Vol.2, No.3, 200-203 (2010) Health
doi:10.4236/health.2010.23029
Copyright © 2010 SciRes Openly accessible at http://www.scirp.org/journal/HEALTH/
Left ventricular noncompaction associated with
hypertrophic cardiomyopathy and
Wolff-Parkinson-White syndrome
Luis Alday1, Eduardo Moreyra1, Eva Bruno2, Norma Rossi3, Hector Maisuls2
1Divisions of Pediatric Cardiology and Cardiology, Sanatorio Allende, Córdoba, Argentina; lealday@arnet.com.ar
2Division of Cardiology, Children’s Hospital, Cordoba, Argentina
3Division of Genetics, Private Hospital, Cordoba, Argentina
Received 14 October 2009; revised 10 December 2009; accepted 14 December 2009.
ABSTRACT
We report a 35-year-old female patient with hy-
pertrophic cardiomyopathy, left ventricular non-
compaction, and Wolff-Parkinson-White EKG patt-
ern. Several other family members present the
same clinical condition. We speculate that this
phenotype is related to the genotypes PRKAG2
and LAMP2 represented by mutations of the
genes encoding AMP-activated protein kinase
(PRKAG2) and lysosome associated membrane
protein 2 (LAMP2 ).
Keywords: Left Ventricular Noncompaction;
Hypertrophic Cardiomyopathy;
Wolff-Parkinson-White Syndrome
1. INTRODUCTION
Left ventricular noncompaction (LVNC) is the result
from the a rrest in m yocardi al dev elopm ent w ith pe rsist ent
sinusoid tracts interspersed with prominent muscular
trabeculae. Affected patients usually develop congestive
heart failure associated with arrhythmias and systemic
thromboembolism.W e report a proband with mental retar-
dation and peculiar somatic findings, associated LVNC
and hypertrophic cardiomyopathy (HCM). Other family
members were also involved, all of them, the proband
included, had Wolff-Parkinson-White (WPW) syndrome,
suggesting a relationship regarding the etiology of this
LVNC - HCM phenotype overlapping.
2. CASE REPORT
The proband is a 35-year-old female who had been fol-
lowed since infancy. She was referred to us for a heart
murmur and congestive heart failure. Clinical examina-
tion at presentation was compatible with moderate to
severe mitral regurgitation. There was cardiomegaly and
signs of pulmonary venous hypertension on the chest
X-ray. The EKG showed a WPW pattern with extremely
high voltage. Cineangi ography reveal ed a hypercontractile
left ventricle without outflow tract obstruction, moderate
to severe mitral regurgitation, and a never-seen-before
cont our wh ich made i t rese mble a “porcu pine ” since there
were heavy trabeculations leaving thin spaces between
them as if they were wheel spokes radiating from the
center to the periphery of the ventricular cavity. On the
basis of the a n gi o gra phic findings this pat i ent’s heart was
called a “spongy” heart because was thought to be the
result of persistence of embryonic myocardium [1].
The patient was treated for heart failure until early
childhood. There was clinical i mprovement with decreasi ng
mitral regurgitation as judged by auscultation. She re-
mained symptom free for several years and she had
non-obstructive HCM with mild mitral insufficiency
upon echocardiographic examination. She continued
regular follo w- up visits and the echocardiograms showed
progression to a dilated stage. Eight years ago she was
admitted with pulmonary edema and frequent ventricular
extrasystoles. Following treatment she was in NYHA
functional class II and was discharged. Occasional re-
missions occurred caused by treatment non-com pliance.
Presently, she is in functional class III and has slight
mental retardation. She has lower than normal stature, a
short neck, low posterior hairline, and a high palate.
