Paper Menu >>
Journal Menu >>
 Vol.1, No.4, 298-303 (2009) doi:10.4236/health.2009.14049 SciRes Copyright © 2009 Openly accessible at http://www.scirp.org/journal/HEALTH/ Health Health status of transitional resettlement sites after the earthquake in Mianyang city of Sichuan province Ying-Hua Li, Ling Qian, Xue-Qiong Nie, Li LI, Xian-Peng Meng, Jin-Bin Zhang, Li Tong, Li Xiao, He Xing, Chang-Sheng Huang, Tao Hu, Yan Ning, Yan Chen, Yu Ma, Mao-Xuan Tao Chinese Center for Health Education, Beijing, China; liyinghua729@sina.com Received 5 August 2009; revised 1 September 2009; accepted 1 September 2009. ABSTRACT Objective: To understand the health status of transitional resettlement sites and the needs of residents on health education, and to pro- vide basis for conducting health education after ear- thquakes and other public emergen- cies. Method: From May 31 to June 2, 2008 (19 to 21 days after the earthquake), field obser- vation, questionnaire survey, and structured interviews were conducted in five transitional resettlement sites. Information on health status, health service, health education, and residents’ needs on health education was col- lected. Results: 430 questionnaires were dis- tributed and 424 valid completed ones were returned. Food and water were adequately supplied. Clinics for health assistance were established and environment disinfecting was conducted regularly by public health profes- sionals. Health education was available to residents. The large proportion (98.6%, 97.9%, 88.7%, and 93.2% respectively) of the residents acknowledged that water supply, food supply, lavatories, and health service were adequate to fulfill basic needs. The overall disease in- cidence of surveyed residents was 44.8%, and diarrhea and fever with respiratory symptoms were the most common diseases. Among residents’ needs on disease prevention knowl- edge and skills, basic knowledge of infectious diseases was most desirable (49.8%), and safety knowledge of water uses was secon- darily most desirable (36.8%). The most fa- vored approach of obtaining knowledge was watching television. Conclusions: In the pe- riod of 20 days after the earthquake, Living security, health facilities, and health care ser- vice could satisfy residents’ basic needs. Post-disaster health education should con- centrate on basic knowledge and skills of communicable diseases and health- risky be- havior. Timely distributing disease prevention materials could be effective. Keywords: Earthquake; Disaster Areas; Health Status; Health Education; Needs; 1. INTRODUCTION On May 12, 2008, an earthquake with magnitude 8.0 hit Wenchuan, Sichuan Province. The quake caused thou- sands of deaths and injured, destroyed buildings and roads, and brought about huge financial loss. In the af- fected area, water and electricity supply were interrupted, and health care facilities and systems were enormously damaged, which resulted in the high risk for the outbreak and epidemic of intestinal communicable diseases, vec- tor-borne diseases, food-borne diseases, diseases of natural focus, and infectious diseases transmissible be- tween human and animals. Food and water safety, envi- ronmental health, health care service, and post-earthquake health education were the most impor- tant issues in disaster relief. To understand the health condition of transitional resettlement sites and residents’ needs on health education, Health Education Institute, Chinese Center for Disease Control and Prevention (China CDC) (Note:now named Chinese Center for Health Education/ Heath News Communication Center, Ministry of Health of China) conducted this study from May 31 to June 2, 19 to 21 days after the earthquake. 