Paper Menu >>
Journal Menu >>
 Vol.2, No.2, 131-136 (2010) Health doi:10.4236/health.2010.22020 SciRes Copyright © 2010 Openly accessible at http://www.scirp.org/journal/HEALTH/ Acute Myocardial Infarction (AMI) and Intermediate Coronary Syndrome (ICS) E. Stoupel1,2, A. Tamoshiunas3, R. Radishauskas3, G. Bernotiene3, E. Abramson4, J.Sulkes4, P. Israelevich5 1Division of Cardiology, Rabin Medical Center, Petah Tiqwa, Israel 2Sackler Faculty of Medicine, Tel Aviv University, Israel 3Institute of Cardiology, University of Medicine, Kaunas, Lithuania 4 Informatics & Epidemiology Unit Rabin Medical Center, Petah Tiqwa, Israel 5Department of Geophysics & Planetary Sciences, Tel Aviv University, Israel Received 17 November 2009; revised 17 December 2009; accepted 21 December 2009. ABSTRACT In recent studies it was shown that blood co- agulation and inflammation markers are raising at high geomagnetic activity; acute myocardial infarction and all his subtypes, mostly related to atheromatous plaque disruption with higher Cosmic Ray (Neutron) activity. The aim of this study was to explore AMI and ICS differences by concomitant physical conditions, accompany- ing each of these acute coronary syndromes. The data was a part of MONICA international study in Kaunas, Lithuania in years 2000-2005 (72 consecutive months). 4633 patients with AMI (2461 men) and 961 with ICS (654 men), (age up to 65) were studied. For comparison four indices of Solar (SA), three of Geomagnetic (GMA), Cosmic Ray (CRA) measured by Neutron activity imp/min. were used. Cosmophysical data were from space science institutions in the USA and Russia. Pearson correlation coefficients and their probabilities were obtained.Monthly num- ber of AMI and ICS shows different links with the physical parameters: AMI were significantly in- verse related to SA (r=-0.4, p=0.0021) and direct to CRA (Neutron) activity (r=0.23, p=0.048). ICS was not correlated with these two parameters, but show significant links to GMA (r=0.25, p=0.037). Gender differences were evident, men more close related to changes in the mentioned physical parameters.Conclusion: 1. Monthly nu- mber of AMI and ICS is different related to fluc- tuations of environmental physical parameters. 2. The described connections can affect differ- ences in the pathogenesis of these forms of Acute Coronary Insufficiency. Keywords: Acute Myocardial Infarction; Intermediate Coronary Syndrome; Geomagnetic; Cosmic Ray; Neutron Activity 1. INTRODUCTION Acute Coronary Syndrome includes many forms of acute coronary insufficiency. Some related to clinical variants connected to myocardial ischemia-blood supply deficit due to, mostly, atherothrombosis, but also coronary artery spasm, blood losses, vasculitis etc. As a result a number of clinical manifestations of coronary insufficiency take place: pain (Anginal pain), cardiac arrhythmia, resulting in many cases Sudden Cardiac