Health
Vol.4 No.12(2012), Article ID:25680,6 pages DOI:10.4236/health.2012.412194
Ego strength and health: An empiric study in hemodialysis patients
![]()
1Department of Human and Social Sciences, University of Messina, Messina, Italy
2Department of Neurosciences, Psychiatric and Anaesthesiological Sciences, Division of Psychiatry, University of Messina, Messina, Italy; *Corresponding Author: cmento@unime.it
3Researcher in Nephrology, Department of Internal Medicine, University of Messina, Messina, Italy
4Department of Clinical and Experimental Medicine and Pharmacology, University of Messina, Messina, Italy
5Department of Nephrology, University of Messina, Messina, Italy
6Nephrology and Dialysis Units, Papardo Hospital, Messina, Italy
7Unit of Nephrology, ASP5 Milazzo Hospital, Milazzo, Italy
8Unit of Nephrology, ASP5 Taormina Hospital, Taormina, Italy
Received 11 September 2012; revised 16 October 2012; accepted 26 October 2012
Keywords: Hemodialysis; Compliance; Ego Strenght; Emotional States
ABSTRACT
Introduction: Ego strength represents an important variable that could be predictable about health and compliance in chronic diseases. In this study we propose a new questionnaire, E.F.E. “Ego Functioning Experience”, able to reveal the psychological functioning profile in Hemodialysis patients. The aim of this work, is to underline the existing relations between emotional profile and compliance, whit E.F.E., that may be predictive of a state of psychologycal health in hemodialysis patients. Methods: Study population included 90 hemodialysis patients. The study protocol was made by three psychological tests: the E.F.E. Questionnaire, the DMI, the Self-Liking and Self-Competence Scale. Results: Factor analysis extracts three factors: 1) “Need of Ego support”; 2) “Ego activity oriented to treatment”; 3) “Ego strength”. The correlation coefficients between the E.F.E. Questionnaire factors (three factors) and other measures, showed a direct correlation with the first factor and “turning against object” TAO of the DMI test (correlation is significant at the 0.001 level) and an inverse relation with set mechanisms of “Principalization”, PRN of the DMI (correlation is significant at the 0.005 level). The correlations of the second and the third factors with other measures, were not statistically significant. No relations were found about other variables. Conclusions: The E.F.E. questionnaire is a simple evaluation to detect hemo-dialysis patients who may need greater attention to the psychological health and therefore the need for treatment such as psychological support. In fact, lower presence of ego strength is indicative of poor compliance to clinical treatment in hemodialysis, but also of worsening of psychiatric symptoms such as demoralization and depressed mood. In conclusion, an increased social support is needed in hemodialysis patient in order to achieve better compliance and achieve a better state of psychological health in chronic hemodialysis patients.
1. INTRODUCTION
Ego strength represents the attitude toward problems, the predominant reaction toward frustration and shows the ability of adaptation in relation to one’s emotional profile [1-6]. In patients with Chronic Kidney Disease (CDK) this ability is severely put to the test by the frustration caused by hemodialysis [7]. The importance of this problem is reported in literature by studies that documented adaptation problems and specific differences that patients on hemodialysis [8-12].
This adaptation process, is based on the model biopsycho-social, because the CKD is a biological complex disease, in which into play factors clinical and psychosocial, that interact differently with each other, in relation to the degree of the disease and the evolution of treatment e.g. pre-dialysis, early dialysis, long term dialysis.
Psychosocial factors e.g. the presence of social support, aspects of self-esteem, negative emotion e.g. anger and feelings of discouragement, perception of illness and religion, play an important psychological role in subjects with CKD and may also affect the clinical factors and the biological state of this patients [13-18].
Several study show that patients with CKD who have a negative attitude, characterized by feelings of loss, failure and rejection, the tendency to experience events so pessimistic, to evoke negative memories, have more complications in psychiatric comorbidity e.g. depression, anxiety, poor QoL, that for the chronic pathology, highest number of hospitalizations, poor compliance to the treatment, worst prognosis [19-24].
Other studies have shown that patients with CKD who had a positive attitude with positive psychosocial characteristics, have accepted the disease, dialysis integrated within their project of life, have a good quality of life, low levels of depression and good compliance to treatment. In addition, these subjects, consider dialysis least intrusive in their lives [25-28].