2. METHODS 2.1. Participant The resident in five transitional resettlement sites in Mianyang city, Sichuan Province were surveyed by the same questionnair, and they were from Beichuan county, one of the worst-hit areas. Four hundred and thirty questionnaires were distributed, and four hun- dred and twenty four valid questionnaires were re- 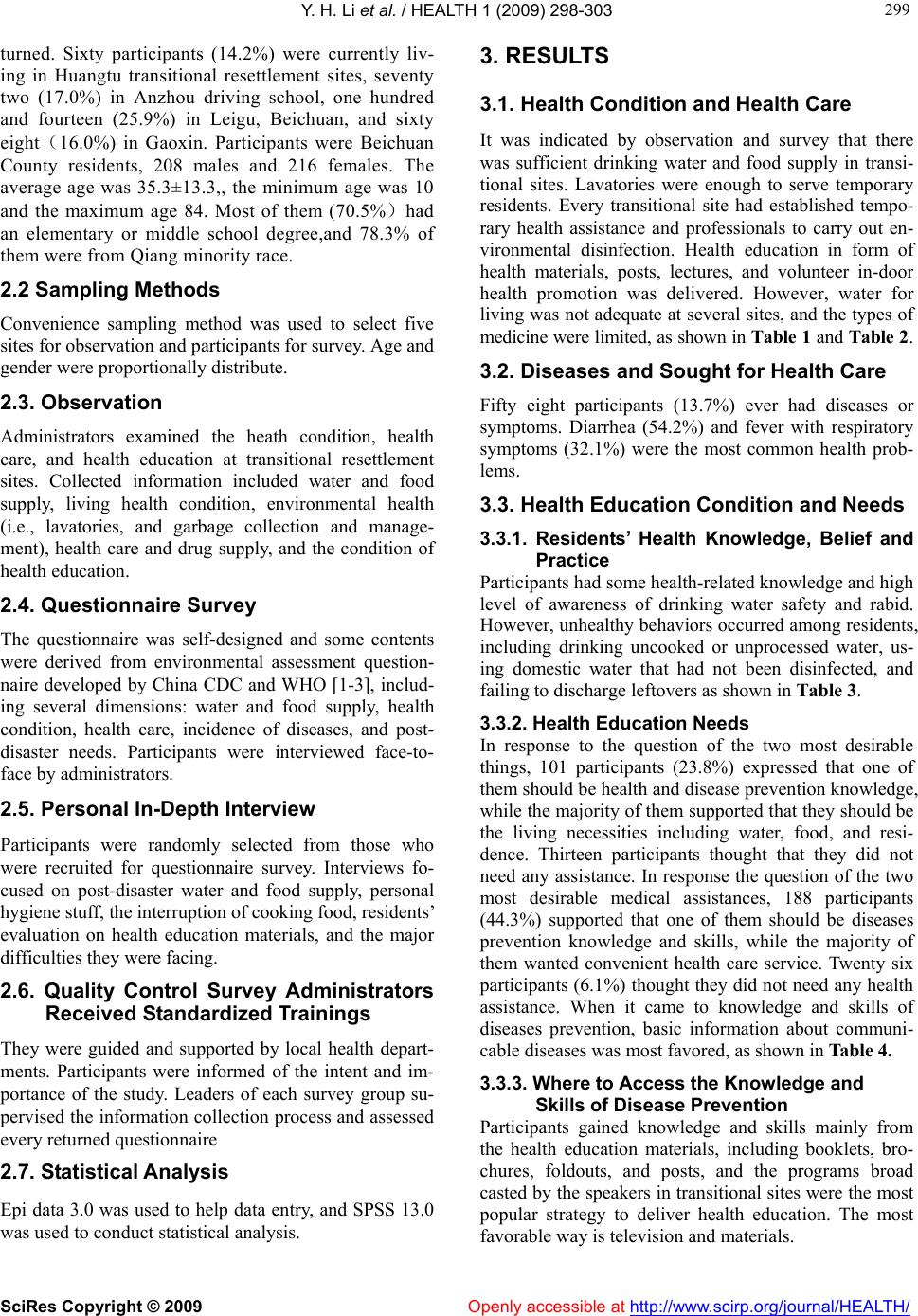 Y. H. Li et al. / HEALTH 1 (2009) 298-303 SciRes Copyright © 2009 Openly accessible at http://www.scirp.org/journal/HEALTH/ 299 299 turned. Sixty participants (14.2%) were currently liv- ing in Huangtu transitional resettlement sites, seventy two (17.0%) in Anzhou driving school, one hundred and fourteen (25.9%) in Leigu, Beichuan, and sixty eight(16.0%) in Gaoxin. Participants were Beichuan County residents, 208 males and 216 females. The average age was 35.3±13.3,, the minimum age was 10 and the maximum age 84. Most of them (70.5%)had an elementary or middle school degree,and 78.3% of them were from Qiang minority race. 2.2 Sampling Methods Convenience sampling method was used to select five sites for observation and participants for survey. Age and gender were proportionally distribute. 2.3. Observation Administrators examined the heath condition, health care, and health education at transitional resettlement sites. Collected information included water and food supply, living health condition, environmental health (i.e., lavatories, and garbage collection and manage- ment), health care and drug supply, and the condition of health education. 2.4. Questionnaire Survey The questionnaire was self-designed and some contents were derived from environmental assessment question- naire developed by China CDC and WHO [1-3], includ- ing several dimensions: water and food supply, health condition, health care, incidence of diseases, and post- disaster needs. Participants were interviewed face-to- face by administrators. 2.5. Personal In-Depth Interview Participants were randomly selected from those who were recruited for questionnaire survey. Interviews fo- cused on post-disaster water and food supply, personal hygiene stuff, the interruption of cooking food, residents’ evaluation on health education materials, and the major difficulties they were facing. 2.6. Quality Control Survey Administrators Received Standardized Trainings They were guided and supported by local health depart- ments. Participants were informed of the intent and im- portance of the study. Leaders of each survey group su- pervised the information collection process and assessed every returned questionnaire 2.7. Statistical Analysis Epi data 3.0 was used to help data entry, and SPSS 13.0 was used to conduct statistical analysis. 3. RESULTS 3.1. Health Condition and Health Care It was indicated by observation and survey that there was sufficient drinking water and food supply in transi- tional sites. Lavatories were enough to serve temporary residents. Every transitional site had established tempo- rary health assistance and professionals to carry out en- vironmental disinfection. Health education in form of health materials, posts, lectures, and volunteer in-door health promotion was delivered. However, water for living was not adequate at several sites, and the types of medicine were limited, as shown in Table 1 and Table 2. 