C. Erfurt et al. / HEALTH 2 (2010) 237-245
Copyright © 2010 SciRes Openly accessible at http://www.scirp.org/journal/HEALTH/
238
attitude, the rejection or ignoring of the child by the
parents or parental figures—a behavior that seriously
damages the child’s sense of personal identity and self-
esteem. Also included is emotional neglect, when the
parents or caregivers fail through negligence to provide
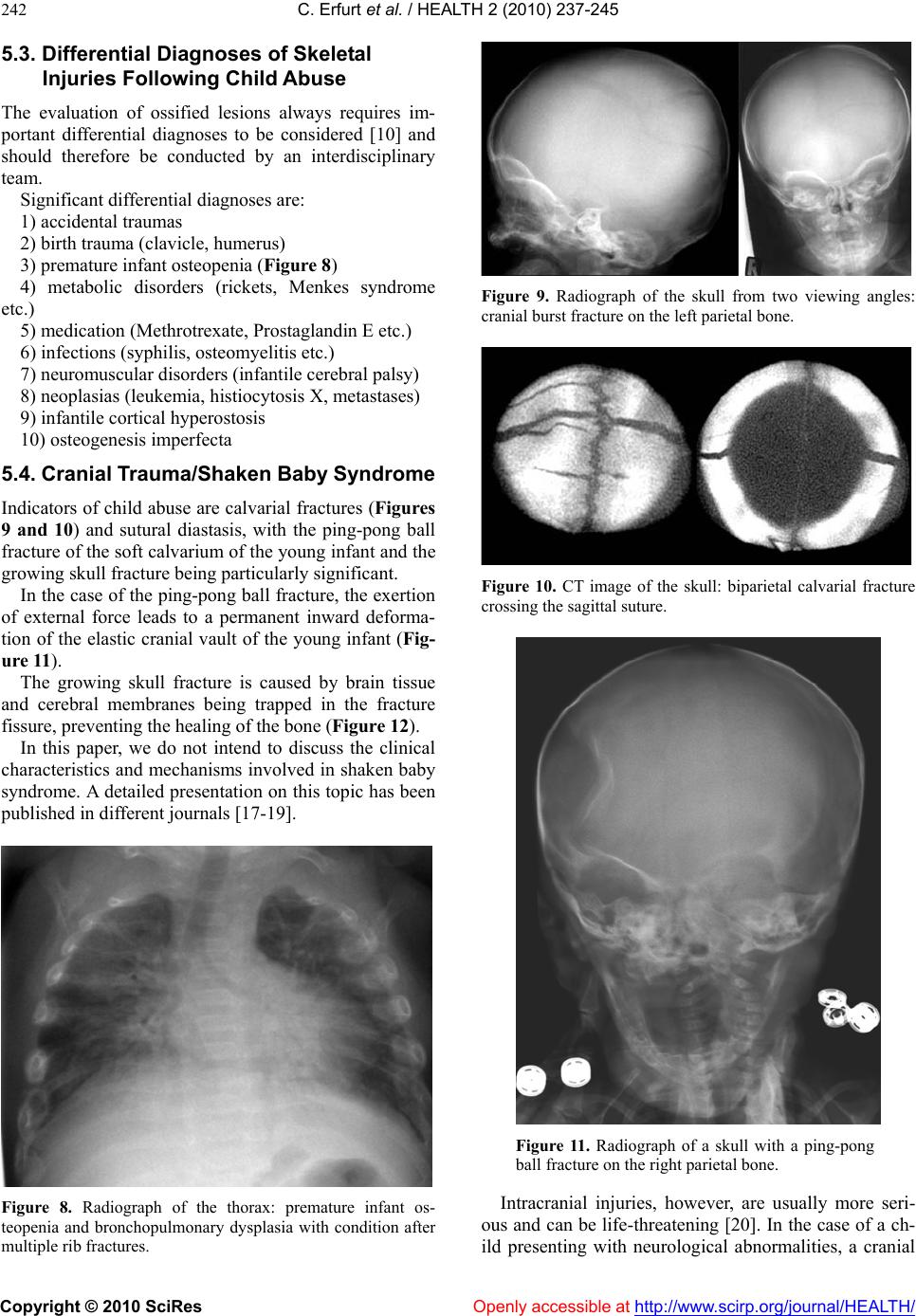
the child with the family atmosphere required for healthy
emotional development (for example through constant
emotional coldness or ignoring the child, as silent forms
of child abuse).
