Open Journal of Nursing
Vol.04 No.13(2014), Article ID:52694,12 pages
10.4236/ojn.2014.413106
Thought Processes of Nurses in Nursing Assessment: Analysis of Nursing Problems and Patient Strengths, Patient Information
Kasumi Mikami1, Ryoko Tsuchiya2, Keiko Aizu1, Yoshiko Nishizawa1
1Hirosaki University Graduate School of Health Sciences, Hirosaki, Japan
2Hirosaki University School of Medicine & Hospital, Hirosaki, Japan
Email: k-mikami@cc.hirosaki-u.ac.jp
Academic Editor: Rie Chiba, Jichi Medical University, Japan
Copyright © 2014 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 14 November 2014; revised 12 December 2014; accepted 23 December 2014
ABSTRACT
Aims: The purpose of this study was to clarify the thought processes of nurses in performing nursing assessment. Methods: The participants comprised 20 nurses working in a surgery ward. Patient information on a case, including presenting illness, vital signs, and other findings from admission until 09:00 on the day after surgery, was shown to the participants. After reading the case report, the nurses presented their assessments. Based on these assessments, nursing problems, patient strengths, and patient information were identified. Nursing problems and patient strengths were described by various words and sentences, and were classified according to similar content. Results: The number of nursing problems ranged from 1 to 8 and patient strengths from 0 to 6 for each nurse. The mean number of nursing problems was 4.7 ± 1.8, and the mean number of patient strengths was 2.2 ± 1.4. The main nursing problems were respiratory complications, postoperative wound pain, and anxiety, and the main patient strength was family cooperation. Patient information as evidence of respiratory complications included history of smoking, chest radiography results, postoperative vital signs, sputum color and properties. Patient information as evidence of postoperative wound pain included complaints of pain, epidural anesthesia, use of patient-controlled anesthesia and its effect. Patient information indicating family cooperation included family structure, preoperative visits by family, and presence of family while providing informed consent. Significant differences were seen in the number of nursing problems and patient strengths according to cognitive style. Conclusions: Postoperative complications were the nursing problems most commonly extracted by nurses. To clarify nursing problems and patient strengths, the nurses made assessments on the basis of information such as patient complaints, vital signs, and test results. However, extracted nursing problems and patient strengths were diverse, suggesting that nursing problems and patient strengths as determined by nurses differed between individual nurses.
Keywords:
Nursing Assessment, Thought Process, Patients, Nursing Problems, Patient Strength

1. Introduction
Nurses provide appropriate nursing care to patients by implementing the nursing process. The nursing process is a way to provide systematic and organized nursing care for individuals or groups. The nursing process is a series of steps for information gathering, nursing assessment, nursing diagnosis, nursing plan, implementation, and evaluation. These steps are repeated to provide nursing care. The nursing process was proposed by Yura and Walsh [1] in 1967, and expanded rapidly.
Nursing assessment consists of gathering and analyzing patient information, and identifying nursing problems and patient strengths. Alfalo [2] stated that it was necessary that nursing assessment was accurate and comprehensive, as nursing assessment formed the basis for evaluating patients’ care needs. Therefore, nursing assessment is very important in order to clarify the needs of patients. In short hospitalizations and in perioperative patients, physical changes produced by operative stress occur very rapidly, requiring nurses to assess the patients as quickly as possible. Currently, Japan is a “super-aging society,” and nursing care will be provided more than ever, not only in the medical setting but also in the home or the community. The role of nurses is comprehensive for patients’ well-being. Since nurses are required to make judgments depending on the situation, such as for patients at risk of illness or treatment complications, further improvement in nurses’ proficiency in nursing assessment is essential. Clarification of the thought processes in nursing assessment will lead to advancing nurses’ assessment capability.
Prior studies have clarified through qualitative analysis how nurses carry out assessment of pain [3] , and have evaluated the methods nurses use to collect and apply initial information [4] . In addition, many studies have asked nurses to remember certain nursing episodes, and have interviewed nurses using a method of asking the nurses to think aloud regarding how they were thinking during those episodes [5] [6] . However, there have been few studies that clarify the characteristics of the thought processes of nurses while they make assessments using a great variety of patient information.
