Health
Vol.4 No.10A(2012), Article ID:24267,4 pages DOI:10.4236/health.2012.430152
Knowledge and preventive measures practiced by junior high school students from Mexico City regarding influenza A (H1N1)
![]()
1Departamento de Salud Pública, Facultad de Medicina, Universidad Nacional Autónoma de México, México City, México
2Dirección de Enseñanza, Hospital General “Dr. Manuel Gea González” Secretaría de Salud, México City, México
3Departamento de Biología, Facultad de Ciencias, Universidad Nacional Autónoma de México, México City, México
4Dirección General de Innovación y Fortalecimiento Académico, Administración Federal de Servicios Educativos en el Distrito Federal, Secretaría de Educación Pública, México City, México
5Departamento de Microbiología y Parasitología, Facultad de Medicina, Universidad Nacional Autónoma de México, México City, México; *Corresponding Author: flisser@unam.mx
Received 18 September 2012; revised 16 October 2012; accepted 18 October 2012
Keywords: Alcohol Gel; Epidemiologic Survey; Hand Washing; Health Behavior; Influenza A (H1N1) Outbreak; Mexico City
ABSTRACT
Background: Influenza A (H1N1) is the most recent pandemic disease that has affected the human population. Objective: To evaluate knowledge and preventive measures related with this disease one year after the epidemic of Mexicothat took place in 2009. Material and methods: An epidemiologic survey regarding influenza A (H1N1) was conducted in June 2010 among 2541 students from the second grade of all public high schools in a borough in Mexico City. The questionnaire included items on the knowledge of the disease and practice of preventive measures. Results: Most students obtained the information from television, half of them from parents and only one fifth from teachers; 72% of the participants had a favorable knowledge about the disease and the measures to avoid being infected. However, only 37% practiced such preventive measures. Conclusion: Knowledge has a positive influence on practices towards health. Parents and teachers have an important role in health education, thus efforts should be directed to involve them more intensely in health education.
1. INTRODUCTION
Influenza is caused by a virus of the Orthomyxoviridae family and is classified in three types A, B and C. It is spherical and measures around 100 nm; the most important components from the immunological point of view are two glycoproteins: hemagglutinin and neuraminidase, contained in the lipid capsule, which induce innate and adaptive immune responses in the respiratory tract mucosa. The virus causes influenza; an acute respiratory disease that damages the respiratory epithelium due mainly to viral replication, cytolysis and apoptosis; in some cases it can cause severe pneumonia. The virus is transmitted among people; it equally affects men and women of any age. However, severe infection from influenza typically occurs in elders and in very young individuals [1].
In April 2009, a novel strain of influenza A (H1N1) virus unexpectedly appeared as a pandemic outbreak, affecting young adults, as compared to seasonal influenza, and the Mexican Ministry of Health established prevention and control measures to reduce the risk of infection in all the country, including Mexico City [2-4]. Media provided information about the name of the virus, preventive measures such as washing hands with water and soap, using alcohol gel to clean hands, coughing and sneezing on the inner part of the elbow or by covering nose and mouth with a napkin (which was to be disposed afterwards in the waste basket), use of facemasks, greeting with out hand shakes, not kissing and avoiding gatherings. Healthy people were to prevent contact with patients having respiratory diseases, no sharing of glassware or food with them and following clinician recommendations if becoming sick. Importantly, main symptoms included sudden high fever, coughing and headache, general malaise or nasal congestion, and death could occur [5,6].
Many studies have been recently published (referred in the discussion) related to questions answered by adults (18 years or older) about knowledge and practices related to influenza, none included younger persons; thus, the purpose of the present study was to identify and describe what junior high school students, in a borough in Mexico City know and what are their practices preventing influenza, one year after the outbreak. Associations between knowledge and practices were also evaluated.
