International Journal of Otolaryngology and Head & Neck Surgery
Vol.04 No.02(2015), Article ID:54615,8 pages
10.4236/ijohns.2015.42021
A Comparative Study on Efficacy of Fludrocortisones versus Glucocorticoids and Vasodilators in the Treatment of Idiopathic Sensorineural Cochlear Hearing Loss
Daniel López-Campos1, Daniel López-Aguado2, Eugenia M. Campos-Bañales2, José Luis de Serdio-Arias3, Mar García-Sáinz4
1ENT Service, University Hospital of the Canary Islands, Tenerife, Spain
2Department of Otorhinolaryngology, La Laguna University, Tenerife, Spain
3ENT Service, University Hospital Nuestra Señora de Candelaria, Tenerife, Spain
4Pharmacology and Pharmacotherapy Service, University Hospital of the Canary Islands, Tenerife, Spain
Email: emcampos@ull.es
Copyright © 2015 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 17 February 2015; accepted 9 March 2015; published 12 March 2015
ABSTRACT
Introduction and Objectives: The idiopathic sensorineural cochlear hearing loss is one of the most frequent human sensory deficits and there is no specific drug therapy for it. The possible hearing recovery is related with the reestablishment of normal ionic homeostasis of the endolymph controlled by the mineralocorticoid as could be demonstrate experimentally. The purpose of this clinical trial was to confirm the efficacy of mineralocorticoids to the recovery of hearing level in patients suffering idiopathic sensorineural hearing loss (SNHL) against the glucocorticoids and vasodilator drugs. Material and Methods: The research lasted three months and involved 90 patients allocated into four different groups: Placebo group, consisted of 20 patients (10 men and 10 women); the group consisting of 22 patients treated with glucocorticoid therapy (12 men and 10 female); the group treated with mineralocorticoid therapy encompassed 26 patients (13 males and 13 females) and the group of vasodilators formed by 22 patients (12 men and 10 women). The level of hearing loss was estimated by the tests Liminal Tone Audiometry (LTA) and Auditory Brainstem Response (ABR). Results: The main features in this research were overall better response in improving the hearing level with the mineralocorticoid therapy. This improvement in hearing levels was greater in women than in men, and a higher response was found in the left ear regardless of patient’s gender. Conclusions: The hearing gain was significantly superior in the mineralocorticoids group followed by the glucocorticoids group whereas the response to vasodilators was lesser and with no statistical significance.
Keywords:
Idiopathic Sensorineural Cochlear Hearing Loss (ISNCHL), Liminal Tonal Audiometry (LTA), Auditory Brainstem Response (ABR)

1. Introduction
Sensorineural hearing loss is a frequent human sensory deficit in the adult population and causes serious alteration to the hearing function in the patient due to underlying damage in the inner ear or in its neural pathways [1] [2] .
The pathogenesis of SNH is multifactorial and includes both intrinsic causes (genetic predisposition, autoimmune, vascular…) and extrinsic causes (toxic, infectious, degenerative, traumatic and neoplastic). It is not possible to know exactly what causes damage to the inner ear, resulting in alterations to cochlear transduction and transmission of acoustic signals [1] -[3] .
There is no specific drug therapy for sensorineural hearing loss [2] [3] . A majority of therapeutic approaches have focused on trials with therapies aimed at controlling its pathogenesis [4] -[9] . Recently a new hypothesis has related the decrease in hearing level in these pathologies to the imbalance of the ionic concentration of the inner ear, and the restoration of cochlear ion homeostasis, as the key concept to achieving hearing recovery [8] .
About 25 years ago, it was known that there were corticoid receptors in the inner ear, in both glucocorticoid and mineralocorticoid forms [10] [11] , and also at the Corti neuron and CNS [12] . Experimentally, it has been demonstrated that the mineralocorticoids are primarily involved in cochlear ionic regulation [13] [14] .
Up to this moment, we know of its effects through some animal experiments which have been carried out by several researchers [13] -[15] , but we do not know of any clinical studies about it.
The purpose of this paper, as a result of these experiments, is to defend the use of mineralocorticoid drugs to improve auditory level in adult patients with idiopathic sensorineural hearing loss.
2. Material and Methods
2.1. Financial Support
This clinical trial was funded by the Health Institute Carlos III after a call made for non-commercial clinical research projects on human drugs, and co-financed by the European Regional Development Fund (ERDF).
2.2. Sample Size
The study included a total of 90 patients who had been diagnosed of idiopathic bilateral sensorineural cochlear hearing loss (180 ears were studied).
