Case Reports in Clinical Medicine
Vol.3 No.1(2014), Article ID:42241,5 pages DOI:10.4236/crcm.2014.31013
Gastric laceration after cardiopulmonary resuscitation: A case report
1Hospital São Paulo-University Hospital of Federal University of São Paulo, São Paulo, Brazil; *Corresponding Author: molosiri@hotmail.com
2Department of Cardiology, Federal University of São Paulo, São Paulo, Brazil
Received 10 November 2013; revised 8 December 2013; accepted 31 December 2013
ABSTRACT
The cardiopulmonary resuscitation (CPR) persists as the best practice to maintain cerebral and coronary perfusion after cardiac arrest. Due to the chest compressions and ventilation maneuvers during resuscitation, there are common complications reported. Abdominal organs injuries occur in approximately 30% of patients, although studies show that they are under diagnosticated. The aim of this article is to report a case of massive digestive hemorrhage by gastric laceration after cardiopulmonary resuscitation, due to the event severity and rare clinic diagnostic. A 75-year-old Caucasian man suffered a sudden malaise and cardiac arrest and transferred to an Emergency Unit (EU). The set of measures recommended by Advanced Cardiac Life Support (ACLS) was performed. Despite no resistance to the passage of nasogastric survey and spontaneous healing of fresh blood exteriorization, an endoscopy showed ulcers in gastric notch with clots adhered and active blood. There was no track record of liver or gastrointestinal diseases on this patient, identifying a gastric laceration after cardiopulmonary resuscitation. The mechanism by which the gastric laceration after CPR occurred is uncertain. Nevertheless, some precipitating factors are considered such as positioning of the patient during CPR, ideal point of compressions and ventilation pressure. In conclusion, this event is rare with a hard diagnostic however that could be avoided and minimized with preventive measures.
Keywords:Cardiac Arrest; Ventilation; Emergency Care; Complications; Gastric Injury; Cardiopulmonary Resuscitation
1. INTRODUCTION
The cardiopulmonary resuscitation (CPR) persists as the best practice to maintain cerebral and coronary perfusion after cardiac arrest. It is the initial step recommending inside the set of measures recommended to Basic Life Support (BLS) and Advanced Cardiac Life Support (ACLS) [1].
Due to the chest compressions during resuscitation, there are common complications which have already been reported. Studies [2] showed that skeletal injuries of ribs and sternum are the most frequently complication in adults, reaching a range from 13% to 97% and 1% to 43% respectively. In infants, studies demonstrated that changes in CPR techniques introduced in 2005 increased the incidence of rib fractures in this population [3]. Kim et al. [4] conducted a prospective cross-sectional, multicenter study in the emergency departments showing that the frequency of this event is variable from one hospital to another hospital. It depends on several factors such as gender and participation of non-physician chest compressors. Also, no difference in arrest location, duration of CPR and number of compressors was seen between rib fracture and non-rib fracture groups. Nor did the use of mechanical chest compressions with LUCASTM device seem to have different incidence [5].
Other complications can occur during the cardiopulmonary resuscitation, but less described in studies. Complications of abdominal organs due to cardiopulmonary resuscitation occur in approximately 30% of patients and include gastric dilatation, pulmonary and splenic distress. Gastric injuries are classified as rare ones, although studies showed that they are under diagnosticated [6].
The aim of this article is to report a case of massive digestive hemorrhage by gastric laceration after the cardiopulmonary resuscitation, due to the event severity and rare clinic diagnostic.
2. CASE REPORT
A man in his 70, caucasian, retired, natural from São Paulo, Brazil. The patient was hypertensive, obese, with clinically controlled hypothyroidism. He reported not to have other pathologies, including liver and gastrointestinal diseases. He also denied alcoholism, smoking or use of nonsteroidal anti-inflammatory drugs.
He suffered a sudden malaise and cardiac arrest that was immediately identified for a doctor, who started thoracic compression e mouth-to-mouth ventilation. After 10 minutes of CPR, an ambulance transferred to an Emergency Unit (EU), where he arrived in a total of 20 minutes, without automated external defibrillator (AED).