Nursing assessment is problem-solving process. Problem-solving encodes various items of information and is considered to be the information-processing approach for the interpretation of information. However, it is difficult to really observe the mechanism of information processing. It is said that the thinking process can be inferred from examining the input information and the output results [7] . Thus, the purpose of the present study was to consider the mechanism of information processing (with patient information as the input information, and nursing problems and patient strengths as the output results), and conjecture the thought processes of nurses and clarify the characteristics of nurses’ thinking.
Additionally, the present study focuses attention on cognitive style as a factor that influences nursing assessment. Cognitive style is defined as information processing and the personal coherence method to systematize the information. It is said that the information processing style is the way that an individual accepts and processes information in a situation where the individual needs to use perception and memory and thinking [8] . Nurses must grasp the state of a changing patient instantly and develop a care plan; the present study therefore ex- amines the “reflectivity” and “impulsivity” cognitive styles, which produce individual differences in cognitive tempo.
The present study uses a “paper patient” for the nursing assessment carried out by the participants. The paper patient was created from the information of a real patient and family. Use of a paper patient allows ample time to gain understanding of the complicated causation in the case and to develop problem-solving ability and subjects can imagine a patient background easily [9] . Use of a paper patient avoids ethical considerations that would be present in using a real patient for the study.
The purpose of this study was to clarify characteristics of the thought processes during the nursing assessment function of nurses, by clarifying how nurses make nursing diagnoses and identify nursing problems and patient strengths from perioperative patient information.
2. Methods
2.1. Sample
The participants comprised 20 nurses working in a surgery ward of the Prefecture General Hospital.
2.2. Data Collection
A questionnaire on age, sex, years of nursing experience, and similar questions, was distributed to the 20 nurses who participated in this study. This study used the scale of cognitive reflectivity-impulsivity to determine cognitive style [10] . This scale is constructed from 10 items. The Cronbach’s coefficient alpha is 0.767 to 0.842, and retest reliability is r = 0.827; therefore, the reliability of this scale has been already determined. This scale classifies cognitive style into reflectivity or impulsivity to calculate it with the median from the total scale score. A score lower than the median is classed as “impulsivity” and a score higher than the median is classed as “reflectivity.” We conducted a questionnaire on nursing assessment with the use of one paper patient case. Patient information on the case, including presenting illness, vital signs, sex, family constitution and other findings from admission until 09:00 on the day after surgery, was shown to the participants. The patient was a 58-year-old male with diabetes and rectal cancer, and was hospitalized to undergo surgery. The prevalence rate of colon cancer in Japan is the second highest after stomach cancer [11] . The patient made good progress postoperatively, but because he suffered from diabetes, the nurses needed to think about his condition. Preparation of this case was supervised by two researchers who specialize in perioperative nursing. Table 1 provides the details of this case. After explaining the purpose of this study to the director of nursing at the participating hospital, and obtaining the director’s consent, we were introduced to the nurses selected for the study. First, we carried out the questionnaire survey about the nurses’ profiles. Second, we conducted our investigation regarding the assessment. We explained to each nurse that the nurse should think about the case as though the nurse was the primary nurse of this paper patient, and to make the nursing assessment from the patient information provided. We asked each nurse, “What are the nursing problems and the patient strengths that you identify in this case?” and “Based on which items in the patient information did you identify the nursing problems and the patient strengths?”
2.3. Data Analysis
The patient information of the case was summarized plainly. The descriptions of the nursing problems and the patient strengths were classified into related items; this was confirmed by a number of researchers. The patient information was confirmed in detail according to the nursing problems and the patient strengths. The data were analyzed with the use of an un-paired t-test and a paired t-test to compare years of nursing experience and years of surgical nursing experience, and so on. Data analysis was performed using the Statistical Package for Social Science 22.0 for Windows. The level of significance used was p < 0.05.
2.4. Ethical Considerations
The Ethics Committee at Hirosaki University Graduate School of Medicine gave ethical approval, and the study was registered. We explained to the participants the purpose of the study and its method, and assured the subjects that participation was voluntary.
3. Results
3.1. Participant Characteristics
Table 2 shows the participant characteristics. The average age of the nurses was 29.5 ± 6.07 years, and there were 3 males and 17 females. The average number of years of nursing experience was 7.9 ± 6.40, and the number of years of working in surgical nursing was 5.1 ± 4.53. The most common nursing modality was primary nursing. Cognitive style included 11 participants with the reflective cognitive style and 9 participants having the impulsive cognitive style.