Due to the number of prescribed drugs in hemodialysis, combined with dietary prescriptions and regularity of sessions hemodialytic, patient compliance is an important issue and is influenced by clinical and psychological factors [29].
Ego strength represents a variable that could be predictable about compliance [17]. Due to the high number of prescribed pills in hemodialysis, patient compliance is an important issue and it seems related to psychosocial factors [16,29,30]. For this reasons, an exhausting clinical-psychological evaluation requires a complex organization, it is necessary to create a specific and simple test for the patients, in order to obtain information regarding compliance and psychological evolution.
We decided to test a new questionnaire, called Ego Functioning Experience, E.F.E. for the conception for the authors Settineri S., Mallamace D., Mento C., that should be able to reveal the psychological functioning profile of Hemodialysis patients. The aims of this work, is finding relations existing between the ego strength (psychological functioning through efe) and other variables such as defense mechanisms and Self-liking and competence, which together constitute predictors of a personological structure more closely tied to the health and compliance of chronic treatment in hemodialysis.
2. METHODS
2.1. Participants and Procedures
Study population included 90 hemodialysis patients from Nephrology and Dialysis Unit at University and other Hospital of Messina. The sample consisted of 51 men and 39 women with mean age of 66.2 S.D. = 13.6. This observational analysis was conducted with all the available patients, and the study protocol was explained during the Hemodialytic session by a physician. Every patients signed an informed consent to take part in the study.
2.2. Measures
Every patients answered to a clinical interview with the aim to reveal other organic disease, presence of psychopathological trait, and years of dialysis treatment.
The psychological protocol given to patients was made up of the following:
The Ego Functioning Experience Questionnaire, E.F.E. (Settineri S., Mallamace D., Mento C., 2009), was developed to evaluate Ego Strength.
Psychometric characteristics of the E.F.E. Questionnaire: The original pool of 30 items for the E.F.E. Questionnaire, was rationally developed by the authors. Items consisted of statements hypothesized to be related to positive and negative emotions, insight of illness, compliance and social functioning. Initially, 30 items were discussed and examined for clarity of expression and ambiguities, and subsequently a set of 21 items were retained for the subsequent steps of Questionnaire development. Following a Factor Analysis, 15 of 21 items were retained and constitute the final Questionnaire. Participants were asked to rate each item on a 6 point Likert scale ranging from 0 = “not at all” to 5 = “very much” in terms of how well the items corresponded to their beliefs about themselves.
The Defense Mechanisms Inventory, D.M.I. is a psychological test, was used to evaluate the defense mechanisms used by the people [31,32]. The test identifies 5 defensive styles with different sets of defense mechanisms:
1) TAO, Turning against object: this set of mechanisms, included deals with conflicts through attacking a real or presumed external frustrating object. Such classical defense mechanisms as displacement and identification with aggressor can be included in this category.
2) PRO, Projection: this set of mechanismis, consists in the attribution of negative characteristics or intent to an external object without unequivocal evidence.
3) PRN, Principalization: this set of mechanismis, deals with conflicts through the splitting of thought content from affect which is repressed. Defense mechanisms as rationalization, intellectualization and isolation fall in this category.
4) TAS, Turning against self: this set of mechanismis, includes those defense mechanisms that handle conflicts through directing aggression toward the subject himor herself. Masochism is an example of defense mechanism in this category.
5) REV, Reversal: this set of mechanisms, deals with conflicts responding in a positive or neutral way to a frustrating object that might rather evoke a negative reaction. Reaction formation, denial and repression are defense mechanisms included in this category.
The Self-Liking and Self-Competence Scale is a psychological scale, is made by 20 items with multiple answers, is based on the conceptualization of global selfesteem as consisting of two dimensions: a sense of social worth, called self-liking and a sense of personal efficacy, called self-competence [33].
2.3. Statistical Analysis
Data was analyzed using the Statistical Package for Social Sciences (SPSS) version 16.0. The preliminary measures of sampling adequacy Kaiser-Meyer-Olkin and Bartlett test of Sphericity is significant (p < 0.001) and demonstrated adeguate normality of the set of distributions of sample. The Exploratory Factor Analysis (EFA) of the Questionnaire EFE is an exploratory analysis included principal axis analysis by the rotation method called Quartimax [34]. The correlations is calculated between principal factors of the E.F.E and other variables comprised in this study protocol.