3.2. Diseases and Sought for Health Care Fifty eight participants (13.7%) ever had diseases or symptoms. Diarrhea (54.2%) and fever with respiratory symptoms (32.1%) were the most common health prob- lems. 3.3. Health Education Condition and Needs 3.3.1. Residents’ Health Knowledge, Belief and Practice Participants had some health-related knowledge and high level of awareness of drinking water safety and rabid. However, unhealthy behaviors occurred among residents, including drinking uncooked or unprocessed water, us- ing domestic water that had not been disinfected, and failing to discharge leftovers as shown in Table 3. 3.3.2. Health Education Needs In response to the question of the two most desirable things, 101 participants (23.8%) expressed that one of them should be health and disease prevention knowledge, while the majority of them supported that they should be the living necessities including water, food, and resi- dence. Thirteen participants thought that they did not need any assistance. In response the question of the two most desirable medical assistances, 188 participants (44.3%) supported that one of them should be diseases prevention knowledge and skills, while the majority of them wanted convenient health care service. Twenty six participants (6.1%) thought they did not need any health assistance. When it came to knowledge and skills of diseases prevention, basic information about communi- cable diseases was most favored, as shown in Table 4. 3.3.3. Where to Access the Knowledge and Skills of Disease Prevention Participants gained knowledge and skills mainly from the health education materials, including booklets, bro- chures, foldouts, and posts, and the programs broad casted by the speakers in transitional sites were the most popular strategy to deliver health education. The most favorable way is television and materials. 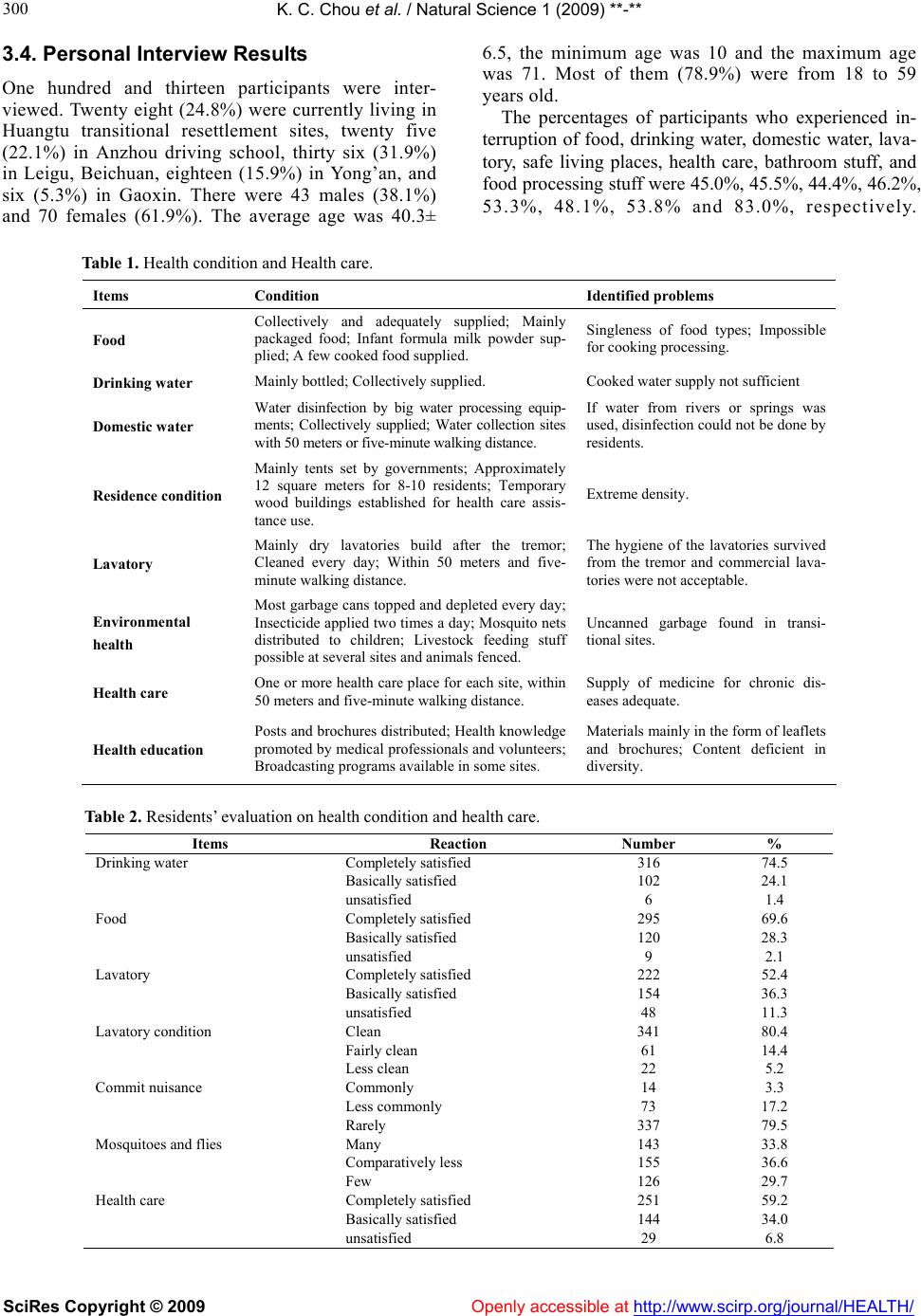 K. C. Chou et al. / Natural Science 1 (2009) **-** SciRes Copyright © 2009 http://www.scirp.org/journal/HEALTH/ 300 3.4. Personal Interview Results One hundred and thirteen participants were inter- viewed. Twenty eight (24.8%) were currently living in Huangtu transitional resettlement sites, twenty five (22.1%) in Anzhou driving school, thirty six (31.9%) in Leigu, Beichuan, eighteen (15.9%) in Yong’an, and six (5.3%) in Gaoxin. There were 43 males (38.1%) and 70 females (61.9%). The average age was 40.3± 6.5, the minimum age was 10 and the maximum age was 71. Most of them (78.9%) were from 18 to 59 years old. The percentages of participants who experienced in- terruption of food, drinking water, domestic water, lava- tory, safe living places, health care, bathroom stuff, and food processing stuff were 45.0%, 45.5%, 44.4%, 46.2%, 53.3%, 48.1%, 53.8% and 83.0%, respectively. Table 1. Health condition and Health care. Items Condition Identified problems Food Collectively and adequately supplied; Mainly packaged food; Infant formula milk powder sup- plied; A few cooked food supplied. Singleness of food types; Impossible for cooking processing. Drinking water Mainly bottled; Collectively supplied. Cooked water supply not sufficient Domestic water Water disinfection by big water processing equip- ments; Collectively supplied; Water collection sites with 50 meters or five-minute