee Surgery, 8, 207-213. [3] Bernard, M., Hertel, P., Hornung, H. and Cierpinski, Th. (1997) Femoral insert ion of the A CL, r ad io gr aphic quadrant method. American Journal of Knee Surgery, 10, 14-22. [4] Loh, J.C., Fukuda, Y., Tsuda, E., Steadman, R.J., Fu, F.H. and Woo, S.L.Y. (2003) Knee stability and graft function following anterior cruciate ligament reconstruction: Com- parison between 11 o’clock and 10 o’clock femoral tun- nel placement. Arthroscopy, 19, 297-304. [5] Farrow, L.D., Chen, M.R., Cooperman, D.R., Victoroff, B.N. and Goodfellow, D.B. (2007) Morphology of the femoral intercondylar notch. The Journal of Bone and Joint Surgery (American), 89, 2150-2155. [6] Ferretti, M., Ekdahl, M., Shen, W. and Fu, F.H. (2007) Osseous landmarks of the femoral attachment of the an- terior cruciate ligament: An anatomic study. Arthroscopy, 23, 1218-1225. [7] Fu, F.H. and Jordan, S.S. (2007) The lateral intercondylar ridge—a key to anatomic anterior cruciate ligament re- construction. The Journal of Bone and Joint Surgery (Am- erican), 89, 2103-2104. [8] Hutchinson, M.R. and Ash, S.A. (2003) Resident’s ridge: Assessing the cortical thickness of the lateral wall and roof of the intercondylar notch. Arthroscopy, 19, 931-935. |