2. METHODS
2.1. Design and Sample Selection
A cross-sectional epidemiological study was performed after approval by the Ministry of Public Education authorities in June 2010 to all students (3200) attending all (20) day-time public junior high schools in the Miguel Hidalgo borough (Figure 1). Authorities in each school were visited in order to explain the project and convene an adequate time to administer the questionnaire without interfering with classes. Students in each second grade (out of three) group received a detailed explanation of the objective and logistics for anonymously answering the questionnaire, after which declared informed consent was required.
2.2. Data Collection
An epidemiological questionnaire was developed and was validated in a group of students from the first year of the medical course, was given to junior high school students, who answered anonymously. The questionnaire inquired about type of mass media (television [TV], radio, newspaper or internet) from which the students obtained

Figure 1. Location of the Miguel Hidalgo borough (gray) in an insert of the Federal District of Mexico City in a map of Mexico.
information about influenza A (H1N1) and with whom they talked about this subject (teachers, parents). The evaluation questionnaire included 28 questions related to knowledge and 12 to preventive practices. Knowledge included: type of microorganism, disease, symptoms and cure, lethality, transmission, distribution, prevention, who could become sick, and the difference with seasonal flu. Practices included: if hands were washed daily with soap and how frequent, use of alcohol gel, technique for sneezing and coughing, greeting with a handshake or with a kiss, how to avoid infection, and what to do if one becomes sick. All responses used tick boxes.
One point was given to each correct answer. Taking in account that in Mexico 6 or more answers, in a scale of 1 to 10, are needed to approve a student in any given exam, at least 17 of the 28 questions needed to have correct answers to be favorable for knowledge and at least 7 of 12 for preventive practices. Responses we reported as the average of all questions on knowledge and on practices.
2.3. Ethical Approval
This study was approved by of authorities of the Ministry of Public Education.
2.4. Analysis
Data were entered in a spreadsheet and analyzed using the SPSS software version for Windows 17 (Inc., Chicago, IL) and Epi-Info 6.04 (CDC, Atlanta, Ga, USA). The magnitude of associations between independent variables (gender, communication, information) and dependent variables (knowledge and preventive practices), was analyzed by bivariate Odds Ratio (OR), 95% confidence interval (IC95%) and chi square test. Pearson correlation test was used to compare students’ knowledge and what do they practice. Statistical significance was considered as p < 0.05.
3. RESULTS
From the 3206 students registered in the 2009-2010 school year in the 20 junior high schools in Miguel Hidalgo borough, 2541 (79%)—considered as good response rate—answered the questionnaire; the remaining 665 were absent on the specific day of the questionnaire or did not attend school anymore. Gender was equally represented and average age was 13.7 ± 0.6 years. Ninety percent of the students knew about the pandemic influenza through messages and commercials on TV; communication regarding the disease was 52% with the parents, 19% with the teachers and 17% did not talk about this matter. Table 1 shows the knowledge of the students and Table 2 the preventive practices, which were 72% and 37% favorable, respectively. However, 24% of students stated that influenza A (H1N1) was a governmental hoax to distract the attention of the inhabitants. The re-

Table 1. Knowledge related with influenza A (H1N1) of junior high school students in the Miguel Hidalgo borough, Mexico City, 2010.