3. RESULTS
The sociodemographic characteristics of subjects are summarized in Table 1. The results of the Exploratory Factor Analysis (with Quartimax rotation with Kaiser normalization) yielded a first solution, four factor explaining 41.47% of the total variance. Factor loadings of the 15 items of the E.F.E. Questionnaire, items retained after the analysis are showed in Table 2. The six tem that failed to load is: “I accept the treatment for my disease”, “I am interested about what happens around me”, “In is easy for me to stay with others”, “I am conscious about my disease”, “I have no-one to call when I have problem”, “I think that dialysis influences my personal situation”. In the study, values with weight > 0.500 were accepted for the number of our sample (n = 90). An examination of the initial eigenvalues of the reduced matrix and their corresponding estimated proportions of variance accounted for, suggested the retention of a fourfactor solution.
The first factor that explain 21.35% of variance, included items related to family worries, discouragement, anxiety, thought focused on disease, very bad mood, is called “Need of Ego support”. The second factor that explain 11.89% of variance, included items that pertained to joy to live, behaviour that improves health. In this factor items relating to negative emotions (irritabil-
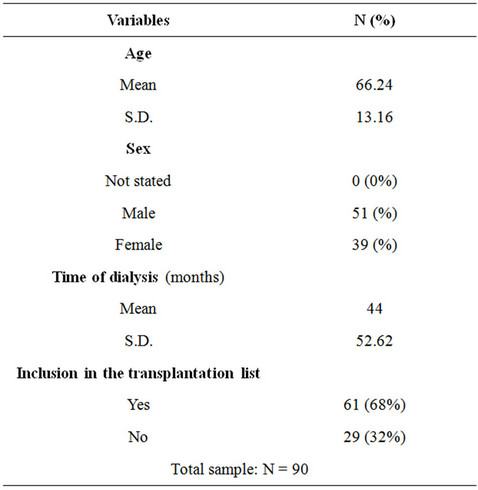
Table 1. Characteristics of hemodialysis patients.
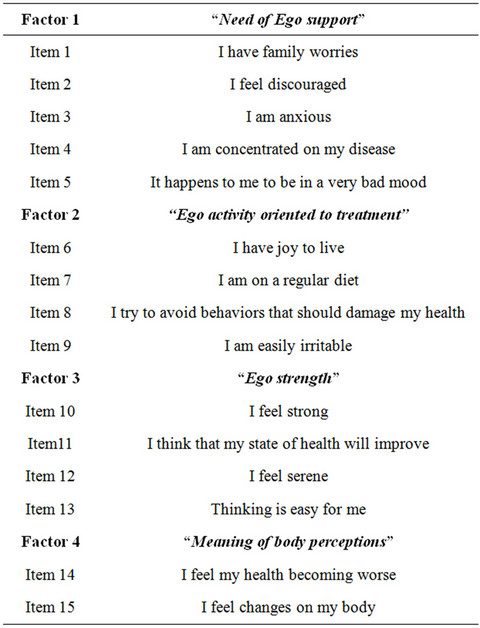
Table 2. 15 Items of the EFE structured by the Exploratory Factor Analysis (EFA).
ity) are inversely related, is called “Ego activity oriented to treatment”.
The third factor that explain 9% of variance, included items related to positive emotions, good reflective ability, optimism about state of health, is called “Ego strength”. The fourth factor included items related to perceptions about body changes and state of health, is called “Meaning of body perceptions”. Six items of the EFE Questionnaire failed to load clearly on these factors. The remaining 15 items had unique loadings on their respective factors ranging from –0.559 to 0.790. This empirically four-factor structure differed from the hypothesized five component structure of Ego functioning experience construct. However, the resulting factors meaningfully reflected the proposed construct.
The evaluation for the reliability of E.F.E. Questionnaire, we calculated of Cronbach’s Alpha of each factor. The coefficients obtained, showed an internal consistency for all the factors except the fourth factor. Probably a further examination, with greater samples will show an internal consistency also for the fourth factor.
The correlation coefficients between the E.F.E. Questionnaire factors (three factors) and other measures, showed a direct correlation with the first factor and “turning against object” TAO of the DMI test (correlation is significant at the 0.001 level) and an inverse relation with set mechanisms of “Principalization”, PRN of the DMI (correlation is significant at the 0.005 level). The correlations of the second and the third factors with other measures, were not statistically significant. No relations were found about other variables.