2.3. Study and Patients
These 90 patients were divided into placebo group and treatment group and were treated during three months.
The patients came from two large university hospitals in “the autonomous region of The Canaries” who had been diagnosed of idiopathic sensorineural hearing loss. They were evaluated by the same health care professional, and regular monitoring was done by the same physician.
To take part in this study, it was required that patients were not taking vasodilators or steroids at that moment and at least in the three months prior to the start of the treatment. All patients were informed of the potential drawbacks of therapy and voluntarily consented to participate. All were studied again with gadolinium MRI to rule out pathology in the pontine angle.
The ages ranged between 19 and 71 years, 43 were women and 47 men (Figure 1 and Figure 2). All these were suffering from sensorineural bilateral, but not symmetrical, hearing loss. 85.5% were older 50 years old (Table 1). The patients were matched for age, sex and auditory level hearing loss.
The design was single blind, taking as reference the placebo group.
2.3.1. Treatment Groups
Patients in the trial were distributed into 4 standard groups in a randomized fashion (Figure 1 and Figure 2)
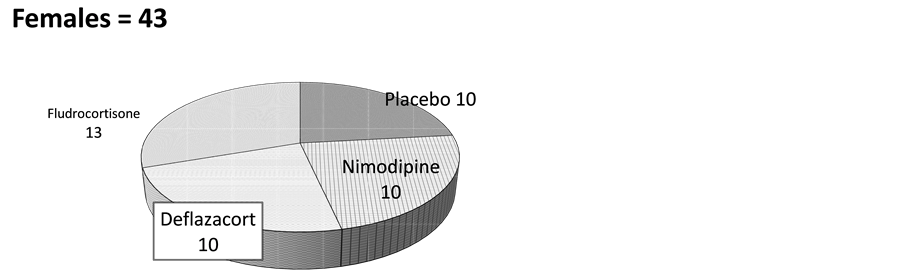
Figure 1. Distribution of female patients. According to treatment received.
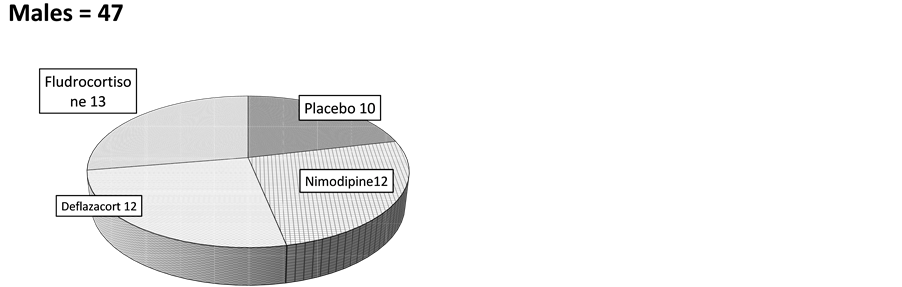
Figure 2. Distribution of male patients. According to treatment received.

Table 1. Percentage distribution of patients by age.
1) the placebo group, consisted of 20 patients, (10 of each sex), 2) another group of 22 patients were treated with glucocorticoids, deflazacort, (10 women and 12 men) at a dose 6 mg/12hours, 3) a group of 26 patients were treated with mineralocorticoids, fludrocortisone, (13 women and 13 men) at a dose 0.1 mg/12hours, and the last group 4) treated with vasodilators, nimodipine, was made up of 22 patients, (10 women and 12 men) at a dose 30 mg/every 8 hours.
Such therapy was individual and controlled for each patient, and the dose used was the minimal efficacy concentration among minimal margins of effectiveness, according to the literature consulted [8] .
Results at the end of the trial were analyzed in relation to the studied ear, patient age, sex and drugs used.
2.3.2. Methodology
1) Basal hearing level evaluation
Initially all patients were evaluated using liminal tonal audiometry (LTA) and with the auditory brainstem response test (ABR) every 15 days during the first two months and at the end of the study.
The diagnosis of sensorineural hearing loss and the degree of hearing level was held according to the criteria adopted by the World Health Organization (WHO) [2] .
Most had a liminal tone audiometry with greater decreases at high frequencies, the ABR showed no retro- cochlear involvement, with no increment in the interval I/V, and a pattern of cochlear hearing loss. We used the disappearance of the wave V to compare gradation hearing in relation to the liminal tonal audiometry.