walking distance. If water from rivers or springs was used, disinfection could not be done by residents. Residence condition Mainly tents set by governments; Approximately 12 square meters for 8-10 residents; Temporary wood buildings established for health care assis- tance use. Extreme density. Lavatory Mainly dry lavatories build after the tremor; Cleaned every day; Within 50 meters and five- minute walking distance. The hygiene of the lavatories survived from the tremor and commercial lava- tories were not acceptable. Environmental health Most garbage cans topped and depleted every day; Insecticide applied two times a day; Mosquito nets distributed to children; Livestock feeding stuff possible at several sites and animals fenced. Uncanned garbage found in transi- tional sites. Health care One or more health care place for each site, within 50 meters and five-minute walking distance. Supply of medicine for chronic dis- eases adequate. Health education Posts and brochures distributed; Health knowledge promoted by medical professionals and volunteers; Broadcasting programs available in some sites. Materials mainly in the form of leaflets and brochures; Content deficient in diversity. Table 2. Residents’ evaluation on health condition and health care. Items Reaction Number % Drinking water Completely satisfied 316 74.5 Basically satisfied 102 24.1 unsatisfied 6 1.4 Food Completely satisfied 295 69.6 Basically satisfied 120 28.3 unsatisfied 9 2.1 Lavatory Completely satisfied 222 52.4 Basically satisfied 154 36.3 unsatisfied 48 11.3 Lavatory condition Clean 341 80.4 Fairly clean 61 14.4 Less clean 22 5.2 Commit nuisance Commonly 14 3.3 Less commonly 73 17.2 Rarely 337 79.5 Mosquitoes and flies Many 143 33.8 Comparatively less 155 36.6 Few 126 29.7 Health care Completely satisfied 251 59.2 Basically satisfied 144 34.0 unsatisfied 29 6.8 Openly accessible at  Y. H. Li et al. / HEALTH 1 (2009) 298-303 SciRes Copyright © 2009 Openly accessible at http://www.scirp.org/journal/HEALTH/ 301 301 Table 3. Health knowledge, belief, and practice. Questions The number of yes responses % Knowledge and belief Drinking uncooked or unprocessed water could do harm to health.402 94.8 Do not share washbasins and towels with relatives who had pink- eye disease. 295 69.6 Rabid vaccine is needed after being biting or scratched by dogs and cats. 391 92.2 Behavior Ever drunk uncooked or unprocessed water 55 13.0 Disinfected domestic water that was collected by themselves (n=110)* 51 46.3 Ate overdue food (n=167)* 6 3.6 Discharged waste water everywhere 27 6.4 Cleaned garbage everyday 62 14.6 Made efforts to prevent mosquitoes, flies, and rats 195 46.0 Ventilated living places 378 89.2 Washed hands before meals and after using the restroom. 396 93.4 Leftover reheating (n=163)* Completely reheated 123 75.5 Just warmed 16 9.8 Did not reheat, because of lack of needed equipments 19 11.7 Did not reheat, since it is not needed 5 3.1 Separated the raw and the cooked (n=58)* Yes. 54 93.1 No, since not allowed by living situations. 4 6.9 No, since it is not needed. 