4. DISCUSSION
An important component of EFE Questionnaire turns around an organization of items expressing family worries, discouragement, anxiety, thoughts focused on disease, very bad mood. This set is the core of the questionnaire and explain most of the variability compared to other factors. The first factor is called “Need of ego support”. The average score of the items composing the factor varies between 9 and 19 and it means that subjects with scores below 9 does not require any support, while those with scores above 19 require ego support. The factor called “Ego activity oriented to treatment” consists of items about the joy of living and positive attitudes towards health, follow the requirements of a diet. It is important factor inversely related with negative emotions. The average score of the items composing the factor varies between 9 and 15, and it means that individuals with lower scores than 9 present a poor compliance and thus require greater attention, while those with scores above 15 have a good compliance.
The nuclear factor called “Ego strength” is the heart of the EFE questionnaire, and consists of items about positive emotions, optimism, good reflective ability. The average score of the items composing the factor is between 7 and 13, and it means that subjects with scores less than 7 have a low Ego strength, indicating the need for social support.
Interestingly, the factors correlated with the defensive style of DMI showed a direct relationship to defensive style TAO. In this case, defensive style of TAO, relating to dependent personality traits, are linked to aggressiveness and irritability, confirm the data already found in the core of factor 1, highlighting the need for psychological support in these patients. Another mechanisms set is defensive style of PRN, Principalization style, which implies the presence of logical processes with more mature defense mechanisms. This data shows how those patients who need to be supported have less access to more mature defense mechanisms and logical processes, eg. mechanisms of rationalization that are involved, by some subjects, in attempts to work out the disease [9,35].
The indication an inverse correlation with the self-esteem score indicating how those who need psychological support have a low self-esteem [23]. These elements reinforce the goodness of the construct found by the questionnaire of the Ego strength and statistical data obtained appear logical by the scientific literature [6,12,25,26,36].
In the study the second factor represents an independent core and indicates patients with awareness of disease and, it is suggestive for a better compliance, resulting in greater adherence to dialysis treatment and better relationship with hospital staff. Indeed, items about negative emotions eg. irritability of mood states that makes doctor-patient relationship harder, show a behavior indirectly are sensibility inversely with this core. This variable, among others, represents in the literature a specific symptom related to mood states, and highlights in patients greater difficulties in relation to acceptance of the disease eg. diagnosis, and to the consequent development of dialysis [7,13,37].
The Ego strength present a core group of emotion for the adaptation [2-4,38]. The sensibility with the age variables, is plausible, even compared to that normally with older age, arise new variables of life in relation to family warries, decreased social support, feelings of discouragement and reducing the chances of the transplant list.
5. CONCLUSIONS
Our data suggest that the first factor can be considered a therapeutic index, as it indicates, with high scores, a clear indication to Ego support, e.g. the presence of cases of depression and other relational problems. Unlike to need of support of the Ego, the aspects oriented to treatment be considered “prognostic factor” as it marks the difference between the presence or absence of Ego activeity oriented to treatment eg. aspects of the adequate compliance. The third aspect in considered “rehabilitative” marks the presence or absence of Ego strength, and when the score is low it highlights the need for social support.
Ego strength is what should be increased for a good compliance [25,26]. This is possible through two key interventions such as set up of programs for individual or group psychological support and, where detected, the elimination of any psychopathological components such as anxiety or depression by a pharmacological treatment [20,35,37]. Such medical attention, means the possibility of achieving better compliance with all patients, that in dialysis could be translated into participating in their treatment plan with greater awareness and regularity in medical prescriptions, diet and time of dialysis [28,29, 38].
This study is used to highlight the possibilities of detecting easily, through a simple questionnaire patients with kidney disease who need psychological support. The possibility of non-compliance to treatment is, in fact, put in relation to the presence of negative emotions e.g. anger and feelings of discouragement, the young age, family warries, lack of insight of illness and are far from health [13,24].
Focusing attention to ego strength in chronic patients, is therefore important, because a lower presence is indicative of poor compliance, but also of a worsening of the psychiatric symptoms evolution toward to demoralization, anxiety and depression, with consequent costs for public health.