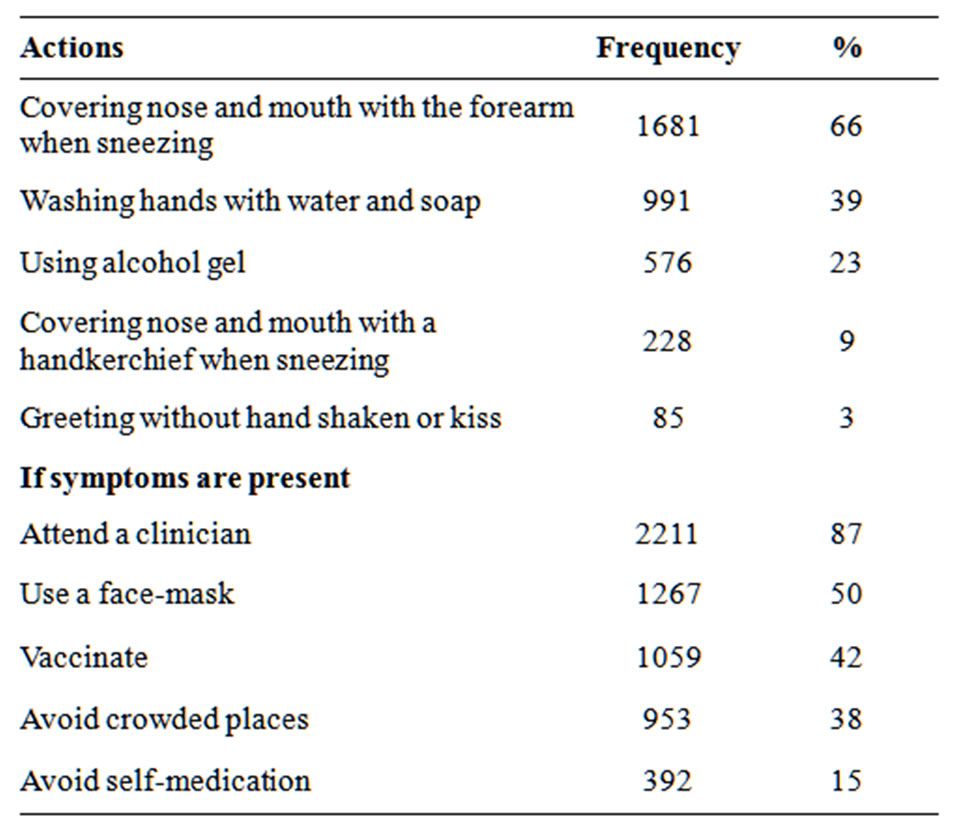
Table 2. Preventive measures against influenza A (H1N1) practiced by junior high school students in the Miguel Hidalgo borough, Mexico City, 2010.
sults of the bivariate analysis (Table 3) showed no association of gender with knowledge or with preventive behaviors. In contrast, information through TV and communication with parents and teachers were significantly associated to knowledge and to practices. Pearson correlation test showed that students assimilated the information they received but there was no correlation between knowledge and practices (r = 0.33; p < 0.0001).
4. DISCUSSION
After the influenza A (H1N1) pandemic in Mexico in the spring of 2009 [2-4], the Mexican government transmitted information through mass media so that people could learn about the disease, how to avoid it, and what to do if they became sick. We considered important to find out one year later the knowledge acquired by adolescents, because no data are available in the literature, and also because in 2009, 29% of this age group (<15 years) were laboratory confirmed cases with 7% mortality [4]. Second grade junior high school students were selected because, being in the second grade, they are adolescents already adapted to a more advanced type of learning, as compared to elementary school and to first graders. Daytime students were chosen in order to have a narrow age distribution since in evening groups, young adults also attend. The Miguel Hidalgo borough was selected because it includes different socio-economic level inhabitants. Interestingly 72% (1753) of the students answered correctly 17 or more of the 28 questions related to knowledge, indicating that they retained adequate information, but self-reported preventive measures were only 37% favorable. It was quite satisfying to find out that half of the students communicated with their parents regarding influenza. Like parents, teachers also had a favorable communication with students although in a lower frequency. Our data suggest that teachers are important in the transmission of health information and provide a window of opportunity for health education to improve personal hygiene; thus education authorities in Mexico should take more advantage of this fact.
Important misconceptions were that 24% of the students indicated that influenza A (H1N1) was faked by the government, 58% would not accept vaccination and 85% would use self-medication if symptoms were present. In other international studies, 38% Saudi adults interviewed in shopping malls were not convinced that reports about the disease given by the Ministry of Health were true [7] and 45% surveyed Indians believed that health care authorities were exaggerating the risk of a pandemic [8]. The fact that the values reported by Mexico were lower could be related to the age of the respondents (adolescents in this case as opposed to adults the other two surveys). Regarding vaccination, 44% of British adults [9] and 68% of Italian nurses [10] would not accept vaccina-

Table 3. Association analysis of variables (knowledge and practice) influenza A (H1N1) obtained by junior high school students in the Miguel Hidalgo borough, Mexico City, 2010.
tion; the latter value is worrisome for it suggests a lack of confidence by health personnel to be vaccinated. Selfmedication (provided mainly by mothers or pharmacists) is common in Mexico; to control it, a new law prohibits selling antibiotics over the counter without a medical recipe since 2010 [11]. Because of the identified misconceptions, authorities should take into consideration the amount and diversity of information provided (including that of mass media) in order to avoid wrong interpretations and distrust.