0 0.0 Note:* indicated that only those ever had overdue food, needed stuff for cooking, and self collected water were surveyed. Table 4. Participants’ needs on general support, health care, and disease prevention. Items Number % General supports(The most desirable two) Safe living places 259 61.1 Sufficient water and food supply 178 42.0 Knowledge and skills of health and diseases prevention 101 23.8 Ability and skills of escaping from the tremor and helping each other 63 14.9 Psychological assistance 26 6.1 Others 65 15.3 Needs on health and disease prevention(The most desirable two) Convenient health care service 191 45.0 Knowledge and skills 188 44.3 Disinfectants 182 42.9 Medicines 4 0.9 Needs on knowledge and skills of disease prevention Basic knowledge of communicable diseases 211 49.8 Drinking water safety 156 36.8 Food safety 140 33.0 Prevent mosquitoes, flies, and rats 132 31.3 Local communicable diseases 126 29.7  Y. H. Li et al. / HEALTH 1 (2009) 298-303 SciRes Copyright © 2009 Openly accessible at http://www.scirp.org/journal/HEALTH/ 302 Table 5. Where to access the knowledge and skills of disease prevention. Already gained Expected to gain Where Number % Number % Television 131 30.9 195 46.0 Broadcasting 159 37.5 127 30.0 Newspapers 102 24.1 94 22.2 Books 61 14.4 89 21.0 Medical professionals 100 23.6 123 29.0 CDC staff 123 29.0 126 29.7 Relatives/ friends 62 14.6 42 9.9 Propaganda materials 209 49.3 160 37.7 The speakers in tran- sitional sites 24 5.7 20 4.7 Never gained 22 5.2 — — Although the problem of cooking food remained unre- solved, other life necessities were fully supplied by gov- ernments. The total period of the interruption was con- trolled to be within two days at every site. The existing difficulties include the singleness of food which caused digest problems and stomach upset of the elder and chil- dren, extreme density of living places where both tem- perature and humidity were at a high level, lacking of bathing stuff, children education, job interruption, the loss of household asset, and financial crisis. 86.9% of participants supported that post-earthquake health education was needed, and 41.6% of them thought that brochures and books were the best method of educa- tion since the content could contain a wide range of in- formation, be systematic, and be understandable. 78.2% of them had a positive evaluation toward the delivered or posted health education materials. 4. DISCUSSION The survey was conducted 19-21 days after the earth- quake. The results indicated that basic life necessities and health care facilities and service could fulfill resi- dents’ needs. Water and food supply were adequate, and there were sufficient lavatories and garbage recycling sites that were cleaned every day. Environmental disin- fection, mosquito, fly, and rat prevention had remarkable effects. Few flies and rats were observed by residents. However, many problems had been identified. There is the risk of food safety issue since food was from outside of the earthquake hit areas [4]. The mainly supplied food was packaged noodles and cookies, which could effec- tively prevent intestinal infectious diseases. However, more efforts should be made to enrich the types of food and provide appropriate food to the elder and children. It was fairly crowded in temporary tents where the tem- perature and humidity were high. Tents were not enough to ensure family as the small unit to be accommodated. Many health care sites only had emergency drugs like anti-bacteria and flu treatment drugs, but the drugs for chronic disease such as high blood pressure and diabetes were not enough to satisfy the needs. Moreover, the bathing stuff were so insufficient that residents could not shower every day. There were three kinds of lavatories available at