He was admitted at Emergency Unit in cardiac arrest and identified rhythm of ventricular fibrillation (VF), and was taken care of according to the ACLS protocol. The patient received electrical cardioversion with 200 J, thoracic compression, drugs, ventilation with bag-valvemask unit and orotracheal intubation. The cardiac arrest was reverted to sinus rhythm after 10 minutes of the admission. Then, he presented arterial hypotension and was identified thru electrocardiogram (ECG) a S-T segment elevation in DII, DIII, AvF, V7 and V8 that corresponds to the lower and dorsal myocardial wall. Therefore, the patient stayed in cardiac arrest during 30 minutes, being 20 minutes pre-hospital.
The patient stayed in invasive mechanical ventilation, sedated and in use of noradrenaline. He was normal colored, dehydrated 1+/4+, auscultation with discrete crackles in lower lung in both hemithorax, cardiac auscultation without alterations, symmetric peripherals pulses with reduced range, lentify capillary refill (4 seconds) and cold extremities.
A survey nasogastric was introduced without resistance to passage, that present large amount of fresh blood, which ceased spontaneously.
At inspection, he did not present traumatic injuries in oropharyngeal region and did not occur any complications during the intubation. Any alterations were observed at thorax radiography.
As the patient was not bleeding, he was forward to hemodynamic to do coronary angiography, due hypothesis cardiac arrest after acute myocardial infarction. At the exam, was seen the total occlusion of right coronary artery and parietal irregularities in the others coronary arteries. During the procedure, he presented hematemesis, with massive hemorrhage, without heal spontaneous, with hemodynamic repercussion and was necessary stop the procedure.
Was realized endoscopy that showed ulcers in gastric notch with clots adhered and active blood (Figure 1), which was controlled after sclerotherapy with epinephrine.
The patient received crystalloids and transfusion of erythrocytes. At the first 12 hours, the hemoglobin decreased 5 points. He improved the hemodynamic and didn’t receive platelet aggregation inhibitors or anticoagulant therapy.
The echocardiogram showed ejection fraction of 55%, in subjective evaluation, without segmental dysfunction.
At third day of hospitalization, was realized a new endoscopy to second look that showed deep lesion on gastric mucosa of 6cm between the lesser curvature and posterior wall and superficial lesions in other regions, without active blood.
At fifth day of hospitalization in ICU the patient was extubated, but evolved septic shock, and after 106 days, evolved to multiple organs failure.
3. DISCUSSION
The cardiopulmonary resuscitation (CPR) has been widespread, with a great recommendation of this knowledge including between laypersons. As a consequence, the possibility of technical error can grow substantially, if had not an efficient training. Among them, besides the inefficiency in maintain supply of oxygen to issues accordingly, can also occur direct iatrogenic injuries [1].
The chain of survival was added a new link, the realization of organized cardiopulmonary post-resuscitation
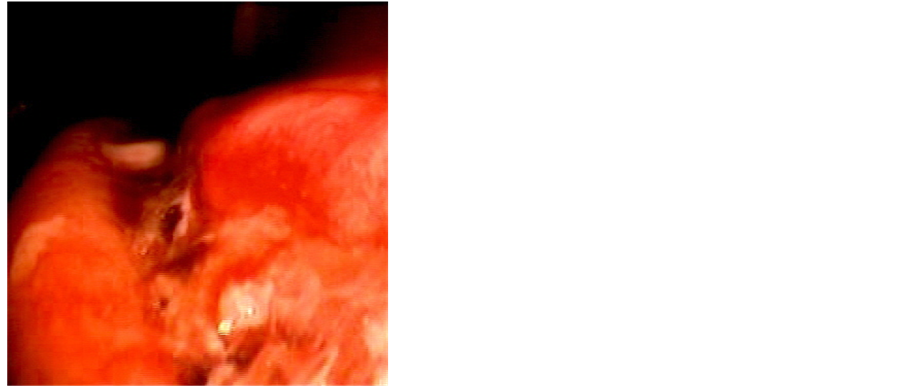
Figure 1. Endoscopy view of gastric laceration bleeding (figure caption).
animation care, since seriously ill subject need a multidisciplinary assistance plan to take care of various amendments [7].