3.2. Nursing Problems
The number of nursing problems identified by individual nurses ranged from 1 to 8; the mean number of nursing
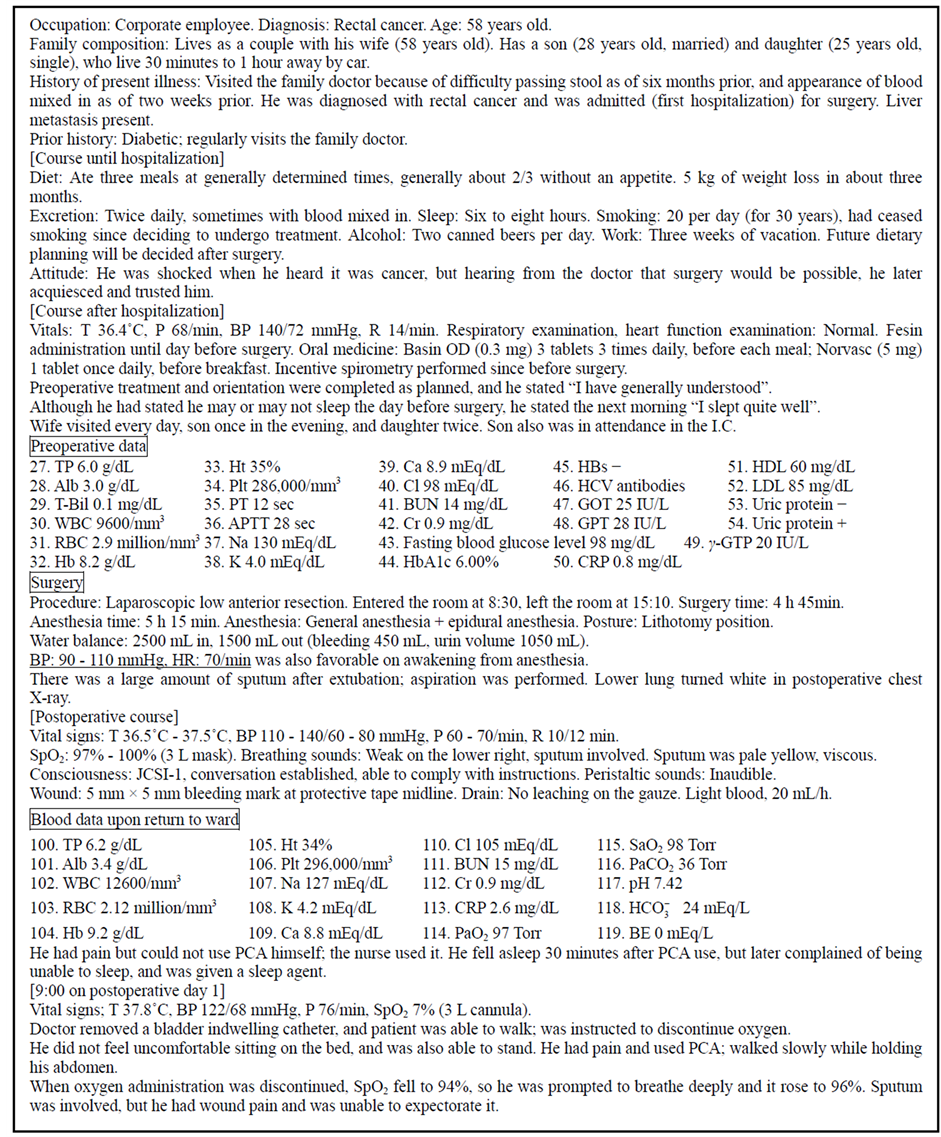
Table 1. The details of this case.
problems was 4.7 ± 1.82. The total number of nursing problems identified was 93, and was categorized into 24 kinds of problems. The nurses categorized the nursing problems as follows: Respiratory complications 16, postoperative wound pain 14, anxiety 10, delayed wound healing and risk of postoperative wound infection 7, risk of falls 6, poorly controlled blood glucose and risk of infection 5. Three nurses answered difficulty expectorating sputum, under nutrition, and risk of impaired skin integrity; two nurses answered risk of injury, insomnia, and

Table 2. Participant characteristics.
recognition of disease; and one nurse answered anemia, economic issues, character, constipation, circulatory state, decreased quantity of meals, difficulty arising, risk of confusion, and impaired comfort. Table 3 shows the breakdown of respiratory complications, postoperative wound pain, and anxiety that more than 10 nurses identified. Respiratory complications consisted of “ineffective airway clearance, pneumonia”, “risk of respiratory complications” and so on. Postoperative wound pain encompassed acute pain, uncontrolled pain, and so on. Anxiety centered on anxiety about surgery, postoperative anxiety, and so on. “Potential” nursing problems were noted with the terms “risk of...” and “possibility of...”.