each site: dry ones established after the tremor, remaining ones that survived from the tremor, and commercial mo- bile lavatories. The dry lavatories were the most appro- priate ones for environmental health. They were easy to build at a lower cost and could serve many people. The other two kinds of lavatory could not be cleaned easily since the water supply was interrupted, which could re- sult in the proliferation of flies and mosquitoes [5]. Ad- ditionally, commercial mobile lavatories were not easy to transport and their cost was high. Thus, it was sug- gested that dry lavatories should be established in time after earthquake. The most common health problems among residents were diarrhea, fever with respiratory symptoms, heat- stroke, cold, and dermatitis. The post-tsunami effects caused by stress sources such as lifestyle changes, the death of relative, and the loss of incomes could cause disorders of the immune system, make residents vulner- able to varieties of diseases. The density and humidity of the residence might be the cause for dermatitis. The environment changed dramatically after the earthquake. If residents lacked the knowledge and will- ingness of disease prevention, or there were not enough health facilities such as lavatories, personal hygiene stuff, or even if related facilities were available but residents did not have a healthy behavior pattern, communicable disease could break out easily. Thus, post-earthquake health education was highly important. According to the results of the survey, residents had some unhealthy be- haviors, like using non-disinfected river water as living water. Post-earthquake health education should follow the principles applying to outbreak public health emer- gencies, be delivered in time, and focus on those at high risk[6]. Booklets/brochures were the most favorable ma- terials since they can have a wide range of information, be systematic and understandable, be kept easily. Tele- vision was the most method favored by the residents. It was highly appropriate for those who receive less educa- tion. As residents were being relocated, televisions should be equipped. Furthermore, the speakers at each site should be fully used to implement health education. REFERENCES [1] Chinese Center for Disease Control and Prevention. (2008) A quickly assessment table of the needs of the public health and disease control in earthquake areas [EB]. http://www.chinacdc.net.cn. [2] Chinese Center for Disease Control and Prevention. (2008) The assessment keys of the food hygiene in earthquake areas in earthquake areas [EB]. http://www.chinacdc.net.cn.  Y. H. Li et al. / HEALTH 1 (2009) 298-303 SciRes Copyright © 2009 http://www.scirp.org/journal/HEALTH/Openly accessible at 303 303 [3] WHO Regional Office for South-East Asia. (2004) Rapid needs assesment for water, sanitation and hygiene [EB]. http://www.who.org.mv/EN/Index.htm. [4] Fan, Y.X., Cui, W.M. and Liu, X.M. (2008) The ques- tions and countermeasures of food hygiene in Wenchuan areas with earthquake [J]. Chinese Journal of Food Hy- giene (in Chinese), 20(4), 291-293. [5] Hui, B. (2008) The deject arrangement and disease hid- den trouble in earthquake areas [J]. Chinese Journal of Border Hygiene Tests and Quarantine (in Chinese), 31(3), 207-208. [6] Hu, J.F. (2004) Heath education and heath promotion in public health emergency [J]. Chinese Journal of Health Education (in Chinese), 20(2), 126-128. |