International Journal of Otolaryngology and Head & Neck Surgery
Vol.3 No.4(2014), Article
ID:47713,5
pages
DOI:10.4236/ijohns.2014.34037
Kimura’s Disease—A Rare Cause of Head and Neck Swelling
Kiran Rao1, Sudesh Kumar2
1SGRD Institute of Medical Sciences and Research, Amritsar, India
2Oral and Maxillofacial Surgery, Institute of Dental Sciences, Jammu, India
Email: drkiranrao25@yahoo.com
Copyright © 2014 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 16 April 2014; revised 15 May 2014; accepted 14 June 2014
ABSTRACT
Kimura’s disease (KD) is a chronic inflammatory disorder with unknown etiology, most commonly manifesting as painless unilateral cervical lymphadenopathy or subcutaneous masses in the head or neck region. The disease is characterized by a triad of painless subcutaneous masses in the head or neck region, blood and tissue eosinophilia, and markedly elevated serum immunoglobulin E levels. Kimura’s disease is an unusual vascular tumor that typically occurs at 20 to 30 years of age. There has been no documented case of malignant transformation; however, recurrence rates after excision may be as high as 25%. Surgery and medical therapy are useful for treatment. We present a 14 years old male developed a unilateral cervical mass associated with KD. It was a recurrence of disease. As a complete excisional resection of the mass already done 1 year back at some other centre, we decided to give medical treatment for Kimura’s disease.
Keywords:Kimura’s Disease, Eosinophilia, Neck Swelling

1. Introduction
Kimura’s disease is a benign rare chronic inflammatory disorder. Its primary symptoms are sub dermal lesions in the head or neck or painless unilateral inflammation of cervical lymph nodes [1] . The disease is characterized by a triad of painless subcutaneous masses in the head or neck region, blood and tissue eosinophilia, and markedly elevated serum immunoglobulin. The first known report of Kimura’s disease was from China in 1937 [2] . It first received its name in 1948 when Kimura and others noted a change in the surrounding blood vessels and referred to it as “unusual granulation combined with hyperplastic changes in lymphoid tissue [3] . The cause of Kimura’s disease remains unknown. Reasons like an allergic reaction or an alteration of immune regulation are suspected. Other theories like persistent antigenic stimulation following arthropod bites and parasitic or candidal infection have also been proposed. To date, none of these theories have been substantiated. The pathophysiology of Kimura’s disease remains unknown, although an allergic reaction, trauma, and an autoimmune process have all been implicated as the possible cause. On histopathology the disease is manifested by an abnormal proliferation of lymphoid follicles and vascular endothelium. Peripheral eosinophilia and the presence of eosinophils in the inflammatory infiltrate suggest that Kimura’s disease may be a hypersensitivity reaction. Some evidence has indicated that TH2 lymphocytes may also play a role, but further investigation is needed [1] . Kimura’s disease is generally limited to the skin, lymph nodes, and salivary glands, but patients with Kimura’s disease and nephrotic syndrome have been reported. The basis of this possible association is unclear. Kimura’s disease is predominantly seen in males of Asian descent. The disease has rarely been reported in the United States [4] . Observation is acceptable if the lesions are neither symptomatic nor disfiguring. Radiotherapy has been used to treat recurrent or persistent lesions. However, considering the benign nature of this disease, radiation should be considered only in cases of recurrent, disfiguring lesions. Surgery has been considered as the mainstay of therapy. However, recurrence after surgery is common [5] .
2. Case Report
A 14 years old male came to SGRD Hospital Amritsar with history of recurrent neck swelling just behind the angle of mandible. Spherical, compressible, non tender swelling was approximately 5 - 6 cm in size (Figure 1). Patient was already operated at some other centre and again developed the same problem within few days after surgery. He had no previous records. FNAC was done showing Lymphoid nodules with discrete germinal centers occupying an area extending from the reticular dermis to the fascia and muscle. A marked eosinophilic infiltrate were present. Centrally, thick-walled vessels were present with hobnail endothelial cells. Immunohistochemical reports also demonstrated the presence of plasmacytoid dendritic cells in a lesion of Kimura’s disease. CT reports showed ill-defined, enhancing lesions behind angle of mandible, with associated lymphadenopathy (Figure 2). Routine blood investigations done. Renal function test were normal. Only absolute eosinophil count was raised.
