Open Journal of Pediatrics
Vol.3 No.3(2013), Article ID:35961,3 pages DOI:10.4236/ojped.2013.33041
Situs invertus totalis in a child with chronic sinusitis*
![]()
University of Nigeria, University of Nigeria Teaching Hospital, Ituku-Ozalla, Enugu
Email: #josephat.chinawa@unn.edu.ng, chuzodi@yahoo.com
Copyright © 2013 Chinawa Josephat Maduabuchi et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 14 June 2013; revised 15 July 2013; accepted 23 July 2013
Keywords: Situs Inversus Totalis; Syndromic; Rare
ABSTRACT
Background: Total situs inversus, (also called situs transversus or oppositus) known as mirror image dextrocardia, is characterized by a heart on the right side of the midline while the liver is on the left side. Situs Inversus Totalis (SIT) is a congenital anomaly characterized by complete transposition of abdominal and thoracic organs. Patients with this anomaly usually lead a normal life. We report a fourteen-year old Nigerian who was found to have dextrocardia with situs inversus totalis while presenting for treatment for a different problem. Conclusion: Situs inversus totalis is a rare finding. This report underscores the need for routine screening by children so that such congenital anomalies can be identified and complications may follow it and avert timely.
1. INTRODUCTION
Situs inversus, first described by Aristotle in animals and Fabricius in humans, is an uncommon anomaly with an incidence varying from one in 4000 to one in 20,000 live births [1,2]. Situs inversus is generally an autosomal recessive genetic condition, although it can be X-linked or found in identical twins [3]. There is a 5% - 10% prevalence of congenital heart disease in individuals with situs inversus totalis, most commonly transposition of the great vessels. The incidence of congenital heart disease is 95% in situs inversus with levocardia [3].
This condition is found to be associated with cardiac and splenic malformations [3]. However in approximately 20% - 25% of patients, associated Primary Ciliary DySkinesia (PCD) and Kartagener’s syndrome may also be observed [4,5].
2. CASE PRESENTATION
AI is a 14-year-old male who presented with cough and noisy breathing of one year duration. There had been a history of snoring at night and stridor. Examination revealed a young male child who had adenoid facies (O-shaped mouth, drooping of eye lids) with apex located at the 4th RIGHT intercostals space mid clavicular line.
A diagnosis of adenoid hypertrophy was made. Chest X-ray showed the heart on the RIGHT side and gastric shadows on the RIGHT. See Figure 1. Abdominal ultrasound showed the spleen on the right side. 2 D echocardiogram showed dextrocardia and liver on the left while ECG also showed dextrocardia. See Figures 2 and 3 and skull X-ray showed shadows and thickening of the nasal and paranasal sinuses. See Figure 4.
A diagnosis of situs inversus totalis with chronic sinusitis and adenoid hypertrophy was made.
Patient however remained asymptomatic.
3. DISCUSSION
This is a first case we have seen since we moved to our new site. In the absence of congenital heart defects, individuals with situs inversus are phenotypically unimpaired, and can lead normal healthy lives, without any complications related to their medical condition [2]. This is akin to our patient who presented only with cough but situs was detected incidentally.
Dextrocardia with situs inversus is a rare condition occurring in about one per 10,000 in the general population. There is no racial predilection for situs inversus and the male-to-female incidence is 1:1. Our patient is a male child, however since this is the first case we saw in recent times, we cannot hazard any sex predilection. This anomaly may not be diagnosed until late in life [5]. In some cases and it is associated with primary ciliary dyskinesia and splenic malformations in some individuals

Figure 1. Note the L mark at the top left corner of the X-ray. The X-ray shows the heart and gastric shadows on the right.
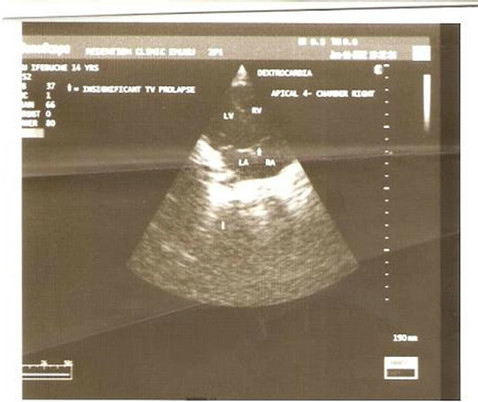
Figure 2. This shows 2 D echocardiogram of our patient; note the dextrocardia. Right heart chambers (right atrium and right ventricles) are in the left position and the left heart chamber (left atrium and left ventricle) are in the right. The liver (Marked L) is in the left.
[5]. This is similar to our case where diagnosis was made at 14 years. We also noted associated chronic sinusitis and adenoid hypertrophy. Since there is no bronchiogram in our institution, we cannot diagnose bronchiochtasis with certainty, thus kertenigiers syndrome was kept in view. Kartagener syndrome is typified by bronchiectasis, sinusitis, and situs inversus and affects 20% of patients with situs inversus; however, only 50% of patients with Kartagener syndrome have situs inversus [6,7].
When situs cannot be determined, it is called situs ambiguous or heterotaxy. In these patients, the liver may be midline, the spleen absent or multiple, the atrial morphology unclear, and the bowel malrotated [8]. This is not what we obtained in our patient.