Death, Heart Failure etc. These symptoms can be short, resulting in angina pectoris attacks (AP), and longer and more severe, but remaining without significant myocardial damage named Interme- diate Coronary Syndrome (ICS) The drop of blood supply and provoked oxygen and other vital agents disballance for a longer time (mostly more than 20 minutes) often lead to necrobiosis in the area of the damaged (culprit) artery with a specific additional complex of symp- toms:(clinical, electrocardiographic, enzymatic) and re- sult in later scar formation, or myocardial rupture, life threatening arrhythmias, aneurysm formation, heart fail- ure that is considered as Acute myocardial Infarction (AMI).The ICS takes place between AP and AMI. Recent studied demonstrated significant links between a number of pathogenetic factors involved in ACS development and environmental physical activity [1-9]. The aim of this study was to explore AMI and ICS (code I21-I22 versus I20, ICD 10) by differences in concomitant environ- mental physical conditions: Geomagnetic, Solar and Cosmic Ray (Neutron) activity. 2. PATIENTS AND METHODS 1) 4633 patients with AMI (2461, 53.12% men) age up 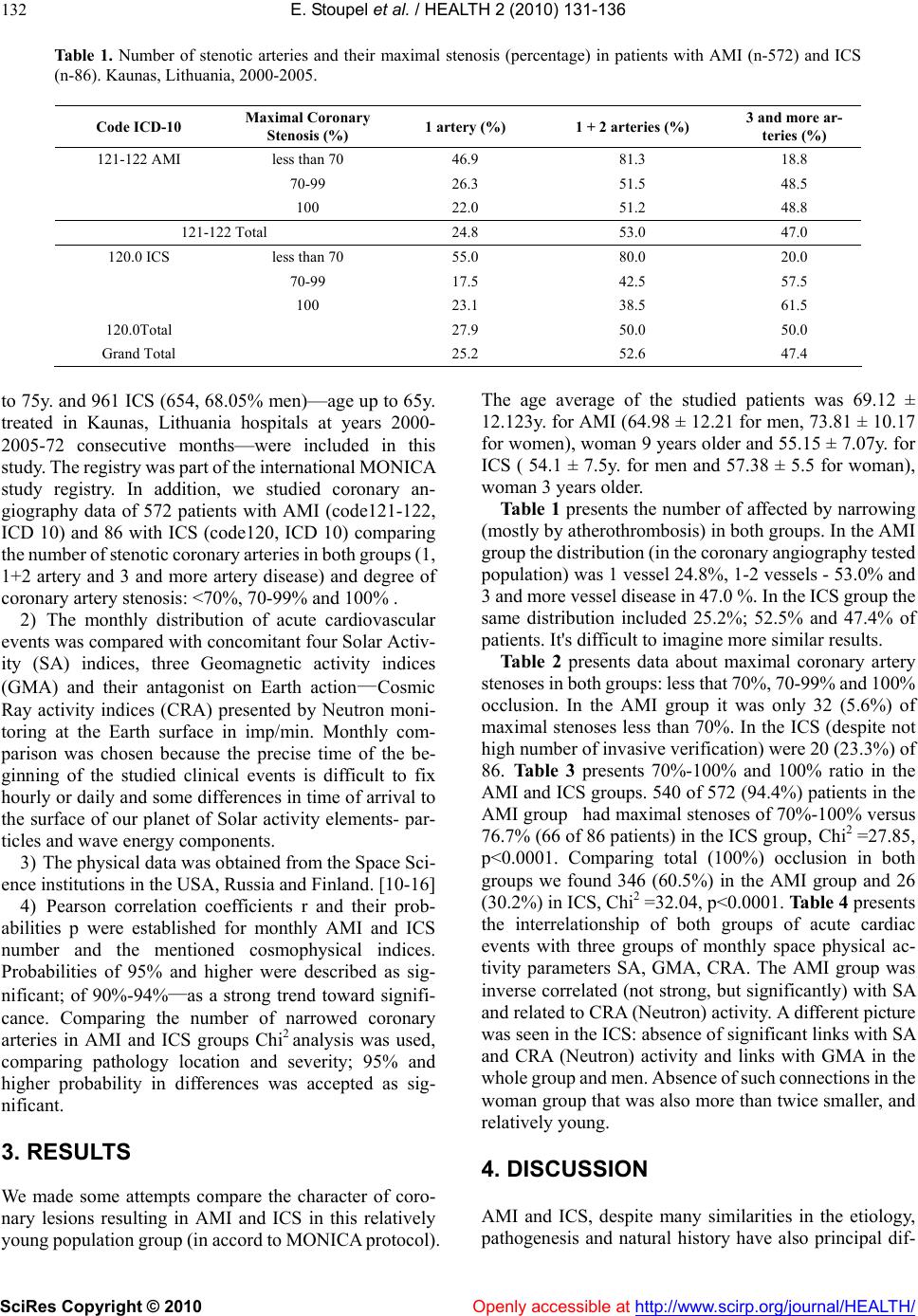 E. Stoupel et al. / HEALTH 2 (2010) 131-136 SciRes Copyright © 2010 Openly accessible at http://www.scirp.org/journal/HEALTH/ 132 Table 1. Number of stenotic arteries and their maximal stenosis (percentage) in patients with AMI (n-572) and ICS (n-86). Kaunas, Lithuania, 2000-2005. Code ICD-10 Maximal Coronary Stenosis (%) 1 artery (%) 1 + 2 arteries (%) 3 and more ar- teries (%) 121-122 AMI less than 70 46.9 81.3 18.8 70-99 26.3 51.5 48.5 100 22.0 51.2 48.8 121-122 Total 24.8 53.0 47.0 120.0 ICS less than 70 55.0 80.0 20.0 70-99 17.5 42.5 57.5 100 23.1 38.5 61.5 120.0Total 27.9 50.0 50.0 Grand Total 25.2 52.6 47.4 to 75y. and 961 ICS (654, 68.05% men)—age up to 65y. treated in Kaunas, Lithuania hospitals at years 2000- 2005-72 consecutive months—were included in this study. The registry was part of the international MONICA study registry. In addition, we studied coronary an- giography data of 572 patients with AMI (code121-122, ICD 10) and 86 with ICS (code120, ICD 10) comparing the number of stenotic coronary arteries in both groups (1, 1+2 artery and 3 and more artery disease) and degree of coronary artery stenosis: <70%, 70-99% and 100% . 2) The monthly distribution of acute cardiovascular events was compared with concomitant four Solar Activ- ity (SA) indices, three Geomagnetic activity indices (GMA) and their antagonist on Earth action—Cosmic Ray activity indices (CRA) presented by Neutron moni- toring at the Earth surface in imp/min. Monthly com- parison was chosen because the precise time of the be- ginning of the studied clinical events is difficult to fix hourly or daily and some differences in time of arrival to the surface of our planet of Solar activity elements- par- ticles and wave energy components. 