Patient was treated with intraleisonal corticosteroid initially followed by oral methylprednisolone for period of 2 months along with antihistaminic. Swelling decreased in size gradually.

Figure 1. An operated case of Kimura’s disease presented with recurrence.
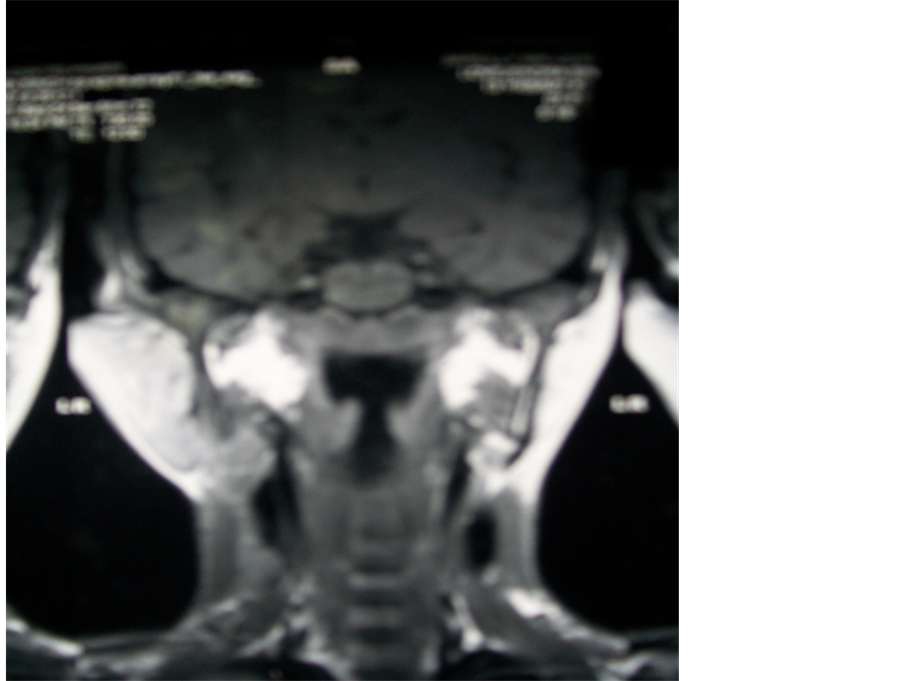
Figure 2. Computed tomographic (image of patient showing swelling upper part of neck).
3. Discussion
Kimura’s disease is a chronic inflammatory disorder of unknown etiology that most commonly presents as painless lymphadenopathy or subcutaneous masses in the head or neck region, especially in the parotid and submandibular regions [2] . These lesions are associated with occasional pruritus of the overlying skin. Renal disease, nephrotic syndrome in particular, is present in up to 20% of patients with Kimura’s disease. Kimura’s disease can lead to disfigurement secondary to the growth of untreated lesions. Additionally, recurrence after treatment is well described. Controversy has existed in the literature regarding whether Kimura’s disease and angiolymphoid hyperplasia with eosinophilia (ALHE) are the same entity. Some authors believe that Kimura’s disease represents a chronic, deeper form of ALHE; however, most recent papers distinguish the 2 on the basis of clinical and histopathologic characteristics [6] . The pathophysiology of Kimura’s disease remains unknown. It has been hypothesized that an infection or toxin may trigger an autoimmune phenomenon or lead to a type I (immunoglobulin E [IgE]-mediated) hypersensitivity reaction. Some evidence has suggested a predominance of TH2 cells which produce eosinophilic cytokines, including interleukin [IL]-4 and IL-5) in patients with Kimura’s disease. Additional studies have shown elevated granulocyte macrophage-stimulating factor (GM-CSF), tumor necrosis factor-a (TNF-a), soluble IL-2 receptor (sIL-2R), IL-5, IL-4, and IL-13. These findings may help lay the groundwork for elucidating the underlying pathophysiology of Kimura’s disease [7] [8] .
Kimura’s disease has rarely been reported in the United States. The exact prevalence of Kimura’s disease is not known. Most cases of this rare disease are reported in East and Southeast Asia, with a small number of cases reported in Europe [9] . Males are affected by Kimura’s disease more commonly than females, with a 3.5:1 to 9:1 male-to-female ratio [10] . Kimura disease is usually seen in young adults during the third decade of life, with the median age being 28 - 32 years [11] -[13] .