3.3. Patient Strengths
The number of patient strengths identified by individual nurses ranged from 0 to 6; the mean number of patient strengths was 2.2 ± 1.39. The total number of patient strengths was 44, and was categorized into 10 kinds. Nurses identified the patient strengths as follows: family cooperation 19, return to work 4, patient’s cognition and understanding about surgery, early rising, ability to perform self-care, preoperative physical evaluation 3,
Table 3. Breakdown of nursing problems identified by >10 nurses who answered questionnaire.
prospects for discharge and pain control 2, and sleep 1. Table 4 shows the breakdown of family cooperation that more than 10 nurses identified. Family cooperation consisted of “good relationship with family,” and “obtaining family’s cooperation” and so on. “Potential” patient strengths were noted with the terms “risk of...” and “possibility of...”.
3.4. Patient Information as Evidence
We found that more than half the nurses identified respiratory complications, postoperative wound pain and anxiety as nursing problems, and family cooperation as patient strengths. In Figures 1-4, the patient information
Table 4. Breakdown of family cooperation identified as a patient strength by >10 nurses who answered questionnaire.

Figure 1. Patient information (n) serving as the basis for pulmonary complications.

Figure 2. Patient information (n) serving as the basis for wound pain.

Figure 3. Patient information (n) serving as the basis for anxiety.

Figure 4. Patient information (n) serving as the basis of when family assistance was obtained.
noted by many descriptions is designated by larger arrows, and (number) indicates the number of nurses who answered. Figure 1 shows the items of patient information that served as evidence of respiratory complications. The items of patient information that served as evidence of respiratory complications included wound pain, difficulty expectorating sputum, amount of sputum after decannulation and suctioning, chest X-ray results, and so on. There was a great deal of information about sputum. Figure 2 shows items of patient information that served as evidence of wound pain. The items of patient information that served as evidence of wound pain were use of patient-controlled anesthesia, pain when arising, complaints of pain, and so on. There was a great deal of information about use of patient-controlled anesthesia and the presence or absence of pain. Figure 3 shows items of patient information that served as evidence of anxiety. Items of patient information that served as evidence of anxiety included state of the patient when obtaining informed consent, and after, state at bedtime the night before the operation day, presenting illness, whether it was the first hospitalization for the patient, and so on. The state of the patient and the patient’s reactions were considered items of patient information that served as evidence. Figure 4 shows items of patient information that served as evidence of family cooperation. Items of patient information that served as evidence of family cooperation were visit of wife and son or daughter, presence of family while patient provided informed consent, preoperative visits by family, family structure, family going to operating room with patient, and so on. There were many answers concerning visits by family and attention given to the patient by the family.
3.5. Comparison of Participant Characteristics
Table 5 shows findings that compare the nurses’ years of nursing experience and years of surgical nursing experience, cognitive style, and academic background, together with the number of patient information items, nursing problems, and patient strengths that the nurses identified. We classified the nurse years of experience and years of surgery experience as the 5 or less or 5 or more. Regarding the number of patient information items, nursing problems, and patient strengths, the differences between groups were not significant. “Potential” nursing problems and patient strengths were noted by the terms “risk of...” or “possibility of...” by the nurses according to the nurses’ characteristics. Nurses with the reflectivity cognitive style were more likely to use the term “potential” than nurses with the impulsivity cognitive style. We compared the number of patient information items, nursing problems and patient strengths, and potential type and actual type, according to each nurse characteristic item. Although the differences noted by nurses with under 5 years of nursing experience were insignificant, the number of nursing problems were more likely to be greater than the number of patient strengths in total (p < 0.05, p < 0.01). The number of potential type items were significantly greater than the number of actual type items in the responses of nurses with a university degree (p < 0.01), nurses with <5 years of nursing experience (p < 0.05), and the impulsivity cognitive type (p < 0.05).