6. ACKNOWLEDGEMENTS
There are no relationships between authors and any companies that may have financial interest in the information contained in the manuscript.
REFERENCES
- Vaillant, G.E. (1971) Theoretical hierarchy of adaptive ego mechanisms. Archives of General Psychiatry, 24, 107-118. doi:10.1001/archpsyc.1971.01750080011003
- Lazarus, R.S. (1991) Emotion and adaptation. Oxford University Press, New York.
- Hillman, J. (1999) The force of character. Random House, New York.
- LeDoux, J. (1996) The emotional brain: The mysterious underpinnings of emotional life. Simon and Schuster, New York.
- Sanz Guajardo, D., Orte, L., Gomez-Compderà, F., Fernandez, E., Aguilar, M.D., Làzaro, P. and Inesir, Group. (2006) Quality of life in patients with chronic renal failure influence of nephrologist’s early intervention and predialysis clinical visit consultation. Nephrology, 26, 56-65.
- Sayin, A., Mutluay, R. and Sindel, S. (2007) Quality of life in hemodialysis, peritoneal dialysis and transplantation patients. Transplantation Proceedings, 39, 3047- 3053. doi:10.1016/j.transproceed.2007.09.030
- Friend, R., Hatchett, L., Shneider, M.S. and Wadhwa, N.K. (1997) A comparision of attributions, heath beliefs and negative emotions as predictors of fluid adherence in renal dialysis patients: A prospective analysis. Annals of Behavioral Medicine, 19, 344-347. doi:10.1007/BF02895152
- Rogers, C. (1951) Client-centered therapy: Its current practice, implications and theory. Constable, London.
- Folkman, S. and Moskowitz, J.T. (2000) Positive affect and the other side of coping. American Journal of Psychology, 55, 647-654. doi:10.1037/0003-066X.55.6.647
- Fowler, C. and Baas, L.S. (2006) Illness representations in patients with chronic kidney disease on maintenance haemodialysis. Nephrology Nursing Journal, 33, 173-174, 179-186.
- Dvison, S.N. (2007) The prevalence and management of chronic pain in end-stage renal disease. Journal Palliative Medicine, 10, 1277-1287. doi:10.1089/jpm.2007.0142
- Zoccali, R., Bellinghieri, G., Mallamace, A., Muscatello, M.R.A., Bruno, A., Santoro, D., Mallamace, D., Barillà, G.P., Scardamaglia, P., La Torre, D. and Meduri, M. (2006) Defence mechanisms in hemodialysis, dependent patients. Clinical Nephrology, 65, 119-123.
- Cukor, D., Cohen, S.D., Petersonr, A. and Kimmel, P.L. (2007) Psychosocial aspects of chronic disease: ESRD as a paradigmatic illness. Journal of the American Society of Nephrology, 18, 3042-3055. doi:10.1681/ASN.2007030345
- Livneh, H. and Antonak, R.F. (1997) Psychosocial adaptation to chronic illness and disability. Aspen Publishers, Giathersburg.
- Thong, M.S.Y., Kaptein A.A., Krediet, R.T., Boeschoten, E.W. and Dekker, F.W. (2007) Social support predicts survival in dialysis patients. Nephrology Dialysis Transplantation, 22, 845-850. doi:10.1093/ndt/gfl700
- Patel, S.S., Shah, V.S., Peterson, R.A. and Kimmel, P.L. (2002) Psychosocial variables, quality of life, and religious beliefs in ESRD patients treated with hemodialysis. American Journal of Kidney Disease, 40, 1013-1022. doi:10.1053/ajkd.2002.36336
- Symister, P. and Friend, R. (2003) The influence of social support and problematic support on optimism and depression in chronic illness: A prospective study evaluating self-esteem as a mediator. Health Psychology, 22, 123- 129. doi:10.1037/0278-6133.22.2.123
- Timmers, L., Thong, M., Dekker, F.W., Boeschoten, E.W., Heijmans, M., Rijken, M., Weinman, J. and Kaptein, A. (2008) Illness perceptions in dialysis patients and their association with quality of life. Psychology & Health, 23, 679-690. doi:10.1080/14768320701246535
- The Diabetes Research in Children Network (DirecNet) Study Group (2006) Psychological aspects of continuous glucose monitoring in pediatric type 1 diabetes. Pediatric Diabetes, 7, 32-38. doi:10.1111/j.1399-543X.2006.00142.x
- Bagby, R.M., Quilty, L.C. and Ryder, A.C. (2008) Personality and depression. Canadian Journal of Psychiatry, 53, 14-25.