Kimura’s disease typically presents as a painless mass or masses in the head and neck region, with occasional pruritus of the overlying skin [14] . Patients typically present with nontender subcutaneous nodules and masses in the head and neck, especially in the parotid and submandibular regions. These lesions are typically associated with lymphadenopathy. Less frequently, the orbit (including the eyelids, conjunctiva, and lacrimal glands [15] , paranasal sinuses, epiglottis, tympanic membrane, and parapharyngeal space may be involved. The average diameter of lesions is 3 cm. Although Kimura’s disease mainly affects the head and neck, involvement of the extremities and inguinal lymph nodes has been reported. Kimura’s disease should be differentiated histologicaly with angiolymphoid Hyperplasia with Eosinophilia, Cylindroma, Dermatofibrosarcoma Protuberans, Kaposi Sarcoma. Nearly all patients with Kimura’s disease demonstrate peripheral eosinophilia and elevate levels of serum IgE. In one series, the number of eosinophils was closely correlated to the sizes of the neck masses. Blood urea nitrogen, creatinine, and urinary protein levels should be obtained to exclude concomitant renal dysfunction (especially nephrotic syndrome). Serum eosinophil cationic protein levels parallel the course of the disease.
The appearance of Kimura’s disease on imaging modalities, including CT scanning and MRI, is variable and is thought to be due, at least in part, to the variable degrees of vascular proliferation and fibrosis within individual lesions. One of the largest case series to date notes the characteristic findings to be multiple ill-defined, enhancing lesions around the parotid gland, with associated lymphadenopathy [16] . Lymphoid nodules with discrete germinal centers can occupy an area extending from the reticular dermis to the fascia and muscle. Histopathological reports show a marked eosinophilic infiltrate and centrally, thick-walled vessels are present with hobnail endothelial cells. Observation is acceptable if the Kimura’s disease lesions are neither symptomatic nor disfiguring. Oral corticosteroids are commonly used; however, the disease frequently recurs after cessation of therapy. Intralesional corticosteroids may be effective for localized disease. Cyclosporine has been reported to induce remission in patients with Kimura’s disease. A dose of 5 mg/kg/d was effective, but, in most cases, the lesions recurred upon cessation of therapy [17] . Intravenous immunoglobulin (IVIG) was used in one patient as a steroid-sparing agent, and he remained disease free more than 6 years after follow-up [18] . Oral pentoxifylline has been reported to be effective in one patient with Kimura’s disease; however, the lesions relapsed after discontinuation of therapy [19] . All trans-retinoic acid in combination with prednisone has resulted in remission of Kimura’s disease in one patient, and he remained disease free 12 months after discontinuation of all therapy. Imatinib may be an effective treatment for Kimura’s disease, based on advances in research for therapy in hyper eosinophilic syndrome, but further investigation is necessary. Photodynamic therapy has been used successfully in one patient who experienced recurrence of disease after initial surgical management. Radiotherapy has occasionally been used to treat recurrent or persistent Kimura’s disease lesions. A report by Hareyama et al. reported on the use of radiotherapy at dosages of 26 - 30 Gy; local control was achieved in 74% of lesions. Another study demonstrated that radiotherapy (20 - 45 Gy) was more effective than local excision and steroid treatment, with local response rates of 64.3% versus 22.2%, respectively. No adverse effects were observed during a mean follow-up period of 65 months [20] . However, considering the benign nature of Kimura’s disease, further investigation may be required, and caution using radiation outside of recurrent, disfiguring lesions is required.
References
- Lee, S. (2007) Kimura Disease. eMedicine. http://www.emedicine.com/derm/topic212.htm
- Kimm, H.T. and Szeto, C. (1937) Eosinophilic Hyperplastic Lymphogranuloma, Comparison with Mikulicz’s Disease. Proc Chin Med Soc, 329.
- Kimura, T., Yoshimura, S. and Ishikawa, E. (1948) On the Unusual Granulation Combined with Hyperplastic Changes of Lymphatic Tissues. Trans Soc Pathol Jpn, 37, 179-180.