3) The physical data was obtained from the Space Sci- ence institutions in the USA, Russia and Finland. [10-16] 4) Pearson correlation coefficients r and their prob- abilities p were established for monthly AMI and ICS number and the mentioned cosmophysical indices. Probabilities of 95% and higher were described as sig- nificant; of 90%-94%—as a strong trend toward signifi- cance. Comparing the number of narrowed coronary arteries in AMI and ICS groups Chi2 analysis was used, comparing pathology location and severity; 95% and higher probability in differences was accepted as sig- nificant. 3. RESULTS We made some attempts compare the character of coro- nary lesions resulting in AMI and ICS in this relatively young population group (in accord to MONICA protocol). The age average of the studied patients was 69.12 ± 12.123y. for AMI (64.98 ± 12.21 for men, 73.81 ± 10.17 for women), woman 9 years older and 55.15 ± 7.07y. for ICS ( 54.1 ± 7.5y. for men and 57.38 ± 5.5 for woman), woman 3 years older. Table 1 presents the number of affected by narrowing (mostly by atherothrombosis) in both groups. In the AMI group the distribution (in the coronary angiography tested population) was 1 vessel 24.8%, 1-2 vessels - 53.0% and 3 and more vessel disease in 47.0 %. In the ICS group the same distribution included 25.2%; 52.5% and 47.4% of patients. It's difficult to imagine more similar results. Table 2 presents data about maximal coronary artery stenoses in both groups: less that 70%, 70-99% and 100% occlusion. In the AMI group it was only 32 (5.6%) of maximal stenoses less than 70%. In the ICS (despite not high number of invasive verification) were 20 (23.3%) of 86. Table 3 presents 70%-100% and 100% ratio in the AMI and ICS groups. 540 of 572 (94.4%) patients in the AMI group had maximal stenoses of 70%-100% versus 76.7% (66 of 86 patients) in the ICS group, Chi2 =27.85, p<0.0001. Comparing total (100%) occlusion in both groups we found 346 (60.5%) in the AMI group and 26 (30.2%) in ICS, Chi2 =32.04, p<0.0001. Table 4 presents the interrelationship of both groups of acute cardiac events with three groups of monthly space physical ac- tivity parameters SA, GMA, CRA. The AMI group was inverse correlated (not strong, but significantly) with SA and related to CRA (Neutron) activity. A different picture was seen in the ICS: absence of significant links with SA and CRA (Neutron) activity and links with GMA in the whole group and men. Absence of such connections in the woman group that was also more than twice smaller, and relatively young. 