Table 5. Comparison by nurse background mean ± SD.
4. Discussion
4.1. Descriptions of Nursing Problems and Patient Strengths
To clarify the thinking characteristics of nurses in making nursing assessments, i.e. identifying nursing problems and patient strengths, we distributed a questionnaire about a case of a paper patient, and asked the participants to identify the nursing problems and patient strengths of this case. The nursing problems that were identified were mostly respiratory complications, followed by wound pain, anxiety, delayed wound healing, and risk of postoperative wound infection. The nurses focused on helping the perioperative patient to have a smooth, safe, and comfortable postoperative course. In addition, it was important that the nurses help the patient to become independent and regain health. The patient used as the case in this study was an adult male with a diagnosis of colon cancer, who was admitted to the hospital for surgery. He was diabetic with a history of smoking, and had a hemoglobin level lower than the standard value. After surgery, he had a large amount of sputum. Based on these factors, it was thought that the nurses judged this patient to be at increased risk for respiratory complications, delayed wound healing, and postoperative wound infection.
In addition, many nurses identified wound pain as a nursing problem. Postoperative wound pain is one of the body’s protective reactions that occur because of damage from surgery, and an inflammatory reaction occurs. This causes various vital reactions; it is said that wound pain adversely affects the whole body [12] . It is therefore essential that patients have their wound pain alleviated. Comfort promotes healing after surgery. Therefore, the nurses judged wound pain as a nursing problem.
The nurses’ identification of the patient’s anxiety about surgery and the prognosis was confirmed as a nursing problem. The nursing diagnosis definition of anxiety [13] according to NANDA-I is a vague, uneasy feeling of discomfort or dread accompanied by an autonomic response. However, the study patient’s feelings did not include restlessness, increased tension, or increased pulse. Canobbio [14] has stated that nurses alleviate fears and concerns regarding changes in body image and lifestyle. The nurse senses the patient’s vague, uneasy feelings of discomfort, and it is necessary to intervene to reduce the feeling after surgery. Thus, the nurses judged anxiety to be a nursing problem.
Many nurses answered “family cooperation” as a patient strength. Patient strengths identified during nursing assessment can serve as resources for patients to manage problems that may be present [15] . Identifying patient strengths can help in solving nursing problems, resulting in a better state for the patient. The support of the family becomes the support of the preoperative and postoperative patient. Other patient strengths identified included “return to work” and “cognition about surgery”. This study patient was a 58-year-old man who was employed. It is thought that social rehabilitation includes returning to work; this would promote the patient’s recovery. In addition, how the patient views their own surgery affects their future lifestyle. It is thought that it becomes a patient strengths that a patient takes an operation precisely and positively.
In the present study, there were fewer patient strengths identified than nursing problems. Because it is supposed that nurses makes assessment mainly on the issue of nursing. Also, because the nursing process is the process of finding nursing solutions to patients’ problems, when the nurse evaluates patients using the available information, it is thought that the nurse thinks mainly about clarifying the nursing problems. Matsunami and others [4] have stated that when a nurse gathers information, the nurse has a purpose “to find a nursing diagnosis”; the nurse does not diversify views about the purpose and application of the information. This leads us to speculate that the nurse gathers information to clarify the nursing problems of the patient, and the nurse has less interest in the information regarding patient strengths, which are the good points of the patient. This is supported by our study, which did not identify a significant number of patient strengths.
4.2. Patient Information as Evidence
In the present study, to clarify which aspects of patient information were used when nurses identified nursing problems and patient problems, we requested evidence from the patient information for every nursing problem and patient strength. Patient information on which the assessment of respiratory complications was based included “difficulty expectorating sputum due to postoperative wound pain,” “large amount of sputum after decannulation,” “chest X-ray,” “decreased breath sounds: right inferior lobe,” “smoking history,” “sputum is light yellow and viscid,” and “postoperative vital signs.” Particular patient information items identified about sputum, such as its amount or properties, and physical assessments such as chest X-ray and breath sounds, were regarded by the nurses as evidence provided by patient information. Respiratory complications are a type of postsurgical complication that occur with equal frequency to postoperative bleeding and suture failure. Respiratory complications include atelectasis, pneumonia, pulmonary edema, and pulmonary embolus. Most nurses identified pneumonia as a nursing problem in the study patient, and identified ineffective airway clearance as a nursing diagnosis, according to the evidence. Cioffi et al. [16] reported that, in acute care settings, the nurses gather information on change in patient status via the respiratory status of the patient or the increase in the oxygen dose for SaO2 maintenance. In the acute phase, the patient’s respiratory state leads to early detection of abnormalities. The nurses gather information on the patient’s state from such items as breathing physical assessment and SpO2 levels; this suggests that nurses identify such conditions as nursing problems.