- Ben-Chetrit, E., Amir, G. and Shalit, M. (2005) Cetirizine: An Effective Agent in Kimura’s Disease. Arthritis & Rheumatology, 53, 117-118. http://dx.doi.org/10.1002/art.20908
- http://emedicine.medscape.com/article/1098777-treatment
- Ramchandani, P.L., Sabesan, T. and Hussein, K. (2005) Angiolymphoid Hyperplasia with Eosinophilia Masquerading as Kimura Disease. British Journal of Oral and Maxillofacial Surgery, 43, 249-252. http://dx.doi.org/10.1016/j.bjoms.2004.11.023
- Ohta, N., Fukase, S., Suzuki, Y., Ito, T., Yoshitake, H. and Aoyagi, M. (2011) Increase of Th2 and Tc1 Cells in Patients with Kimura’s Disease. Auris Nasus Larynx, 38, 77-82. http://dx.doi.org/10.1016/j.anl.2010.03.011
- Katagiri, K., Itami, S., Hatano, Y., Yamaguchi, T. and Takayasu, S. (1997) In Vivo Expression of IL-4, IL-5, IL-13 and IFN-Gamma mRNAs in Peripheral Blood Mononuclear Cells and Effect of Cyclosporin A in a Patient with Kimura’s Disease. British Journal of Dermatology, 137, 972-977. http://dx.doi.org/10.1111/j.1365-2133.1997.tb01562.x
- Sun, Q.F., Xu, D.Z., Pan, S.H., et al. (2008) Kimura Disease: Review of the Literature. Internal Medicine Journal, 38, 668-672. http://dx.doi.org/10.1111/j.1445-5994.2008.01711.x
- Wang, D.Y., Mao, J.H., Zhang, Y., et al. (2009) Kimura Disease: A Case Report and Review of the Chinese Literature. Nephron Clinical Practice, 111, c55-c61. http://dx.doi.org/10.1159/000178980
- Kung, I.T., Gibson, J.B. and Bannatyne, P.M. (1984) Kimura’s Disease: A Clinico-Pathological Study of 21 Cases and Its Distinction from Angiolymphoid Hyperplasia with Eosinophilia. Pathology, 16, 39-44. http://dx.doi.org/10.3109/00313028409067909
- Thomas, J., Jayachandran, N.V., Chandrasekhara, P.K., Rajasekhar, L. and Narsimulu, G. (2008) Kimura’s Disease—An Unusual Cause of Lymphadenopathy in Children. Clinical Rheumatology, 27, 675-677. http://dx.doi.org/10.1007/s10067-007-0821-9
- Chen, H., Thompson, L.D., Aguilera, N.S. and Abbondanzo, S.L. (2004) Kimura Disease: A Clinicopathologic Study of 21 Cases. The American Journal of Surgical Pathology, 28, 505-513. http://dx.doi.org/10.1097/00000478-200404000-00010
- Rajpoot, D.K., Pahl, M. and Clark, J. (2000) Nephrotic Syndrome Associated with Kimura Disease. Pediatric Nephrology, 14, 486-488. http://dx.doi.org/10.1007/s004670050799
- Yoganathan, P., Meyer, D.R. and Farber, M.G. (2004) Bilateral Lacrimal Gland Involvement with Kimura Disease in an African American Male. Archives of Ophthalmology, 122, 917-919.
- Park, S.W., Kim, H.J., Sung, K.J., Lee, J.H. and Park, I.S. (2012) Kimura Disease: CT and MR Imaging Findings. American Journal of Neuroradiology, 33, 784-788.
- Kaneko, K., Aoki, M., Hattori, S., Sato, M. and Kawana, S. (1999) Successful Treatment of Kimura’s Disease with Cyclosporine. Journal of the American Academy of Dermatology, 41, 893-894. http://dx.doi.org/10.1016/S0190-9622(99)70354-3
- Hernandez-Bautista, V., Yamazaki-Nakashimada, M.A., Vazquez-Garcia, R., Stamatelos-Albarran, D., Carrasco-Daza, D. and Rodriguez-Lozano, A.L. (2011) Treatment of Kimura Disease with Intravenous Immunoglobulin. Pediatrics, 128, e1633-e1635.
- Hongcharu, W., Baldassano, M. and Taylor, C.R. (2000) Kimura’s Disease with Oral Ulcers: Response to Pentoxifylline. Journal of the American Academy of Dermatology, 43, 905-907. http://dx.doi.org/10.1067/mjd.2000.101931
- Hareyama, M., Oouchi, A., Nagakura, H., et al. (1998) Radiotherapy for Kimura’s Disease: The Optimum Dosage. International Journal of Radiation Oncology * Biology * Physics, 40, 647-651. http://dx.doi.org/10.1016/S0360-3016(97)00813-4