The gradation of hearing level of patients was estimated in the range of conversational frequencies as follows: mild losses: <35 dBs; moderate loss: >35 dBs and <50 dBs; moderate-severe: >50 dBs and <60 dBs; severe: >60 dBs and <75 dBs and profound: >75 dBs. The final measure result was based in the average between the measurement obtained using LTA (liminal tonal audiometry), only in the conversational frequencies, and that achieved by ABR (auditory brainstem response).
The efficacy of treatment was achieved comparatively for each drug and by crossing the results with the use of the different drugs.
3. Statistical Analysis
Univariate and bivariate descriptive statistics by gender, age, affected ear and degree of hearing loss were conducted.
The Bonferroni statistical method (multiple comparisons) was used to compare the efficacy between the different drugs.
4. Results
A total of 90 patients were studied, from 19 to 70 years of age. About 86% of them were older than 50 years of age (Table 1).
In all groups asymmetric hearing loss predominated (Table 2).
Table 2. Initial percentage classification of hearing level, in all patients.
RE = right ear; LE = left ear; N˚ ptes = n˚ patients; dBs = decibels.
Mainly the left ear exhibited a severe-deep hearing loss (27.35%) compared with the right ear (20.64%) while the right ear showed a high prevalence of hearing loss moderate-severe (78.35%) compared with the left ear (72.72%) (Table 3).
After treatment, the left ear had a higher increase in hearing (Figure 3) regardless of the sex of the patients (Figure 4). This increase was more evident in the fludrocortisone group (Figure 5, Table 4). There was a better response in women than in men, in all groups (Figure 4).
Table 3. Total percentage of binaural hearing loss, in all patients.
Table 4. Comparison of auditory gains by sex, ear and drug used Bonferroni method (multiple comparisons).
RE = right ear, LE = left ear, P = statistical significance.
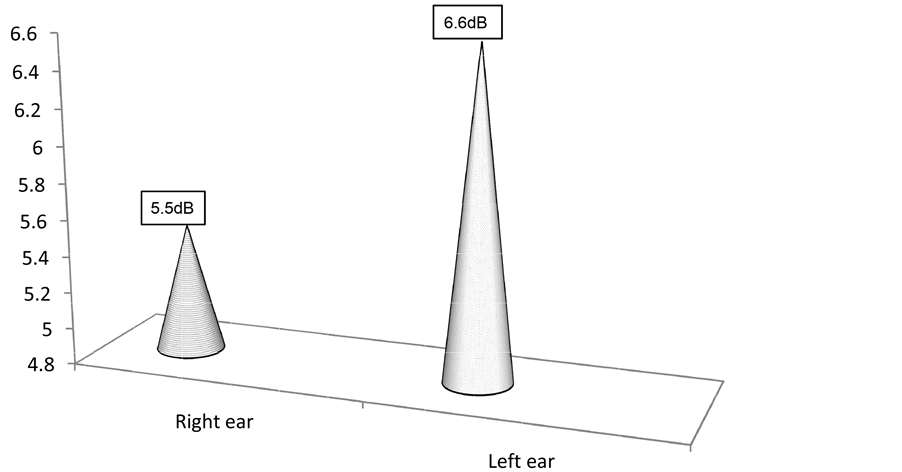
Figure 3. Average increase in hearing recovery, dB, in all ears at study end.
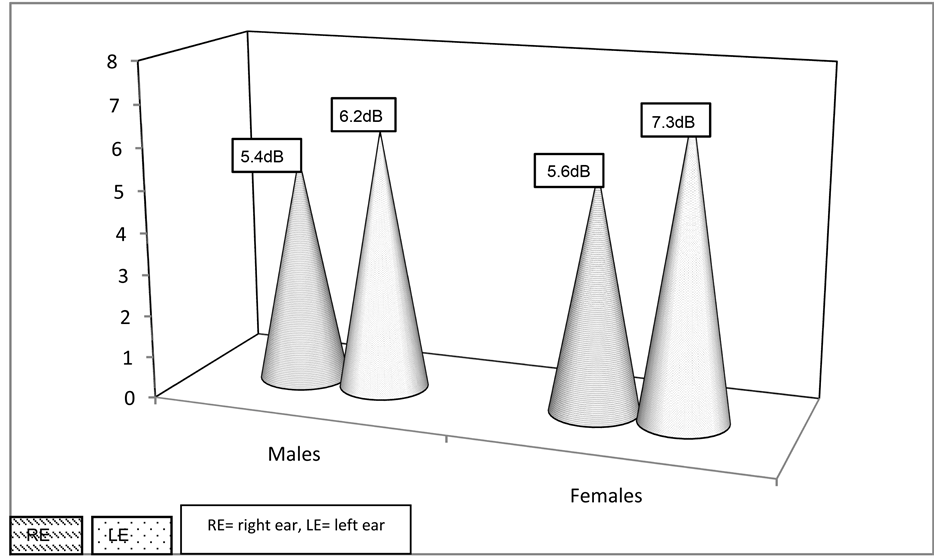
Figure 4. Average increase in binaural hearing recovery, dB, according to patient’s sex.