Patient information as evidence of postoperative wound pain included “use of PCA,” “use of PCA for pain during postoperative ambulation,” and “complaint of pain”; the nurses identified these items of patient information as evidence that the patient had pain. Additionally, nurses answered “difficulty in expectorating sputum due to postoperative wound pain,” “unusual gait after surgery,” “complained of insomnia, and received soporific” “effect after the PCA use,” and “epidural anesthesia”, as items of patient information about wound pain. In addition, basic information such as male sex and age was also included. Information such as male sex and age do not provide direct evidence of wound pain, but is construed as such by an experienced nurse. Iizuka [17] stated that nurses base the amount of pain as information to use in making clinical judgments during the early postoperative ambulation period; this information includes administration time of pain medicine and patient complaints. Nurses determine the characteristics of the pain via the operative procedure and the kind of pain. The present study found these same results.
Patient information as evidence of anxiety included “reaction to the informed consent process before surgery,” “going to bed at 23:00 hours the previous day,” “first hospitalization,” “presenting illness,” “concern about 3 weeks’ absence and future work,” and “reduction in appetite and amount of appetite”. The evidence for anxiety is not based on complaints about anxiety; rather, the nurses predicted anxiety from patients’ reactions, the patients’ bedtime, and from physical reactions such as reduced appetite. Also, the nurse identified nursing problems from changes in the patients’ living arrangements such as the first hospitalization and from patients’ social background with respect to their work.
Patient information as evidence of family cooperation included visitation and attendance of family members, such as “visitation of wife,” “visitation of son and daughter,” “presence of family while providing informed consent,” and “attendance of family after operation”. Most nurses noted the relationships of the family during the postoperative recovery and social rehabilitation period, and recognized the importance of family relationships. Kenney [18] stated that family-centered nursing views the family as a contextual background of the individual client, who is the focus of care. The patient’s key person understands the treatment policy and the patient’s condition, influences the patient's decision-making, and is an important person in supporting the patient, including during continuation of treatment. Evidence of family support and visitor information are very important for the nurse.
4.3. Comparison of Number of Patient Information Items, Nursing Problems, and Patient Strengths with Respect to Background of Nurse
We compared the number of nursing problems, patient strengths, and items of patient information with respect to years of nursing experience, years of surgery ward experience, cognitive style, and educational background. Benner [19] stated that the novice sees all information moment by moment; as the level of experience rises, the expert can catch more and more as a complete whole in which only certain parts are relevant. Additionally, the expert nurse has an intuitive grasp of each nursing situation and makes a judgment. In the present study, we expected to find differences in the number of nursing problems and patient strengths identified, and items of patient information proportional to years of nursing experience and years of surgery ward experience. However, our analyses showed no significant differences. Maggi [20] reported that although experienced and inexperienced nurses use clinical reasoning processes to make judgments and decisions about nursing care, the speed of the thinking process and outcome may differ. In addition, experienced nurses use patient-centered prototypes to undertake cognitive shortcuts during the thinking process, but also rely on schemata, experience and intuition. Corcoran [21] stated that a clinical judgment means to make a decision regarding patient care, and cognitive consideration and intuition are related. Clinical judgment is a thinking process used to judge what kind of nursing intervention would be appropriate, based on the knowledge or experience of the individual nurse relevant to the state of the patient or situation. The nurse is thought to make a clinical judgment about nursing care while making a clinical decision in the nursing process about nursing care. However, the case of the present study was not a situation in which judgment was required in order to immediately make a clinical decision. It is thought that the nurse refines the judged result and is able to perform the nursing assessment in greater detail. Gordon [15] stated that the nursing diagnosis process includes an analytic reasoning strategy and diagnostic strategy of intuition. Both the inexperienced novice, as well as the expert encountering an unfamiliar clinical problem, use analytic strategies. Defined as logical, critical, or rational thinking, an analytic strategy uses divergent thinking to generate alternative explanations for cues, and uses convergent thinking to focus the cue search [15] . On the other hand, the diagnostic strategy of intuition―defined as immediate insight without conscious deliberation or analysis―recognizes similarities in a situation, and uses past experiences for interpretation. The expert nurse frequently uses the analytic strategy when indicated. In fact, the nurse performs two thought processes for assessment: one, an analytic reasoning strategy, and the other, a diagnostic strategy of intuition. In these ways, it is thought that the nurse makes a judgment about the patient’s situation. The nurses of the present study chose necessary information about the case and interpreted and judged it, without any time limitation. This suggests that nurses sufficiently test a hypothesis, and might use an analytic reasoning strategy mainly to make a more accurate judgment.