4. DISCUSSION AMI and ICS, despite many similarities in the etiology, pathogenesis and natural history have also principal dif- 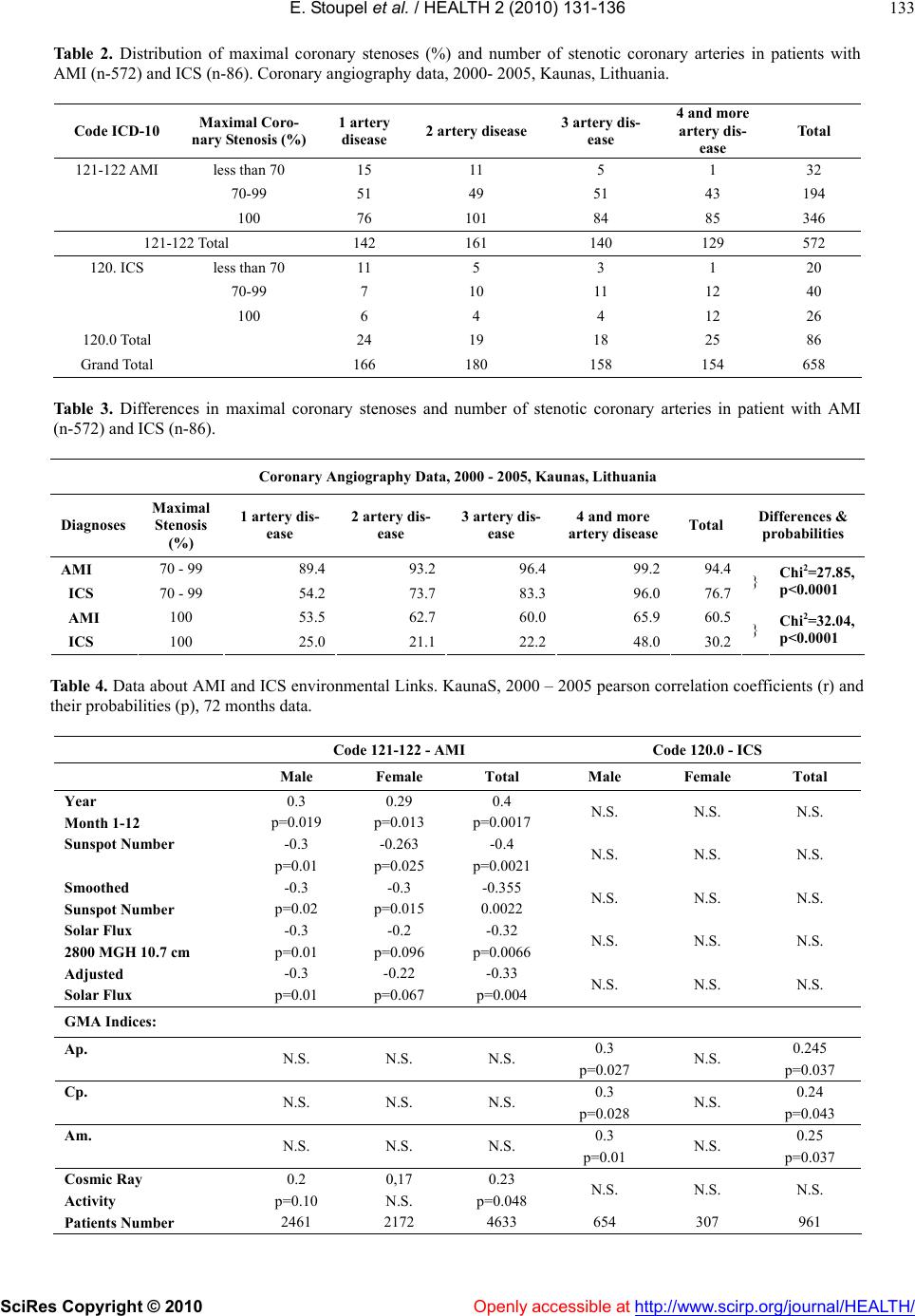 E. Stoupel et al. / HEALTH 2 (2010) 131-136 SciRes Copyright © 2010 Openly accessible at http://www.scirp.org/journal/HEALTH/ 133 Table 2. Distribution of maximal coronary stenoses (%) and number of stenotic coronary arteries in patients with AMI (n-572) and ICS (n-86). Coronary angiography data, 2000- 2005, Kaunas, Lithuania. Code ICD-10 Maximal Coro- nary Stenosis (%) 1 artery disease 2 artery disease 3 artery dis- ease 4 and more artery dis- ease Total 121-122 AMI less than 70 15 11 5 1 32 70-99 51 49 51 43 194 100 76 101 84 85 346 121-122 Total 142 161 140 129 572 120. ICS less than 70 11 5 3 1 20 70-99 7 10 11 12 40 100 6 4 4 12 26 120.0 Total 24 19 18 25 86 Grand Total 166 180 158 154 658 Table 3. Differences in maximal coronary stenoses and number of stenotic coronary arteries in patient with AMI (n-572) and ICS (n-86). Coronary Angiography Data, 2000 - 2005, Kaunas, Lithuania Diagnoses Maximal Stenosis (%) 1 artery dis- ease 2 artery dis- ease 3 artery dis- ease 4 and more artery disease Total Differences & probabilities AMI 70 - 99 89.4 93.2 96.4 99.2 94.4 ICS 70 - 99 54.2 73.7 83.3 96.0 76.7 } Chi2=27.85, p<0.0001 AMI 100 53.5 62.7 60.0 65.9 60.5 ICS 100 25.0 21.1 22.2 48.0 30.2 } Chi2=32.04, p<0.0001 Table 4. Data about AMI and ICS environmental Links. KaunaS, 2000 – 2005 pearson correlation coefficients (r) and their probabilities (p), 72 months data. Code 121-122 - AMI Code 120.0 - ICS Male Female Total Male Female Total Year 0.3 0.29 0.4 Month 1-12 p=0.019 p=0.013 p=0.0017 N.S. N.S. N.S. Sunspot Number -0.3 -0.263 -0.4 p=0.01 p=0.025 p=0.0021 N.S. N.S. N.S. Smoothed -0.3 -0.3 -0.355 Sunspot Number p=0.02 p=0.015 0.0022 N.S. N.S. N.S. Solar Flux -0.3 -0.2 -0.32 2800 MGH 10.7 cm p=0.01 p=0.096 p=0.0066 N.S. N.S. N.S. Adjusted -0.3 -0.22 -0.33 Solar Flux p=0.01 p=0.067 p=0.004 N.S. N.S. N.S. GMA Indices: Ap. 0.3 0.245 N.S. N.S. N.S. p=0.027 N.S. p=0.037 Cp. 0.3 0.24 N.S. N.S. N.S. p=0.028 N.S. p=0.043 Am. 0.3 0.25 N.S. N.S. N.S. p=0.01 N.S. p=0.037 Cosmic Ray 0.2 0,17 0.23 Activity p=0.10 N.S. p=0.048 N.S. N.S. N.S. Patients Number 2461 2172 4633 654 307 961 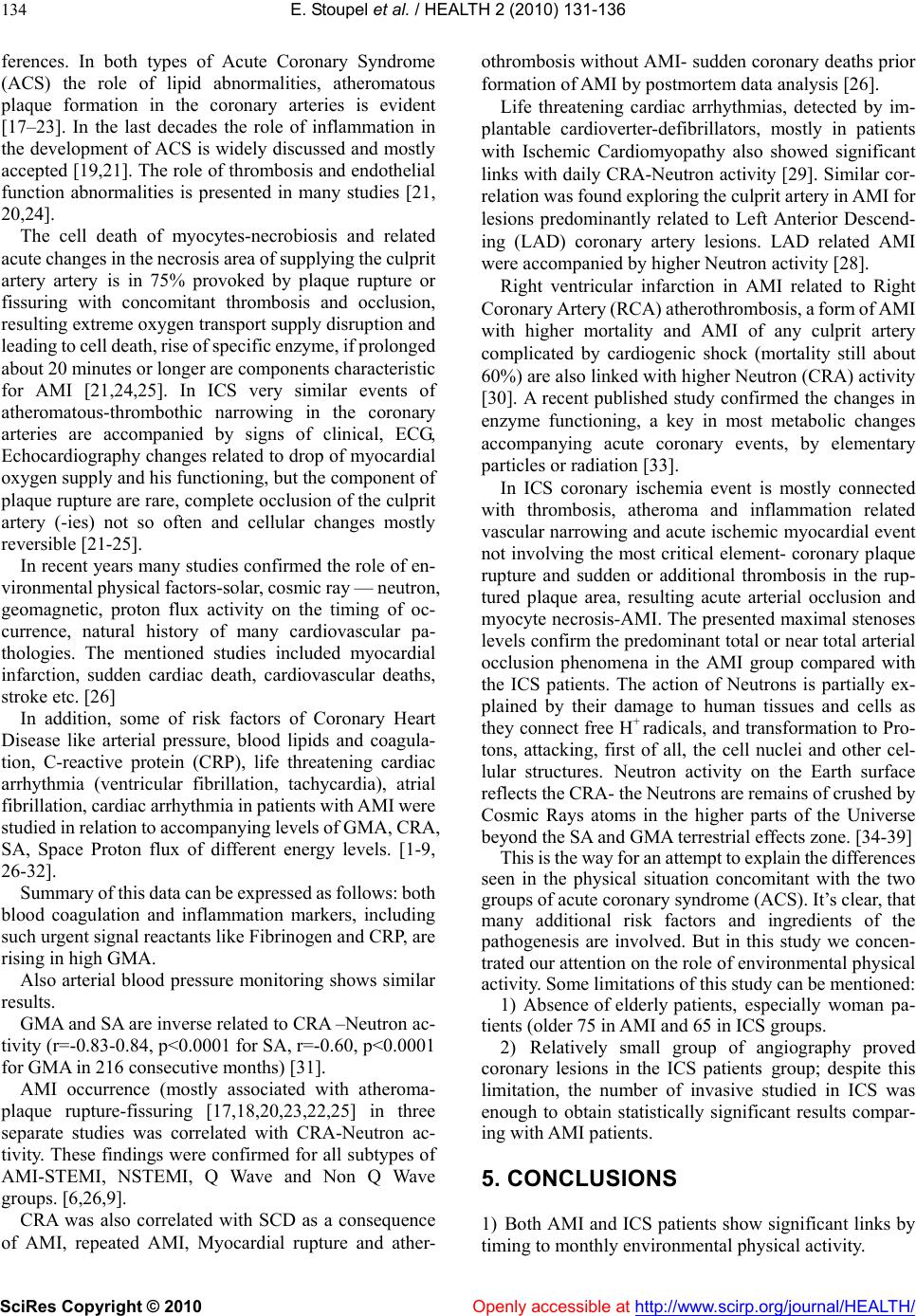 E. Stoupel et al. / HEALTH 2 (2010) 131-136 SciRes Copyright © 2010 Openly accessible at http://www.scirp.org/journal/HEALTH/ 134 ferences. In both types of Acute Coronary Syndrome (ACS) the role of lipid abnormalities, atheromatous plaque formation in the coronary arteries is evident [17–23]. In the last decades the role of inflammation in the development of ACS is widely discussed and mostly accepted [19,21]. The role of thrombosis and endothelial function abnormalities is presented in many studies [21, 20,24]. The cell death of myocytes-necrobiosis and related acute changes in the necrosis area of supplying the culprit artery artery is in 75% provoked by plaque rupture or fissuring with concomitant thrombosis and occlusion, resulting extreme oxygen transport supply disruption and leading to cell death, rise of specific enzyme, if prolonged about 20 minutes or longer are components characteristic