Clinical genetics evaluation suggests the diagnosis of
Noonan syndrome. Cardiovascular examination shows, a
mitral regurgitation murmur and gallop rhythm. Chest
x-ray a nd E KG pr ese nt e d s e ve re ca r di omegaly wi th si g ns
of pulmonary venous hypertension and WPW pattern,
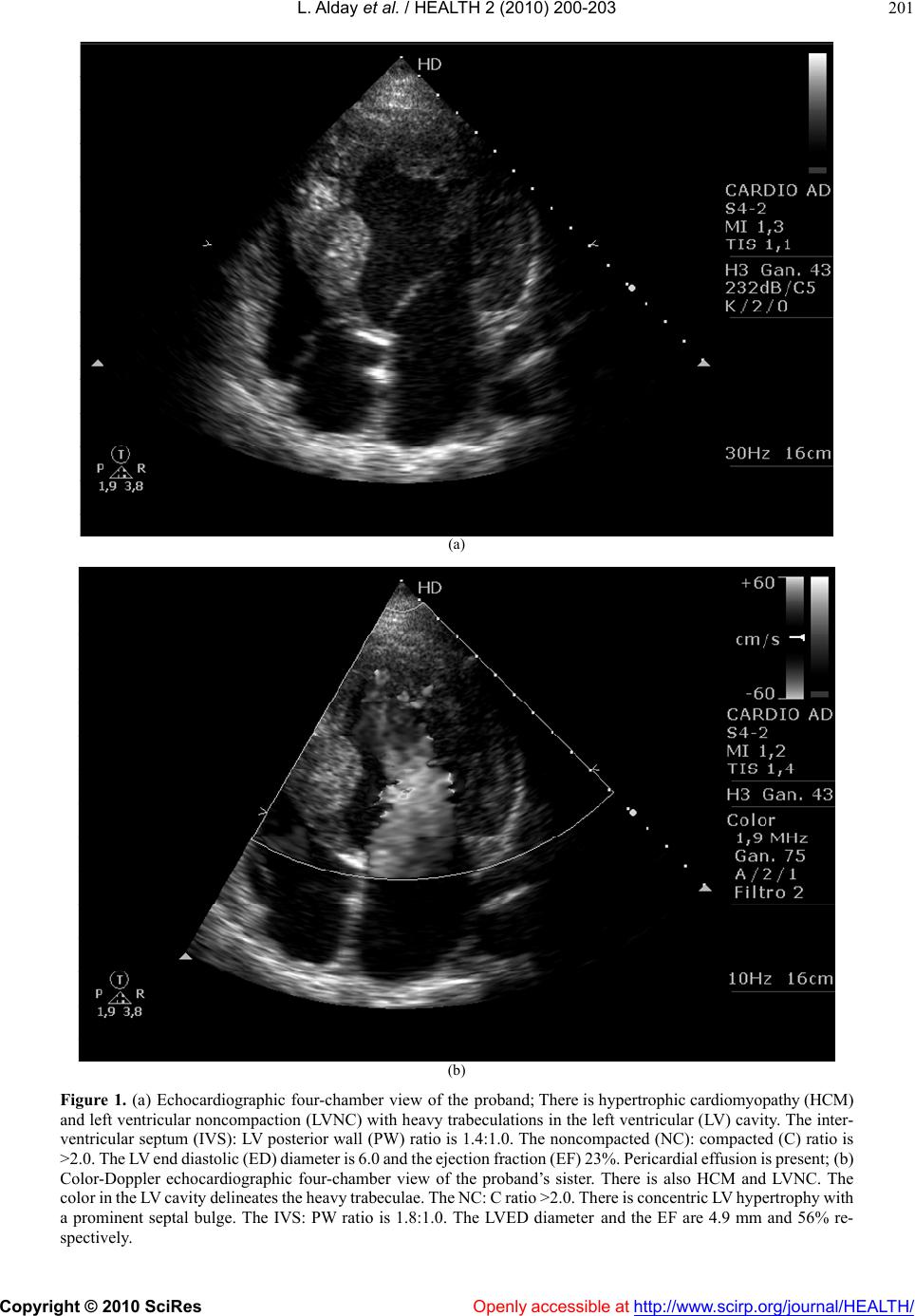