The ventilator support is recommended and is an important component in CPR along thoracic compression of high quality and defibrillation in a shockable rhythm. The ventilation during CPR ensures enough oxygen and removes carbon dioxide [8].
The complications involving abdominal viscera after CPR occurred in approximately 30% of patients [6]. Among the complications, stand out ribs and sternum fractures, mediastinal emphysema, pneumothorax and, less common, abdominal viscera injuries like liver, spleen and stomach [1].
Gastric laceration happens up to 12% of individuals that were submitted to CPR maneuvers without success and forwarded to autopsy, beyond ribs and/or sternum fractures in 53% of the cases [1,5]. The gastric perforation after CPR is rare (0.1%), however, this occurred because is clinically less diagnosed [6,9]. In according with Dias et al. [1], in some series of autopsy, the occurrence of gastric laceration reaches 10% of the cases.
The mechanism by which the gastric laceration after CPR occurred is uncertain. However, some considerations are highlighted, like highly pressure and gastric distension. The gastric dilatation decreases the function of cardia and pylorus relax, resulting in difficult to mobilize the air in stomach, generating vulnerably condition to traumas, when submitted to pressure, as occurred in heart massage [10-12].
As precipitating factors of gastric distension stand out the application of the cardiac massage of the ideal point below, head and neck of patients’ incorrect positioning during the airway maneuver and ventilation pressure excessively high. The maneuvers of thoracic compression, if does with full stomach or distended by gas, can cause a rapid rise of gastric pressure and lead to viscera rupture [1].
Other mechanisms involved in ventilation contribute to increase the gastric dilatation. As an example, mouthto-mouth ventilation [9], the bag-mask ventilation [1,6], the laryngeal mask [8], nasal catheter of oxygen5 and the esophageal intubation [6,9-11].
The American Heart Association (AHA) recommends a rate of thoracic compression/ventilation of 30:2 in all age patients, attended by one or two rescuers in adults and 15:2 with two rescuers in children. After the achievement of artificial airway with advanced support, should do at least 100 thoracic compressions per minute and 8 to 10 ventilations per minute, without disruption of compressions, after definitive airway [13].
The professional responsible to ventilation should be certain that opened properly the airway passage with head elevation and chin inclination, lifting the jaw against the mask and holding the mask without the face, making a tight seal [13].
In adults, the ventilation by bag-mask should be such that it produces about 600 ml tidal volume, with elevation of chest rise more than one second. This volume is appropriate to oxygenate and minimize the risk of gastric insufflations [14].
The incorrect form of ventilation with system bagvalve, excessive oxygenation and difficult to ventilate contribute to greater risks and injuries [1,9,10], beyond regurgitation, aspiration and pneumonia; it can also elevates the diaphragm, restricting lung inflation and decreases complacency pulmonary system [14]. The analysis made with corpses organs showed that stomach disrupts when is bagged with 4 liters of air, and is necessary a pressure of 120 to 150 mmHg to develop an injury in gastric wall [9,11].
Besides this, the hyperventilation increases significantly the intrathoracic pressure, decreases coronary perfusion pressure and can reduce the survival rate [8].
The advanced ventilation normally occurred in the second phase of cardiac arrest assistance. During the obtention of definitive airway, the esophageal intubation can cause serious problems as hypoxia increase, gastric hyperdistension and interruption of circulation. Moreover, is important to confirm the tracheal intubation as soon as possible, and that, the lungs should be examined with a stethoscope after epigastrium auscultation [8].
Parka et al. [8] related that hyperventilation was seen in more than 90% of the cases when was realized the auscultation during CPR, and more than 60% involved severe hyperventilation (respiratory frequency > 20 per minute). In particular, the auscultation to confirm the success of intubation was hardly associated with severe hyperventilation.