for AMI [21,24,25]. In ICS very similar events of atheromatous-thrombothic narrowing in the coronary arteries are accompanied by signs of clinical, ECG, Echocardiography changes related to drop of myocardial oxygen supply and his functioning, but the component of plaque rupture are rare, complete occlusion of the culprit artery (-ies) not so often and cellular changes mostly reversible [21-25]. In recent years many studies confirmed the role of en- vironmental physical factors-solar, cosmic ray — neutron, geomagnetic, proton flux activity on the timing of oc- currence, natural history of many cardiovascular pa- thologies. The mentioned studies included myocardial infarction, sudden cardiac death, cardiovascular deaths, stroke etc. [26] In addition, some of risk factors of Coronary Heart Disease like arterial pressure, blood lipids and coagula- tion, C-reactive protein (CRP), life threatening cardiac arrhythmia (ventricular fibrillation, tachycardia), atrial fibrillation, cardiac arrhythmia in patients with AMI were studied in relation to accompanying levels of GMA, CRA, SA, Space Proton flux of different energy levels. [1-9, 26-32]. Summary of this data can be expressed as follows: both blood coagulation and inflammation markers, including such urgent signal reactants like Fibrinogen and CRP, are rising in high GMA. Also arterial blood pressure monitoring shows similar results. GMA and SA are inverse related to CRA –Neutron ac- tivity (r=-0.83-0.84, p<0.0001 for SA, r=-0.60, p<0.0001 for GMA in 216 consecutive months) [31]. AMI occurrence (mostly associated with atheroma- plaque rupture-fissuring [17,18,20,23,22,25] in three separate studies was correlated with CRA-Neutron ac- tivity. These findings were confirmed for all subtypes of AMI-STEMI, NSTEMI, Q Wave and Non Q Wave groups. [6,26,9]. CRA was also correlated with SCD as a consequence of AMI, repeated AMI, Myocardial rupture and ather- othrombosis without AMI- sudden coronary deaths prior formation of AMI by postmortem data analysis [26]. Life threatening cardiac arrhythmias, detected by im- plantable cardioverter-defibrillators, mostly in patients with Ischemic Cardiomyopathy also showed significant links with daily CRA-Neutron activity [29]. Similar cor- relation was found exploring the culprit artery in AMI for lesions predominantly related to Left Anterior Descend- ing (LAD) coronary artery lesions. LAD related AMI were accompanied by higher Neutron activity [28]. Right ventricular infarction in AMI related to Right Coronary Artery (RCA) atherothrombosis, a form of AMI with higher mortality and AMI of any culprit artery complicated by cardiogenic shock (mortality still about 60%) are also linked with higher Neutron (CRA) activity [30]. A recent published study confirmed the changes in enzyme functioning, a key in most metabolic changes accompanying acute coronary events, by elementary particles or