The arrangements of the position of the abdominal vis-
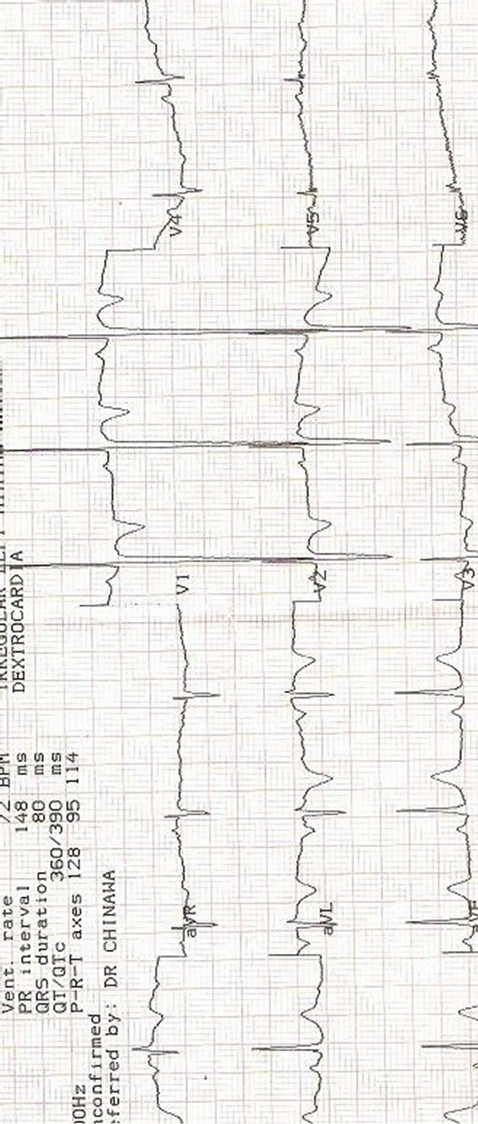
Figure 3. ECG (electrocardiogram) findings of our patient.
cera in dextrocardia may be normal (situs solitus), reversed (situs inversus), and indeterminate (situs ambiguous or isomerism) in 32% - 35%, 35% - 39% and 26% - 28% of cases respectively [8]. Ours was of reverse type.
Situs invertus has been linked with a number of factors including autosomal recessive gene with incomplete penetrance, maternal diabetes, cocaine use and conjoined

Figure 4. CXR of the patient showing soft-tissue opacity along the bony walls of the sinuses may and adenoids (chronic sinusitis and adenoid hypertrophy).
twinning [9,10]. Investigations such as X-rays, abdominal ultrasound, 2-Dechcardiograph, electrocardiogram, magnetic resonant imagery, and computerized axial tomography are all diagnostic tools. X-rays, abdominal ultrasound and 2-D echocardiography were used in this index patient. It is important to detect this anomaly early in patients to enable the clinician make an appropriate diagnosis when the patient presents with other illness.
Imagine a child with left iliac tenderness that had SIT, if undetected, acute appendicitis will be missed!
4. CONCLUSIONS
Situs inversus, though rare, is a condition that demands attention and high index of suspicion , and it is warranted to help the clinician in further management of other illnesses.
5. CONSENT
Informed consent was obtained from the patient for publication of this case.
6. ACKNOWLEDGEMENTS
Our gratitude extends to the care giver and patient who were very cooperative.
Finally we thank the almighty God whose assistance and ideas through the course of this work is priceless.
REFERENCES
- Blegen, H.M. (1949) Surgery in situs inversus. Annals of Surgery, 129, 244-259. doi:10.1097/00000658-194902000-00009
- Budhiraja, S., Singh, G., Miglani, H.P. and Mitra, S.K. (2000) Neonatal intestinal obstruction with isolated levocardia. Journal of Pediatric Surgery, 35, 1115-1116. doi:10.1053/jpsu.2000.7839
- Yokoyama, T., Copeland, N.G., Jenkins, N.A., Montgomery, C.A., Elder, F.F. and Overbeek, P.A. (1993) Reversal of left-right asymmetry: A situs inversus mutation. Science, 260, 679-682. doi:10.1126/science.8480178
- Casey, B. (1998) Two rights make a wrong: Human leftright malformations. Human Molecular Genetics, 7, 1565- 1571. doi:10.1093/hmg/7.10.1565
- Nawaz, H., Matta, M., Hamchou, A., Jacobez, A.H. and Salem, A. (2005) Situs inversus abdominus in association with congenital duodenal obstruction: A report of two cases and review of the literature. Pediatric Surgery International, 21, 589-592. doi:10.1007/s00383-005-1412-y
- Kinney, T.B. and DeLuca, S.A. (1991) Kartagener’s syndrome. American Family Physician, 44, 133-134.
- Ortega, H.A., Vega Nde, A., Santos, B.Q. and Maia, G.T. (2007) Primary ciliary dyskinesia: Considerations regard- ing six cases of Kartagener syndrome. Brazilian Journal of Pulmonology, 33, 602-608. doi:10.1590/S1806-37132007000500017
- Isezuo, S.A., Ma’aji, S.M., Isah, U. and Makusidi, A. (2010) Dextrocardia with situs viscerum inversus totalis in a 65-year-old man: A case report. Nigerian Journal of Clinical Practice, 13, 98-100.
- Agirbashi, M., Hamid, R., Jennings, H.S. and Tiller, G.E. (2000) Situs inversus and hypertrophic cardiomyopathy in identical twins. American Journal of Medical Genetics, 91, 327-330. doi:10.1002/(SICI)1096-8628(20000424)91:5<327::AID-AJMG1>3.0.CO;2-S
- Distefano, G., Romeo, M.G., Grasso, S., Mazonne, D., Sciacca, P. and Mollica, F. (1987) Dextrocardia with and without situs viscerum in 2 siblings. American Journal of Medicine, 27, 929-934.
NOTES
*The authors hereby declare that we have no competing interests.
#Corresponding author.
Authors’ Contributions: JMC contributed in the writing of this paper, he also contributed in all the investigations that the patient went through. Involved in this patient. Eze CU evaluated and worked up the patient.