2.3. Physical Neglect
Physical neglect means that the parents or other caregiv-
ers fail completely or partially to provide for the child’s
survival or well-being, i.e. health care, nourishment, clo-
thing, healt h pr omotion, pr ot ection and supervisio n.
2.4. Sexual Abuse
Sexual abuse is the involvement of children and adoles-
cents in all types of sexual activity and/or sexual explo i-
tation by adult reference persons to whom the child
cannot give informed consent owing to ignorance, de-
pendence, developmental immaturity or fear.
Child pornography is a form of sexual abuse, as is
also the confrontation of minors with representations of
sexuality in a manner that is inappropriate to the child’s
stage of development. In every case, responsibility for
such mistreatment is borne by the perpetrator. Incest is a
special form known as ‘intrafamilial child sexual abuse’,
committed by a member of the family group. Child sex-
ual abuse also refers to actions performed with the inten-
tion of sexually stimulating a child or using a child for
the purpose of sexual arousal, either of the perpetrator or
of another person.
Children in particular are often unable to speak out—
either because they are insufficiently developed as in-
fants or toddlers, or as a result of fear. A thorough
physical examination in cases of suspected mistreatment
or sexual abuse is an important milestone in both the
diagnosis and ‘therapy’ of the abuse. The detection and
ascertainment of traumatic findings and their attribution
is an important diagnostic criterion in cases of suspected
child abuse.
Infants and toddlers are particularly challenging in
this context. In instances of suspected physical abuse,
the examination should not be restricted solely to the
external inspection of the body, since osseous injuries
are frequently not detected through clinical examination.
A full skeletal survey using radiological imaging tech-
niques can detect or rule out bone lesions resulting fro m
traumatic injury, therefore constituting an essential
component of the investigations in suspected child abuse
cases.
Both action and failure to provide care can constitute
a threat to a child.
The following text briefly deals with the possible
consequences of physical violence. Based on the daily
experiences made by the Doctor of Legal Medicine and
the Pediatric Radiologist it can be said that any form of
physical violence one can think of can also occur when a
child is abused. Typical forms of violence are punches,
kicks, pushes against the wall and the use of objects
(sticks, etc.).
Consequently, the affected children suffer from inju-
ries such as hematomas, swellings of soft parts or inju-
ries to the soft parts and skin (contused wounds or cuts).
Additionally, there can be hidden injuries, such as dam-
aged organs and fractures.
A special form of physical abuse is the shaken baby
syndrome. The term “Whiplash shaken baby syndrome”
goes back to Caffey [4]. Severe shaking of a baby leads
to strong shearing forces due to acceleration and decel-
eration. Babies and toddlers are not able to hold their
head, which is very heavy compared with their body,
when they are shaken severely. As a result there will be
cranial hemorrhages (subdural and subarachnoid hem-
orrhages), hemorrhages in the retina and lesions of cra-
nial tissue [5]. The shaken baby syndrome can lead to
death. The affecting forces have been determined exten-
sively in the finite element analysis [6]. The scope of
injuries resulting from shaken baby syndrome comprises
not only intracranial injuries, but also frequently injuries
of the skeletal system in particular rib fractures and fin-
ger marks [7]. Based on literature one can assume that
shaken babies show clinically diagnosable symptoms
[8].
The strategy of examination depends on the clinical
situation and the age of the child.
Besides the clinical examination , radiological imaging
examination methods are to be app lied.
3. IMAGING PROCEDURES
Accordingly, we aim to presently discuss the various
uses of radiological diagnostic imaging in this context,
including an assessment of their respective valu e and the
necessary indications.
In instances of clinical suspicion of child abuse, the
following imaging procedures may be used: skeletal
radiography, computer tomography (CT) and/or, pref-
erably, magnetic resonance imaging (MRI) investiga-
tions and sonography [9,10].