radiation [33]. In ICS coronary ischemia event is mostly connected with thrombosis, atheroma and inflammation related vascular narrowing and acute ischemic myocardial event not involving the most critical element- coronary plaque rupture and sudden or additional thrombosis in the rup- tured plaque area, resulting acute arterial occlusion and myocyte necrosis-AMI. The presented maximal stenoses levels confirm the predominant total or near total arterial occlusion phenomena in the AMI group compared with the ICS patients. The action of Neutrons is partially ex- plained by their damage to human tissues and cells as they connect free H+ radicals, and transformation to Pro- tons, attacking, first of all, the cell nuclei and other cel- lular structures. Neutron activity on the Earth surface reflects the CRA- the Neutrons are remains of crushed by Cosmic Rays atoms in the higher parts of the Universe beyond the SA and GMA terrestrial effects zone. [34-39] This is the way for an attempt to explain the differences seen in the physical situation concomitant with the two groups of acute coronary syndrome (ACS). It’s clear, that many additional risk factors and ingredients of the pathogenesis are involved. But in this study we concen- trated our attention on the role of environmental physical activity. Some limitations of this study can be mentioned: 1) Absence of elderly patients, especially woman pa- tients (older 75 in AMI and 65 in ICS groups. 2) Relatively small group of angiography proved coronary lesions in the ICS patients group; despite this limitation, the number of invasive studied in ICS was enough to obtain statistically significant results compar- ing with AMI patients. 5. CONCLUSIONS 1) Both AMI and ICS patients show significant links by timing to monthly environmental physical activity.  E. Stoupel et al. / HEALTH 2 (2010) 131-136 SciRes Copyright © 2010 Openly accessible at http://www.scirp.org/journal/HEALTH/ 135 2) ICS patients show correlation with level of GMA. Patients with AMI - with CRA. 3) These differences can be a result to diminished role of plaque disruption and / or fissuring in ICS compared to AMI. 4) Both groups were similar by number of affected coronary arteries, but AMI patients suffered from more critical and total coronary occlusions. 6. ACKNOWLEDGEMENTS The authors express gratitude to Mr. G.H. Jenkins for his help with the English version of the manuscript. We are very grateful for the fi- nancial support from Junta de Castilla y León (JCYL). REFERENCES [1] Stoupel, E., Joshua, H., Lahav, J. (1996) Human blood coagulation parameters and geomagnetic activity. Eur J Int Med, 7, 217-220. [2] Stoupel, E., Wittenberg, C., Zabludovski, J., Boner, G. (1995) Ambulatory blood pressure monitoring in patients with hypertension on days of high and low geomagnetic activity. J Human Hypertension, 9, 293-294. [3] Stoupel, E., Abramson, E., Israelevich, P., Sulkes, J., Harell, D. (2007) Dynamics