Other forms of gastric trauma can occur even without stomach distension, as repeated thoracic compressions [10,11], or successive Heimlich maneuvers [9,10,15].
As the intra-abdominal pressure rises, there is compression of veins, reduces venous return, compression of mesenteric system and reduces of venous return to heart, resulting in decreases of cardiac output and consequent less issues perfusion. Furthermore, with the increased of intra-abdominal pressure, the diaphragm is pulled to intra-abdominal cavity, rising the chest pressure [15].
The place of more frequent gastric laceration and rupture is in less curvature [6,11], usually adjacent to gastroesophageal junction. This region has less elasticity than others stomach regions, due less mucosal folds and it is fixed in hepatogastric ligament [9,15]. The gastric dilatation distorts the gastro-esophageal junction and prevents that gas stay at esophagi, but permits the continuous air entrance. Besides, as the point more distorted of stomach is bagged, the pyloric ligaments are obstructed by duodenum folding. As consequence, with obstruction of both sphincter, the stomach breaks [15].
The gastric laceration can generate hemodynamic instability, as happened in this case report, could develop the perforation, mostly if it was subject to new CPR maneuvers. The endoscopy confirms the laceration diagnostics and permits the treatment with epinephrine application [9,10].
The intra-abdominal lesions after CPR required immediately treatment, despites the hemodynamic instability. The prognosis usually is reserved and is directly related to quickness in diagnostic. The viscera rupture should be considerate in patients who are hemodynamic instable after CPR, presents signs like abdominal distension and hyper or hypotension [1].
The passage of gastrointestinal probe after tracheal intubation helps in gastric decompression. The evidence of abdominal distension during or after CPR, whom do not improve with the passage of gastrointestinal probe is a signal of visceral injury. The blood output across the gastrointestinal probe confirms de diagnostics of lesion, could be laceration or rupture, but the absence of bleeding do not discard the clinical status [6,9-11].
The clinical treatment has been the choice in cases of gastric laceration and gastric perforation, being instituted as early as possible [9,10]. However, the surgical treatment associated with anti-bacterial therapy is necessary when there is the perforation with peritonitis [6,9-11].
The most important during CPR would be started prevention measures of gastric lesion, as ventilation with positioning adequate of head and chin, well adaptation of devices airway and normal ventilation, whom permits a air flow with adequate pressure and prevents stomach dilatation. Also the tracheal intubation been quickly and effective with smaller deviation to gastrointestinal tract [9].
The use of continuous capnography has been recommended to confirm the localization of tracheal tube and monitoring the quality of CPR. As cardiac massage, the best way is the execution of the technique correctly, with minimal frequency of compression of 100 per minute, minimal depth of compression of 5 centimeters in adults, total return of chest after each compression, minimization of the interruptions in thoracic compressions and to avoid hyperventilation, as recommended by AHA guidelines [13].
Recent studies show that experienced people or certified by Advanced Cardiovascular Life Support have less chances to hyperventilate during a CPR when compared to people untrained and inexperienced. However, in case of tense cardiac arrest, could be difficult to maintain a respiratory frequency of 8 to 10 per minute during CPR, even for people well trained [8].
4. CONCLUSIONS
The gastric laceration after CPR is a rare event and has a difficult diagnostic. However, there are preventive measures for this complication, mainly about the care with the ventilation during maneuvers. Those measures ensure an air flow with adequate pressure and avoid stomach dilatation after CPR maneuvers.
Therefore, it stands out the importance of measures of ventilation to minimize the consequences of hyperventilation or the consequences of inadequate ventilation.
Thus, the divulgation of some measures can prevent and decrease the number of complicating events. In prehospital, it is necessary to promote teaching correct ventilation and thoracic compression and the Basic Life Support. In hospital, an important measure is continuing education about practice procedures in execution of the Advanced Life Support.