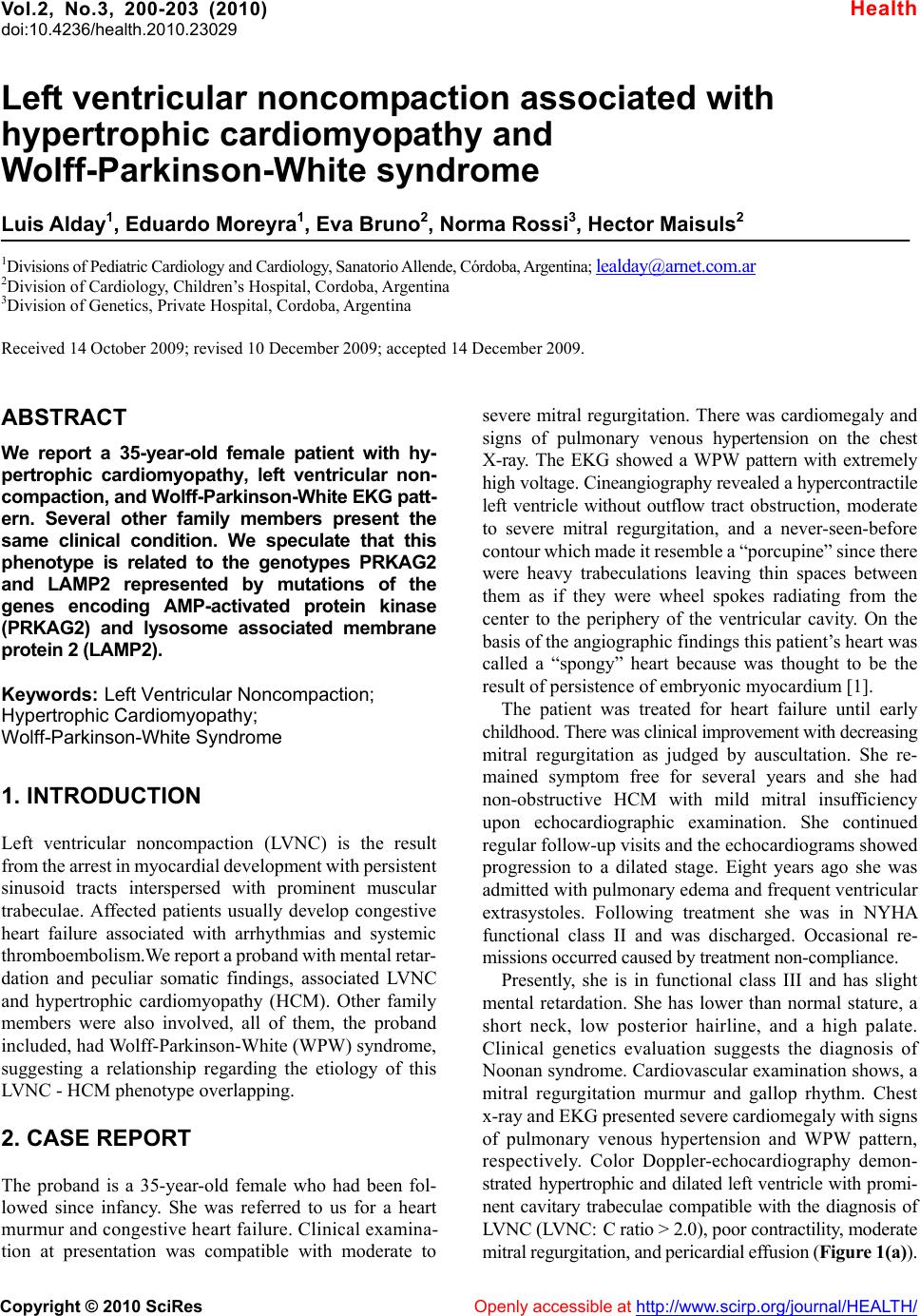
respectively. Color Doppler-echocardiography demon-
strated hypertrophic and dilated left ventr icle with promi-
nent cavitary trabeculae compatible with the diagnosis of
LVNC (LVNC: C ratio > 2.0), poor contractility, moderate
mitral regur gitation, and pericardial ef fusion (Figur e 1(a)).