of serum C-reactive protein (CRP) level and cosmophysical activity. Eur J Int Med, 18(2), 124-128. [4] Stoupel, E. (1980) Solar-terrestrial predictions: Aspects for preventive medicine in: Donnelly Ed. solar-terrestrial predictions. Vol 4. NOAA Space Environment Laboratory and USAF, Boulder, Co., USA, G29-G40. [5] Oranevskii, V.N., Breus, T.K., Baevskii, R.M., Rappoprt, S.I., Petrov, V.M., Barsukova, Z.V. (1998) Effect of geo- magnetic activity on the functional status of the body. Biofizika, 43(5), 819-826. [6] Stoupel, E., Domarkiene, S., Radishauskas, R., Bernotiene, G., Abramson, E., Israelevich, P., Sulkes, J. (2004) Links between monthly rates of four subtypes of acute myocar- dial infarction and their corresponding cosmophysical activity parameters. J Basic & Clin Physiol & Pharmacol, 15(3-4), 175-184. [7] Gurfinkel, Y.I., Liubimov, V.V., Orajevskii, V.N., Par- fenova, L.M., Yurjev, A.S. (1995) The influence of geo- magnetic activity on capillary flow in ischemic heart disease patients. Biofizika, 40(4), 793-799. [8] Nuzhdina, M.A. (1998) Effect of natural factors on the occurrence of cardiovascular diseases. Biofizika, 43(4) 640-646. [9] Stoupel, E., Babayev, E., Mustafa, F., Abramson, E., Israelevich, P., Sulkes, J. (2007) Acute myocardial In- farction occurrence: Environmental links - Baku 2003-2005 data. Med Sc Monit, 13(8), BR 175-179. [10] NOAA National Geophysical Data Center. Solar Indices Bulletin. [11] NOAA National Geophysical Data Center. Geomagnetic Indices Bulletin. [12] NOAA, SWPC –USAF Preliminary Report and Forecast of Solar Geophysical Data. [13] Russian Academy of Sciences. Izmiran Institute. Cosmic Data. [14] Russian Academy of Sciences. Moscow Neutron Moni- toring Data. [15] Oulu University. Neutron Monitoring Data, 15. [16] NOAA-USAF. (1988) SESC glossary of solar–terrestrial terms. Boulder, CO, USA, 1-69. [17] Fuster, V. (1999) The vulnerable atherosclerotic plaque. Blackwell Publishing. [18] Fuster, V., Fayad, Z.A., Badimon, J.J. (1999) Acute coro- nary syndromes. Lancet 353, Suppl., 2, S114-119. [19] Libby, P., Ridker, P.M., Maseri, A. (2002) Inflammation and atherosclerosis. Circulation, 105(9), 1135-1143. [20] Topol, E. (2005) Atlas of Atherothrombosis. Current Medical Group. 2004 London. [21] Gawaz, M. (2006) The evolving science of atherothrom- botic disease Eur heart J Suppl. Antiplateled Strategies in Patients Undergoing Interventions with Acute Coronary Syndrome Ed. J.