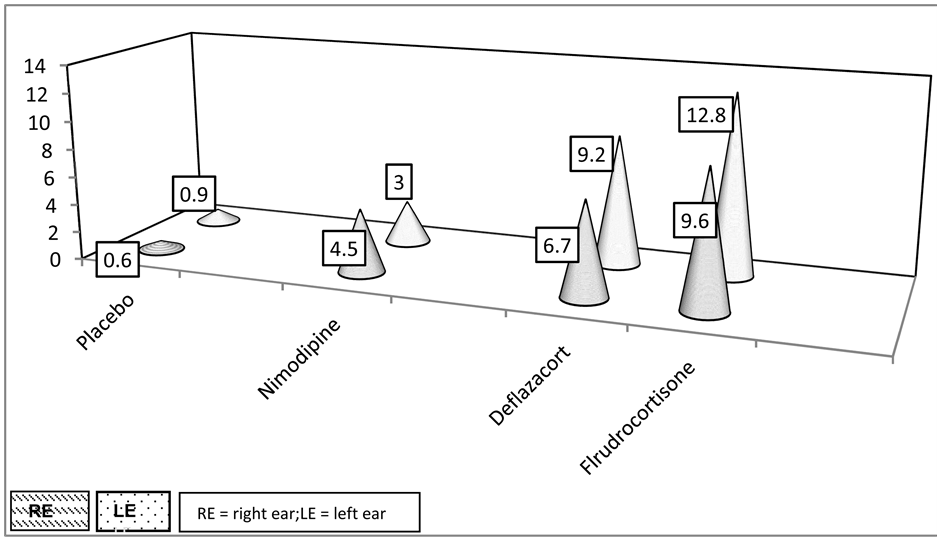
Figure 5. Average increase in hearing recovery, dB, for both ears, according to treatment group.
4.1. Characteristics by Group
4.1.1. Placebo Group
It comprised 20 people, 10 men and 10 women (Figure 1 and Figure 2), who exhibited bilateral sensorineural hearing loss (Table 2).
Right ear: mild to moderate in 15 people (75%), and moderate to severe in 5 (25%). In the left ear: mild- moderate loss in 6 patients (30%), moderate-severe in 6 (30%) and severe in 8 (40%) The variations in the level of hearing at the end of the study were of 0.6 dBs for the right ear, and 0.9 dBs in the left one (Figure 5).
4.1.2. The Group of Patients Treated with Deflazacort
It was composed of 22 patients, 12 men and 10 women, with bilateral sensorineural hearing loss (Table 2).
In the right ear: mild to moderate loss in 10 patients (45%), moderate to severe in 5 patients (22.7%), severe in 5 (22.7%) and profound in 2 patients (9.6%). In the left ear: mild to moderate in 14 patients (63.6%), moderate to severe in 3 patient (13.6%), severe in 3 (13.6%) and profound in 2 patients (9.2%).
In these patients we found a gain of 6.7 dBs in the right ear and 9.2 dBs in the left ear (Figure 5).
4.1.3. Group Treated with Fludrocortisone
The group consists of 26 patients, 13 men and 13 women exhibiting bilateral sensorineural hearing loss (Table 2).
Right ear: mild to moderate in 16 cases (61.5%), moderate to severe in 3 cases (11.6%) and severe in 7 cases (26.9%).
In the left ear: mild-moderate loss in 18 patients (69.2%), moderate to severe in 3 cases (11.6%), severe in 4 (15.3%) and profound in 1 (3.9%).
We found an average hearing gain of about 9.6 dBs in the right ear, and 12.8 dBs in the left ear (Figure 5).
4.1.4. Group Treated with Nimodipine
Made up of 22 people, 12 men and 10 women, who were suffering binaural sensorineural hearing loss (Table 2).