Nursing problems and patient strengths that were identified were divided into potential types (as “risk of...” and “possibility of...”) and actual types, and compared according to years of nursing experience and cognitive style. Although the differences were not significant, nurses having the “impulsivity” cognitive style were more likely to better identify actual types than nurses having the “reflectivity” cognitive style. No significant differences were found in the number of patient information items for evidence, nursing problems, or patient strengths, but the “impulsivity” nurses were more likely to identify actual type nursing problems and patient strengths than the “reflectivity” nurses. This demonstrates that an “impulsivity” nurse is more likely to determine a nursing problem from patient information; it suggests that the “impulsivity” nurse judges when it is necessary to intervene for a nursing problem that has already occurred. The “impulsivity” nurse comes to a decision in some situations immediately [10] . The “impulsivity” nurse is good at holistic processing, and the “reflectivity” nurse is good at detailed partial processing [8] . We consider that the “impulsivity” type of nurse captures holistically the situation of the patient from limited information, and information processing is performed to determine the nursing problems. Nurses with academic backgrounds other than university were more likely to identify the actual type of nursing problems. Yamada and others [22] have stated that registered nurses possess higher intelligence and logical thinking than practical nurses. Nursing basic education fosters problem-solving ability. As a result, logical thinking ability and critical thinking ability demanded in the nursing process increase.
5. Limitation of This Study
This study investigated only 20 nurses and assessed only one patient as an example. Therefore, it is necessary to increase the participants of nurses and example patients to raise the reliability.
6. Conclusions
The present study distributed a questionnaire to 20 nurses to clarify the characteristics of nurses’ thought processes in nursing assessment using a case of a perioperative patient. The following results were obtained:
1) The nurses identified nursing problems during the preoperative period as respiratory complications, followed by wound pain, anxiety, delayed wound healing, and risk of postoperative wound infection. The patient information focused particularly on sputum and physical assessment; the nurses regarded these items of patient information as evidence.
2) The nurses identified patient strengths as family cooperation, return to work, cognition about the surgery, understanding of the patient, early rising, ability for self-health care, and preoperative physical evaluation.
3) Nurses whose cognitive style was characterized by impulsivity were more likely to better identify actual types of nursing problems and patient strengths than nurses whose cognitive style was characterized by reflectivity.
To identify nursing problems and patient strengths, the nurses made assessments on the basis of various types of information. More nursing problems were identified than patient strengths. It is suggested that this is influenced by the problem-solving ability of the nurses.
References
- Yura, H. and Walsh, M. (1984) The Nursing Process: Assessing, Planning, Implementing, Evaluating. In: With Its Translation Supervised by Ikuko Iwai, Mitsuko Ina, 3rd Edition, Igaku-Shoin Ltd., Tokyo.
- Alfalo-LeFevre, R. (2014) Applying Nursing Process: The Foundation for Clinical Reasoning. 8th Edition, Wolters Kluwer Health, Philadelphia.
- Kim, H.S., Schwariz-Barcott, D., Tracy, S.M., Fortin, J.D. and Sjöström, B. (2005) Strategies of Pain Assessment Used by Nurses on Surgical Units. Pain Management Nursing, 6, 3-9. http://www.sciencedirect.com/science/article/pii/S1524904204001596# http://dx.doi.org/10.1016/j.pmn.2004.12.001
- Matsunami, M., Hirose, C., Kojima, M., Hori, M., Kinoshita, E. and Nakagawa, C. (2003) Evaluation of Methods Used to Collect and Apply Initial Information. Journal of Japan Society of Nursing Diagnosis, 8, 42-50.