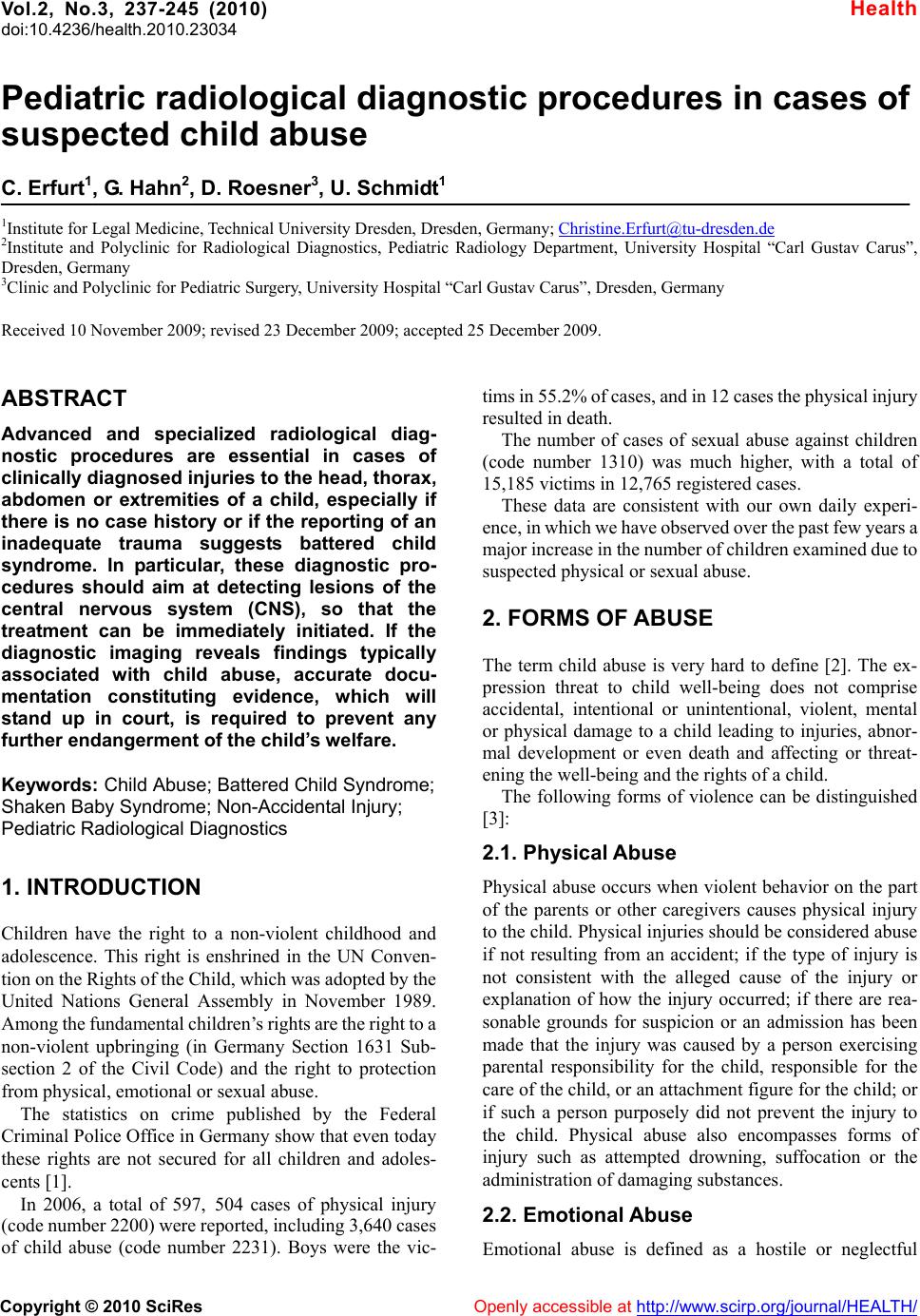
3.1. Full Radiographic Skeletal Survey
A full radiographic skeletal survey should always be
performed in children up to 2 to 3 years old if child
abuse is suspected [11]. All the extremities, the thorax
and pelvis should be x-rayed from one viewing angle
and the cranium, spine and fracture areas should be
x-rayed from two viewing angles (Figure 1). The radio-
graphic images of the extremities should include the