Seemingly, knowledge is not enough to change practices: self-reported preventive measures were only 37% favorable. Many students knew of the importance of washing hands with soap or with alcohol gel, nonetheless only 39% or 23% said they use these measures respectively. Washing hands with water and soap is a measure that has been endorsed since the last cholera pandemic in Mexico in 1991 [12] while using alcohol gel was recently promoted with the influenza pandemic in 2009. Interestingly the knowledge of the importance of washing hands during the recent pandemic outbreak was close to half of the individuals inquired, independently from the age or the country where the study was performed: in junior high school students (the present study), 39% indicated washing their hands with water and soap 1 to 6 times a day, 47% of adults interviewed by telephone in Hong Kong, China, reported currently washing their hands more than 10 times a day [13], 50% of adults in shopping malls in Sydney, Australia [14] and 55% in Rajasthan, India washed their hands with soap and water more often than usual [8] as well as 57% of students from the University of Korea [15]. As expected, the response was higher among Italian health workers, since 80% of nurses and 65% of physicians indicated, through a website questionnaire, that they washed their hands or used a sanitizer more frequently [10]. Lau et al. consider that the frequency of hand washing can be further increased by informing citizens about the relationship between hand washing and prevention of emerging respiretory infectious diseases, based on previous evidences from SARS and avian flu epidemics [13]. Since less than half of junior high school surveyed students indicated washing hands sufficiently per day, it would be important to investigate the real availability of soap or of fresh water in schools and at home for this purpose.
Alcohol gel has been involved in a recent controversy in the USA regarding its efficacy against influenza A (H1N1) [16]. The fact that 23% of students in Mexico said they use the new product, and a similar value was found with a sample of the general population (L: VCL, VC and AF, unpublished results), suggests that the information provided by mass media, parents, teachers, etc., generates awareness on the importance of cleaning hands, and thus, it would be useful if authorities define in the future if messages should pinpoint the use of tap water and soap or also alcohol gel.
Another interesting result of the present study was the finding that 66% of the students indicated covering nose and mouth with the forearm when sneezing. This is also new information that probably had a high rate of acceptance since there is no need of having a handkerchief at hand to reduce contamination, as only 9% of the students said they used a handkerchief for covering their months when sneezing.
The present study has some limitations, mainly because it is based on a questionnaire. It is unknown whether the responses given to the situations stated in the survey would accurately reflect the respondents’ real attitudes. The study also used a cross-sectional design, thus only associations rather than causal effects could be observed. Finally, the information obtained represents only one borough and one age group in Mexico City.
5. CONCLUSION
Seven out of ten students have adequate knowledge on influenza A (H1N1) but only four out of ten practice preventive measures. Parents and teachers play an important role in the transmission of health education, thus schools should take advantage of this fact in addition to mass media. The present study suggests that teachers provide a window of opportunity to improve personal hygiene in students by making available health education.
6. ACKNOWLEDGEMENTS
The authors wish to thank the authorities of all schools visited and, especially the students of the second grade of high school in the Miguel Hidalgo borough for their participation.This study was partially financed by CONACYT Salud 2004-01-086.
REFERENCES
- Cordova-Villalobos, J.A., Valdespno-Gomez, J.L. and Poncede-Leon, S. (2010) La epidemia de influenza A/ H1N1 en México. Editorial Medica Panamericana, 366.