- Hoffman, K.A., Aitken, L.M. and Duffield, C. (2009) A Comparison of Novice and Expert Nurses’ Cue Collection during Clinical Decision-Making: Verbal Protocol Analysis. International Journal of Nursing Studies, 46, 1335-1344. http://www.sciencedirect.com/science/article/pii/S0020748909001266 http://dx.doi.org/10.1016/j.ijnurstu.2009.04.001
- Iitsuka, M., Kamota, R., Watanabe, Y. and Saitoh, K. (2011) Floor Nurses’ Clinical Judgments for Perioperative Patients. Bulletin of Fukushima School of Nursing, 13, 1-10. http://ir.fmu.ac.jp/dspace/bitstream/123456789/244/1/BullFukushimaSchNurs_13_p1.pdf
- Lachmanm, R., Lachman, J.L. and Butterfield, E.C. (1990) Cognitive Science & Information Processing. In: With Its Translation Supervised by Youji Hakoda, Koutarou Suzuki, Saiensu-Sha Co., Ltd., Tokyo.
- Yamazaki, A. (1994) Study on Scanning Stratagem about Reflectivity and Impulsivity Cognitive Style. Kitaooji-Syobo, Kyoto.
- Shigemi, S. (2004) Learning and Educating in Paper Patient. 28 Cases. Igaku-Shoin Ltd., Tokyo.
- Takigiki, K. and Sakamoto, A. (2011) A Scale of Reflectivity-Impulsivity Cognitive Style. In: Hori, H., Ed., Collection of Psychological Measurements, Saiensu-Sha Co., Ltd., Tokyo, 195-198.
- ganjoho.jp (2014) Cancer Statistics. http://ganjoho.jp/public/statistics/pub/statistics01.html
- Onishi, C. and Akimoto, N. (2014) Adult Nursing Science, the Operation Period Nursing Theory. 3rd Edition, Nouvelle Hirokawa, Tokyo.
- Herdman, T.H. (2012) NANDA International. In: Herdman, T.H., Ed., Nursing Diagnoses: Definitions & Classification, Wiley-Blackwell, Chichester.
- Canobbio, M.M. (2000) Mosby’s Handbook of Patient Teaching. Mosby, St. Louis.
- Gordon, M. (2008) Assess Notes Nursing Assessment & Diagnostic Reasoning. F.A. Davis Company Press, Philadelphia.
- Cioffi, J., Conwayt, R., Everist, L., Scott, J. and Senior, J. (2009) “Patients of Concern” to Nurses in Acute Care Settings: A Descriptive Study. Australian Critical Care, 22, 178-186. http://www.sciencedirect.com/science/article/pii/S1036731409001209# http://dx.doi.org/10.1016/j.aucc.2009.07.001
- Iizuka, M. (2011) Nurse’s Clinical Judgment of Patients Receiving Abdominal Surgery at the Time of Their Early Ambulation. Journal of Human Care Studies, 12, 9-21.
- Kenney, J.W. (1995) Assessment Data Collection of the Family Client. In: Christensen, P.J. and Kenny, J.W., Eds., Nursing Process: Application of Conceptual Models, Mosby, St. Louis, 78-99.
- Benner, P. (2001) From Novice to Expert Excellence and Power in Clinical Nursing Practice. Prentice Hall, Englewood Cliff.
- Banning, M. (2008) Clinical Reasoning and Its Application to Nursing: Concept and Research Studies. Nursing Education in Practice, 8, 177-183. http://www.sciencedirect.com/science/article/pii/S1471595307000595
- Corcoran, S.A. (1990) Basic Concept of Clinical Judgment in the Nursing. Nursing Research, 23, 3-12.
- Yamada, R., Izumi, K., Hiramatsu, T., Kato, M. and Shogenji, M. (2007) Investigation of Clinical Nurses’ Intuition Relationships between Hospital, Years of Experience and Nurses’ License. The Journal of the Japan Academy of Nursing Administration and Policies, 10, 40-47. http://janap.umin.ac.jp/mokuji/J1002/10000004.pdf#search='Investigation+of+Clinical+Nurses%E2%80%99+Intuition+Relationships+between+Hospital%2C+Years+of+Experience+and+Nurses%E2%80%99+License