In the right ear the loss was: mild to moderate in 12 patients (54.5%) moderate to severe in 4 patients (18.1%) severe in 4 patients (18.1%) and profound in 2 patients (9.3%). In the left ear the loss was: mild to moderate in 14 patients (63.6%), moderate to severe in 2 patients (9.3%) and severe in 6 (27.1%).
At the end of the study we found an average increase of 4.5 in dB for the right ear and 3.0 dB in the left one (Figure 5).
4.2. Final Valuation of the Results Achieved
The estimation of hearing gain achieved at the end of the study comparing with the initial hearing grade, was carried out individually for each ear (Figure 3), sex (Figure 4) and each one of the drugs used (Figure 5).
With the Bonferroni study we verified the efficacy of different drugs, achieved by multiple comparisons between them.
4.3. Valuation of the Side Effects
Overall there were no side effects, only small increments in blood pressure in 3 patients treated with deflazacort (13.6%) and 7 patients treated with fludrocortisones (26.8%). The blood pressure increase was normalized using a thiazidic diuretic drug.
5. Discussion
Hearing impairment is one of the six leading contributors to the burden of disease in industrialized countries, and it is one of the conditions that most severely impair the quality of life of those who suffer from it [2] [3] .
There are two forms of hearing impairment: the conductive and the sensorineural one. The latter form resulting from either damage to the sensory cells of the inner ear-secondary to an impaired inner cochlear homeostasis- or from different diseases affecting the cochlear nerve (including its synapses) [2] .
Idiopathic sensorineural hearing loss is predominant in middle-aged adults, and it is equally distributed by gender [1] [2] , although, in this study, we found a non-significant higher prevalence in males (Figure 1 and Figure 2).
Conductive hearing loss has various possibilities of treatment, whereas there is no specific drug therapy for sensorineural hearing loss, apart from symptomatic approaches with moderate efficacy [2] -[7] .
One of the main reasons for the absence of specific tools to cure or prevent SNHL is the insufficient knowledge about the basic molecular mechanisms of normal and impaired adult hearing, thus therapeutic measures have focused on the recovery of hearing levels by trying to control its pathogenesis [1] -[9] .
The hypothesis argued, in the case of sudden hearing loss, and in hearing loss secondary to acoustic trauma, is that it is caused by alterations to the hemodynamics of the cochlear level which end up ischemic injury, which could be controlled with vasodilators drugs [5] [6] . This therapy which we use, thinking that some of these factors could have pathogenetic implications, does not show to be effective for hearing recovery.
There is well documented evidence on the use of steroids in the treatment of pathologies of the inner ear [8] and has also been proved by different studies that demonstrate that there is a great amount of steroid receptors in the inner ear, not only in its neurons [12] but also in the Corti organ―here mainly concentrated in the cochlear stria vascularis [10] [11] whose mission is that of regulating the endolymphatic ionic balance.
It has been demonstrated by Trune et al. [13] , in the autoimmune mouse, that mineralocorticoids are the key regulators of this balance [13] [14] and on this basis most researches advocate for glucocorticoids as the effective therapy for patients suffering from immune-mediate or inflammatory deafness processes, whereas mineralo- corticoids should be used in the treatment of idiopathic or not well defined deafness [13] -[15] .
Based on these findings, and with the evidence that the restoration of hearing with steroid treatment is due to increased stria sodium-potassium transport, to reestablish normal ionic balances in the endolymph, our study was aimed at demonstrating if it has any application in a clinical model.
This study aims to demonstrate the efficacy of mineralocorticoids in patients suffering from idiopathic cochlear hearing loss and to draw contrast with glucocorticoids and also with vasodilators drugs.
In all treated patients we observed a gain in binaural hearing, greater in the group treated with steroids than in the group treated with vasodilators, and it was much more significant with the mineralocorticoids (Figure 5, Table 4).
We found better response in women, and hearing recovery was greater in the left ear (Figure 3 and Figure 4). We cannot give a justification for such results.
In all patients blood pressure side effects were easily regulated with thiazide treatment.
6. Conclusions
Mineralocorticoid therapy is effective in improving hearing function in patients with idiopathic HNS with cochlear BRA pattern.
Its use provides statistically significant results, higher than those observed with the use of glucocorticoids.
Vasodilator drugs lack these beneficial effects in the restoration of the hearing levels in these pathologies.
Side effects of steroids therapy can be easily controlled.
Acknowledgements and Economic Support
Funded through the Carlos III Health Institute agreement to carry out non-commercial clinical trials involving human drugs, co-financed by the European Regional Development Fund (ERDF).