- Rothbaum, F., Morling, B. and Rusk, N. (2009) How goals and beliefs lead people into and out of depression. Review of General Psychology, 13, 302-314. doi:10.1037/a0017140
- Wisco, B.E. (2009) Depressive cognition: Self-reference and depth of processing. Clinical Psychology Review, 29, 382-392. doi:10.1016/j.cpr.2009.03.003
- Gotlib, I.H. and Joormann, J. (2010) Cognition and depression: Current status and future directions. Annual Review of Clinical Psychology, 6, 285-312. doi:10.1146/annurev.clinpsy.121208.131305
- Chan, R., Brooks, R., Erlich, J., Gallagher, M., Snelling, P., Chow, J. and Suranyi, M. (2011) Studying psychosocial adaptation to end-stage renal disease: The proximaldistal of health-related outcomes as a base model. Journal of Psychosomatic Research, 70, 455-464. doi:10.1016/j.jpsychores.2010.11.005
- Folkman, S. (2008) The case for positive emotions in the stress process. Anxiety Stress Coping, 21, 3-14. doi:10.1080/10615800701740457
- Fredrickson, B.L. (2006) Unpacking positive emotions: Investigating the seeds of human flourishing. Journal of Positive Psychology, 1, 57-59. doi:10.1080/17439760500510981
- Rabkin, J.G., Mcelhiney, M., Moran, P., Acree, M. and Folkman, S. (2009) Depression, distress and positive mood in late-stage cancer: A longitudinal study. Psycho Oncology, 18, 79-86. doi:10.1002/pon.1386
- Chan, R., Steel, Z., Brooks, R., Heung, T., Erlich, J., Chow, J. and Suranyi, M. (2011) Psychosocial risk and protective factors for depression in the dialysis population: A systematic review and meta-regression analysis. Journal of Psychosomatic Research, 71, 300-310. doi:10.1016/j.jpsychores.2011.05.002
- Browne, T. and Merighi, J.R. (2010) Barriers to adult hemodialysis patients’ self-management of oral medications. American Journal Kidney Disease, 56, 547-557.
- Marsch, C.M., Goncalves, L.F. and Barras, E. (2006) Healt-related quality of life among haemo-dialysis patients relationship with clinical indicators, morbility and mortality. Journal of Clinical Nursing, 15, 498-504. doi:10.1111/j.1365-2702.2006.01349.x
- Ihilevich, D. and Gleser, G.C. (1986) Defence mechanisms. Their classification, correlates, and measurement with the defence mechanim inventory. DMI Association Ossowo.
- Fioriti, G. and Gentili, P. (1994) Defence mechanism inventory. Italian Version. OS, Giunti.
- Tafarodi, R.W. and Swann Jr., W.B. (1995) Self-liking and self-competence as dimensions of global self-esteem: Validation of a measure. Journal of Personality Assessment, 65, 322-342. doi:10.1207/s15327752jpa6502_8
- Pedhazur, E.J. and Schmelkin, L.P. (1991) Measurement, design, and analysis: An integrated approach. Lawrence Erlbaum Associates, Hillsdale.
- Johnson, S. and Dwyer, A. (2008) Patient perceived barriers to treatment of depression and anxiety in hemodyalisis patients. Clinical Nephrology, 69, 201-206.
- Taskapan, H., Ates, F., Kaya, B., Emul, M., Kaya, M., Taskapan, C. and Sahin, I. (2005) Psychiatric disorders and large interdialytic weight gain in patients on chronic hemodialysis. Nephrology (Carlton), 10, 15-20. doi:10.1111/j.1440-1797.2005.00321.x
- Baris, A. and Beril, A. (2009) Depression and nonadherence are closely related in dialysis patients. Kidney International, 76, 679.
- Cukor, D., Rosenthal, D.S., Jindal, R.M., Brown, C.D. and Kimmel, P.L. (2009) Depression is an important contributor to low medication adherence in hemodialyzed patients and transplant recipients. Kidney International, 75, 1223-1229. doi:10.1038/ki.2009.51