REFERENCES
- Dias, L.T., Mendes, L.C.M., Mello, P.M.V.C., et al. (2006) Ruptura gástrica por reanimação cardiopulmonar: Relato de caso. Rev Bras de Terapia Intensiva, 18, 207-211. http://dx.doi.org/10.1590/S0103-507X2006000200017
- Hoke, R.S. and Chamberlain, D. (2004) Skeletal chest injuries secondary to cardiopulmonary resuscitation. Resuscitation, 63, 327-338. http://dx.doi.org/10.1016/j.resuscitation.2004.05.019
- Martin, P.S., Jones, M.D., Maguire, S.A., et al. (2012) Increased incidence of CPR-related rib fractures in infants—Is it related to changes in CPR technique? Resuscitation, 83, Article ID: e109. http://dx.doi.org/10.1016/j.resuscitation.2011.08.034
- Kim, M.J., Park, Y.S., Kim, S.W., et al. (2013) Chest injury following cardiopulmonary resuscitation: A prospective computed tomography evaluation. Resuscitation, 84, 361-364. http://dx.doi.org/10.1016/j.resuscitation.2012.07.011
- Smekal, D., Johansson, J., Huzevka, T., et al. (2009) No difference in autopsy detected injuries in cardiac arrest patients treated with manual chest compressions compared with mechanical compressions with the LUCAS device—A pilot study. Resuscitation, 80, 1104-1107. http://dx.doi.org/10.1016/j.resuscitation.2009.06.010
- Hahn, C.D., Choi, Y.U., Lee, D., Frizzi, J.D., et al. (2008) Pneumoperitoneum due to gastric perforation after cardiopulmonary resuscitation: Case report. American Journal of Critical Care, 17, 388-390.
- Campanharo, C.R.V., Moreira, R.S.L., Batista, R.E.A., et al. (2012) Ressuscitação cardiopulmonar: novas diretrizes de atendimento. Acta Paulista de Enfermagem, 25,483. http://dx.doi.org/10.1590/S0103-21002012000300026
- Park, S.O., Shin, D.H., Baek, K.J., et al. (2013) A clinical observational study analysing the factors associated with hyperventilation during actual cardiopulmonary resuscitation in the emergency department. Resuscitation, 84, 298-303. http://dx.doi.org/10.1016/j.resuscitation.2012.07.028
- Spoormans, I., Hoorenbeecka, K.V., Balliu, L. and Jorensa, P.G. (2010) Gastric perforation after cardiopulmonary resuscitation: Review of the literature. Resuscitation, 81, 272-280. http://dx.doi.org/10.1016/j.resuscitation.2009.11.023
- Campillo-Soto, A., Lirón-Ruiz, R., Torralba-Martínez, J.A., et al. (2007) Rotura gástrica y neumoperitoneo masivo trás resucitación cardiopulmonar por personal no sanitário. Cirugía Española, 81, 49-51. http://dx.doi.org/10.1016/S0009-739X(07)71258-7
- Offerman, S.R., Holmes, J.F., Wisner, D.H., et al. (2001) Gastric rupture and massive pneumoperitoneum after bystander cardiopulmonary resuscitation. The Journal of Emergency Medicine, 21, 137-139. http://dx.doi.org/10.1016/S0736-4679(01)00357-2
- Haslam, N., Campbell, G.C., Duggan, J.E., et al. (2004) Gastric rupture associated with use of laryngeal mask airway during cardiopulmonary resuscitation. British Medical Journal, 329, 125-126. http://dx.doi.org/10.1136/bmj.329.7476.1225
- American Heart Association (2010) Highlights of the 2010 AHA guidelines for CPR and ECC. Circulation. http://www.heart.org/idc/groups/heart-public/@wcm/@ecc/documents/downloadable/ucm_317350.pdf
- Neumar, R.W. (2010) Part 8: Adult Advanced cardiovascular life support: 2010 American Heart Association Guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation, 122, S729-S767. http://dx.doi.org/10.1161/CIRCULATIONAHA.110.970988
- Smally, A.J., Ross, M.J., Huot, C.P., et al. (2002) Gastric rupture following bag-valve-mask ventilation. The Journal of Medicine, 22, 27-29.