- López-Cervantes, M., Venado, A., Moreno, A., PachecoDominguez, R.L. and Ortega-Pierres, G. (2009) On the spread of the novel influenza A (H1N1) virus in Mexico. Journal of Infection in Developing Countries, 3, 327-330. doi:10.3855/jidc.238
- Córdova, J.A., Sarti, E., Arzoz, J., Manuell, G., Romero, J. and Kuri, P. (2009) The influenza A (H1N1) epidemic in Mexico. Lessons learned. Health Research Policy and Systems, 7, 21. doi:10.1186/1478-4505-7-21
- World Health Organization (2009) Human infection with new influenza A (H1N1) virus: Mexico. Weekly Epidemiological Record, 84, 213-219.
- Secretaria de Salud del Gobierno de México. Influenza. 17 February 2011. http://portal.salud.gob.mx/contenidos/noticias/influenza/influenza_prin.html
- Narain, J.P., Kumar, R. and Bhatia, R. (2009) Pandemic (H1N1) 2009: Epidemiological, clinical and prevention aspects. National Medical Journal of India, 22, e1-e6.
- Balkhy, H.H., Abolfotouh, M.A., Al-Hathlool, R.H. and Al-Jumah, M.A. (2010) Awareness, attitudes, and practices related to the swine influenza pandemic among the Saudi public. BMC Infectious Diseases, 28, 42.
- Kamate, S., Agrawal, A., Chaudhary, H., Singh, K., Mishra, P. and Asawa, K. (2010) Public knowledge, attitude and behavioural changes in an Indian population during the influenza A (H1N1) outbreak. Journal of Infection in Developing Countries, 4, 7-14.
- Rubin, G.J., Amlôt, R., Page, L. and Wessely, S. (2009) Public perceptions, anxiety, and behaviour change in relation to the swine flu outbreak: Cross sectional telephone survey. BMJ Journal, 2, 2651.
- La Torre, G., Di Thiene, D., Cadeddu, C., Ricciardi, W. and Boccia, A. (2009) Behaviours regarding preventive measures against pandemic H1N1 influenza among Italian healthcare workers, October 2009. Eurosurveillance, 14, 19432.
- Secretaria, de S. (2010) Ley General de Salud 227, artículos 226, fracción IV, ultimo párrafo: Acuerdo por el que se determinan los lineamientos a los que estará sujeta la venta y dispensación de antibióticos. México.
- Flisser, A., Velasco-Villa, A., Martínez-Campos, C., González-Domínguez, F., Briseño, B., Caballero, A., MonroyI, G.H., Gutiérrez, L., Rodríguez, A., López-Martínez, I., Virgen, S., Vázquez, R., Balandrano, S., Guzmán-Bracho, C., Díaz, A., De la Rosa, J., Magos, C., Escobar-Gutiérrez, A. and Correa, D. (2002) Infectious diseases in Mexico. A survey from 1995-2000. Archives of Medical Research, 33, 343-350. doi:10.1016/S0188-4409(02)00381-8
- Lau, J., Griffiths, S., Choi, K. and Lin, C. (2010) Prevalence of preventive behaviors and associated factors during early phase of the H1N1 influenza epidemic. American Journal of Infection Control, 38, 374-380. doi:10.1016/j.ajic.2010.03.002
- Seale, H., McLaws, M.L., Heywood, A., Ward, K., Van Lowbridge, K.D., Gralton, J. and MacIntyre, R. (2009) The community’s attitude towards swine flu and pandemic influenza. Medical Journal of Australia, 191, 267- 269.
- Park, J., Cheong, H., Son, D., Kim, S. and Ha, C. (2010) Perceptions and behaviors related to hand hygiene for the prevention of H1N1 influenza transmission among Korean university students during the peak pandemic period. BMC Infectious Diseases, 10, 222. doi:10.1186/1471-2334-10-222
- Grayson, L.M., Melvani, S., Druce, J., Barr, I.G., Ballard, S., Johnson, P., Mastorakos, T. and Birch, C. (2009) Efficacy of Soap and Water and Alcohol-Based Hand-Rub Preparations against Live H1N1 Influenza Virus on the Hands of Human Volunteers. Clinical Infectious Diseases, 48, 285-291. doi:10.1086/595845