Conflict of Interest
All authors of this study certify that there is no conflict of interest with any organization and that there is no financial or non-financial interest in the subject matter or materials discussed in this manuscript. This is an original study.
References
- Berretini, S., Ravecca, F., Forli, F., Sellari-Franceschini, S. and Piragine, F. (1998) Diagnostic and Therapeutic Approach to Progressive Sensorineural Hearing Loss. Acta Otorhinolaryngologica Italica, 18, 87-94.
- Yamasoba, T., Lin, F.R., Someya, S., Kashio, A., Sakamoto, T. and Kondo, K. (2013) Current Concepts in Age-Re- lated Hearing Loss: Epidemiology and Mechanistic Pathways. Hearing Research, 16, 95-105.
- Zahnert, T. (2011) The Differential Diagnosis of Hearing Loss. Deutsches Ärzteblatt international, 108, 433-444.
- Sekiya, T., Hatayama, T., Shimamura, N. and Suzuki, S. (2000) An in Vivo Quantificable Model of Cochlear Neuronal Degeneration Induced by Central Process Injury. Experimental Neurology, 161, 409-502. http://dx.doi.org/10.1006/exnr.1999.7280
- Fish, U., Nagahara, K. and Pollak, A. (1984) Sudden Hearing Loss Circulatory. American Journal of Otolaryngology, 5, 488-491.
- Kansy, L., Ozkarakas, H., Efendi, H. and Okar, I. (2011) Protective Effects of Pentoxifylline and Nimodipine on Acoustic Trauma in Guinea Pig Cochlea. Otology Neurotology, 32, 19-25.
- Polon, Y.G., Humli, V., Andó, R., Aller, M., Horváth, T., Harnos, A., Tamás, L., Vizi, E.S. and Zelles, T. (2014) Protective Effect of Rasagiline in Aminoglycoside Ototoxicity. Neuroscience, 265, 263-273. http://dx.doi.org/10.1016/j.neuroscience.2014.01.057
- Trune, D.R. and Canlon, B. (2012) Corticosteroid Therapy for Hearing and Balance Disorders. Anatomical Record, 295, 1928-1943. http://dx.doi.org/10.1002/ar.22576
- Rita Fetoni, A., Bartolo, P., Eramo, S.L., Rolesi, R., Pacielo, F., et al. (2013) Noise-Induced Hearing Loss (NIHL) as a Target of Oxidative Stress-Mediated Damage: Cochlear and Cortical Responses Alter an Increase in Antioxidant Defense. The Journal of Neuroscience, 33, 4011-4023. http://dx.doi.org/10.1523/JNEUROSCI.2282-12.2013
- Rarey, K.E. and Curtis, L.M. (1996) Receptors for Glucocorticoids in the Human Inner Ear. Otolaryngology―Head and Neck Surgery, 115, 38-41. http://dx.doi.org/10.1016/S0194-5998(96)70133-X
- Sinha, P.K. and Pitovsky, D.Z. (1995) 3-H-Aldosterone Bingind Sites (Type I Receptors) in the Lateral Wall of the Cochlea: Distribution Assessment by Quantitative Auto Radiography. Acta Oto-Laryngologica, 115, 643-647. http://dx.doi.org/10.3109/00016489509139380
- Jin, D.X., Lin, Z., Lei, D. and Bao, J. (2009) The Role of Glucocorticoids for Spiral Ganglion Neuron Survival. Brain Research, 1277, 3-11. http://dx.doi.org/10.1016/j.brainres.2009.02.017
- Trune, D.R. and Kempton, J.B. (2001) Aldosterone and Prednisolone Control of Cochlear Function in MRL/MpJ- Fas(lpr) Autoimmune Mice. Hearing Research, 155, 9-20. http://dx.doi.org/10.1016/S0378-5955(01)00240-4
- Trune, D.R., Kempton, J.B. and Gross, N.D. (2006) Mineralocorticoid Receptor Mediates Glucocorticoid Treatment Effects in the Autoimmune Mouse Ear. Hearing Research, 212, 23-32. http://dx.doi.org/10.1016/j.heares.2005.10.006
- Trune, D.R., Kempton, J.B., Harrison, A.R. and Wobig, J.L. (2007) Glucocorticoid Impact on Cochlear Function and Systemic Side Effects in Autoimmune C3MRL-Fask or and Normal C3H-Hej Mice. Hearing Research, 226, 209-212. http://dx.doi.org/10.1016/j.heares.2006.09.011