-F. Neumann, 10(1), 14-17. [22] Solem, J., Levin, M., Karlsson, T., Grip, L., Albertson, P., Wiklund, O. (2006) Composition of coronary plaque ob- tained by directional atherectomy in stable angina: its re- lation to serum lipids and statin treatment. J Int Med, 259 (3), 267-275. [23] Tanaka, A., Shimada, K., Numba, M., Sakamoto, T., Na- kamura, Y., Nishida, V.Y., Yoshikawa, J., Akasaka, T.M., Relationship between longitudinal. [24] (2008) Morphology of ruptured plaques and TIMI flow grade in acute coronary syndrome: a three-dimensional intravascular ultrasound imaging study. Eur Heart J, 29, 38-44. [25] De Catherina, R., Husted, S., Walentin, L. et al. (2007) ESC position paper v. Anticoagulants in heart disease: current status and perspectives. Eur Heart J, 28(7), 880-913. [26] Thigesen, K., Alpert, J.S. (2007) White HD on behalf the ESC/ACCF/AHA/ WHF task force universal definition of myocardial infarction. European Heart Journal, 28, 2525-2538. [27] Stoupel, E. (2002) The effect of geomagnetic activity on cardiovascular parameters. Biomedicine & Pharmaco- therapy. 56, 247-256. [28] Stoupel, E., Domarkiene, S., Radishauskas, R., Abramson, E., Israelevich, P., Sulkes, J. (2006) Neutrons and Sudden Cardiac Deaths (SCD) Codes 121-125 ICD 10. Basic & Clin Physiol & Pharmacol, 17(1), 45-53. [29] Stoupel, E., Assali, A., Teplitzky, I., Abramson, E., Is- raelevich, P., Sulkes, J. (2008) The culprit artery in acute myocardial infarction in different environmental physical activity levels. Intern J Cardiol, 126, 266-290. [30] Stoupel, E., Kusniec, J., Mazur, J., Abramson, E., Is- raelevich, P., Strasberg, B. (2008) Timing of life-threat- ening arrhythmias detected by implantable cardioverter- defibrillators in relation to changes in cosmophysical factors. Cardiology J, 15(5), 1-4. [31] Stoupel, E., Assali, A., Teplitzky, I., Vaknin-Assa, H., Abramson, E., Israelevich, P., Kornowski, R. (2009) Physical influences on right ventricular infarction and cardiogenic shock in acute myocardial Infarction. Basic & 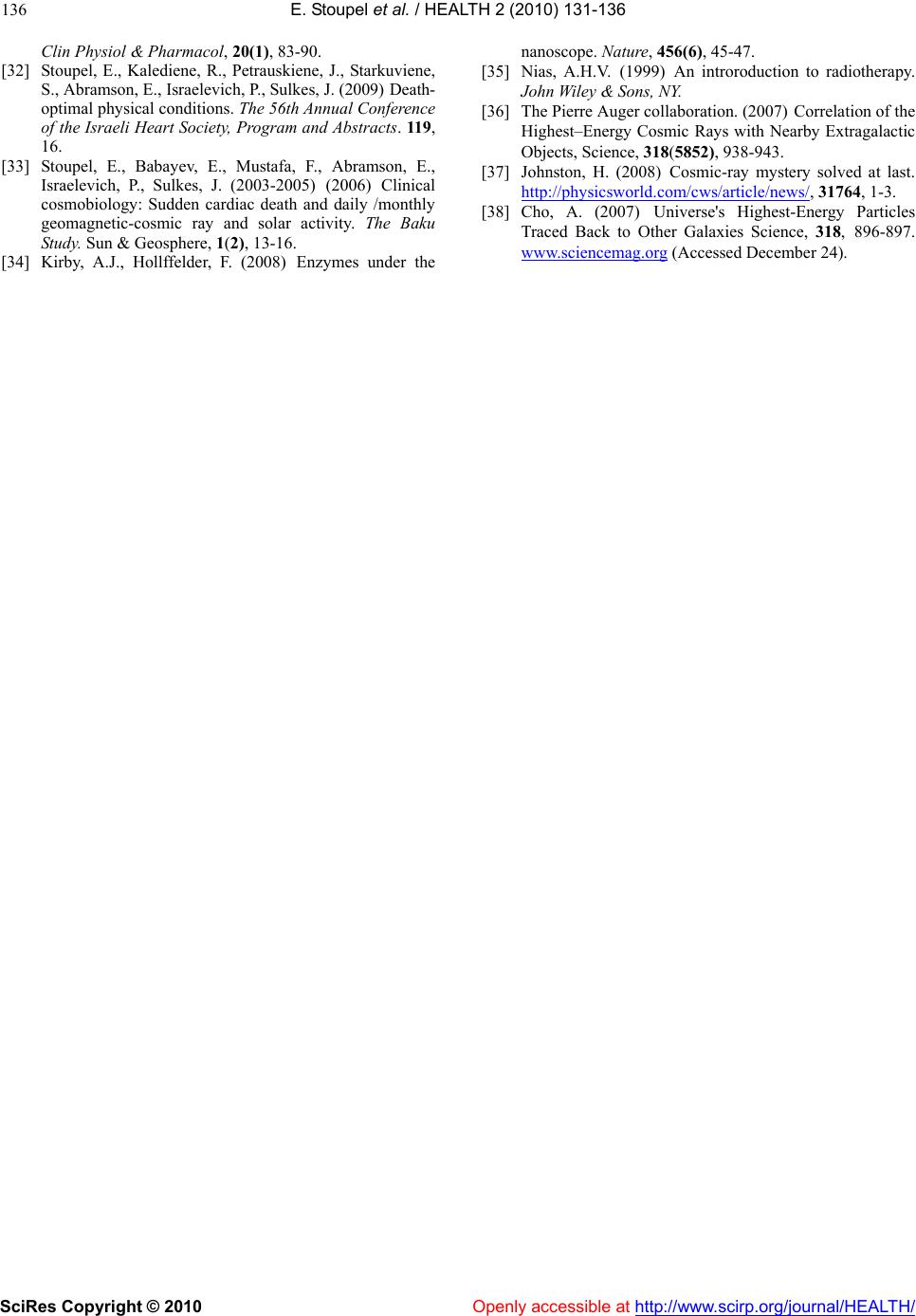 E. Stoupel et al. / HEALTH 2 (2010) 131-136 SciRes Copyright © 2010 Openly accessible at http://www.scirp.org/journal/HEALTH/ 136 Clin Physiol & Pharmacol, 20(1), 83-90. [32] Stoupel, E., Kalediene, R., Petrauskiene, J., Starkuviene, S., Abramson, E., Israelevich, P., Sulkes, J. (2009) Death- optimal physical conditions. The 56th Annual Conference of the Israeli Heart Society, Program and Abstracts. 119, 16. [33] Stoupel, E., Babayev, E., Mustafa, F., Abramson, E., Israelevich, P., Sulkes, J. (2003-2005) (2006) Clinical cosmobiology: Sudden cardiac death and daily /monthly geomagnetic-cosmic ray and solar activity. The Baku Study. Sun & Geosphere, 1(2), 13-16. [34] Kirby, A.J., Hollffelder, F. (2008) Enzymes under the nanoscope. Nature, 456(6), 45-47. [35] Nias, A.H.V. (1999) An introroduction to radiotherapy. John Wiley & Sons, NY. [36] The Pierre Auger collaboration. (2007) Correlation of the Highest–Energy Cosmic Rays with Nearby Extragalactic Objects, Science, 318(5852), 938-943. [37] Johnston, H. (2008) Cosmic-ray mystery solved at last. http://physicsworld.com/cws/article/news/, 31764, 1-3. [38] Cho, A. (2007) Universe's Highest-Energy Particles Traced Back to Other Galaxies Science, 318, 896-897. www.sciencemag.org (Accessed December 24). |