World Journal of Cardiovascular Diseases
Vol.3 No.3(2013), Article ID:33366,3 pages DOI:10.4236/wjcd.2013.33050
On-pump coronary artery bypass in moyamoya disease: A case report
![]()
1Department of Cardiovasculary Surgery, Istanbul University Cardiology Institute, Istanbul, Turkey
2Department of Cardiovascular Surgery, Hospitalium Hospitals Camlica, Istanbul, Turkey
Email: onurgurer@gmail.com
Copyright © 2013 Ismail Haberal et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 25 March 2013; revised 2 May 2013; accepted 17 May 2013
Keywords: Cardiopulmonary Bypass; Coronary Artery Disease; Moyamoya Disease
ABSTRACT
A 54-year-old female with pre-existing idiopathic moyamoya disease developed chest pain with acute myocardial infarction. Coronary angiography detected occluded and stenotic lesions in the coronary arteries. Right coronary artery stenosis was treated by balloon angioplasty and stenting. Because of the restenosis, onpump cardiopulmonary bypass was performed. The operation was uneventful and no perioperative cerebral ischemic episode occurred. The conclusion is that on-pump cardiopulmonary bypass preserving intraoperative hemodynamic parameters at an optimal level is a safe procedure in a patient with moyamoya disease.
1. INTRODUCTION
First described in 1957, moyamoya describes a rare cerebral arteriopathy characterized by occlusive disease of the terminal internal carotid or proximal middle cerebral arteries and proliferation of lenticulostriate collaterals [1]. The steno-occlusive changes in moyamoya disease are believed to be confined to the intracranial arteries and rarely occur in the extracranial arteries, including only rare occurrences in the coronary arteries [2]. In the literature, extracranial vascular involvement has been reported mainly in the renal artery [3]. However, coronary artery involvement among patients with moyamoya disease (MMD) is extremely rare [2]. We report an elderly female having ischemic heart disease with MMD who was successfully treated by on-pump coronary artery bypass grafting (ACBG).
2. CASE REPORT
A 54-year-old female was admitted to our clinic with sudden-onset acute inferior myocardial infarction. Urgent coronary angiography, performed at our hospital, revealed triple vessel disease; total occlusion of the right coronary artery (RCA) and left anterior descending artery (LAD); and 70 - 80 percent stenosis of the circumflex obtuse marginal artery (CXOM).
RCA stenosis was treated by balloon angioplasty and stenting.
Upon the resumption of the patient’s angina within one month, coronary angiography was performed. Fifty to sixty percent stenosis within the stent was found. The patient was referred to us for CABG “Figure 1”. Her past medical history included left hemiparesis due to a stroke at age 48 years. She recuperated at an another institution following the diagnosis of MMD “Figure 2”.
This patient also suffered from hypertension and diabetes mellitus, though she was being treated successfully
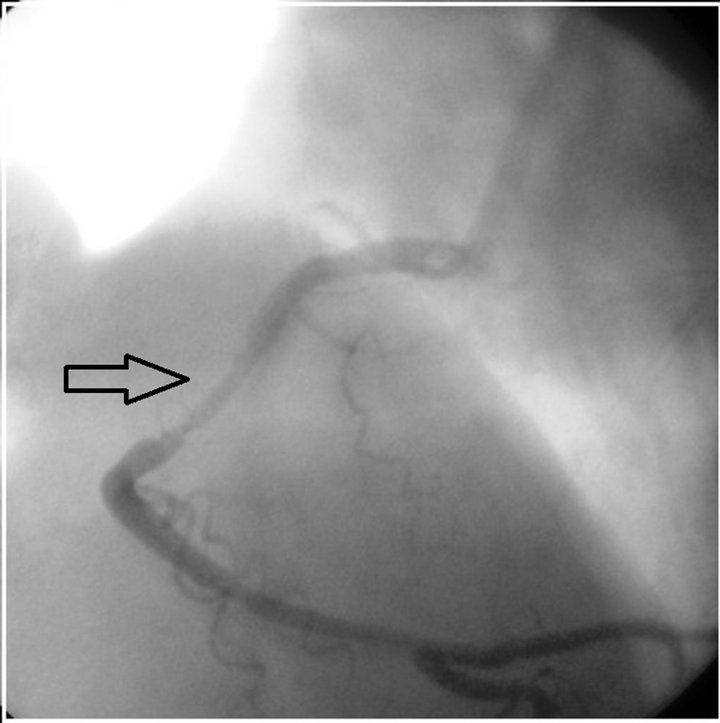
Figure 1. Stenosis within the stent.
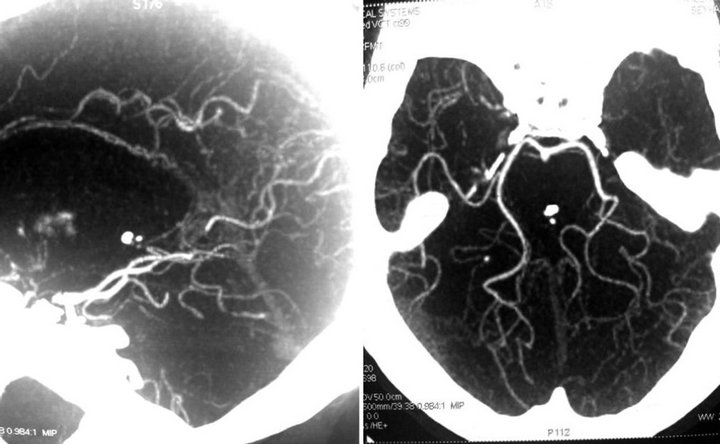
Figure 2. Magnetic resonance cerebral angiography indicated atherosclerotic vessels and collateral circulations (Suzuki grade II).
for both, measuring within normal ranges of blood pressure and glycosylated hemoglobin (HbA1c). Echocardiography revealed severe inferolateral, septal and apical hypokinesia. Ejection fraction was 40 percent.
Following routine preoperative preparation, patient underwent surgery. This included a median sternotomy. She received an infusion of four mg/kg heparin and cannulation of the ascending aorta and right atrium. Intermittent antegrade cold blood cardioplegia (with 15 mEq/L K+) or cold K+ cardioplegia accompanied by systemic hypothermia (28˚C - 30˚C) was performed. In order to avoid hypotension during induction of anesthesia, we interfered with vasopressor agents as necessary.
The patient received a left internal mammary graft to the left anterior descending artery, and a saphenous vein graft to the RCA and to the CXOM. Aortic cross-clamping time was 42 minutes; total cardiopulmonary bypass (CPB) time was 65 minutes. During the operation, mean arterial pressure and blood PaCO2 level were constantly maintained above 70 mmHg and 35 mmHg, respectively Hemoglobin value was maintained at level 8 mg/dl.
The operation was uneventful and no perioperative cerebral ischemic episode occurred. Inotropic support was applied after the end of CPB and continued during the two-day stay in an intensive care unit. Patient was discharged seven days postoperatively without problems.
3. DISCUSSION
MMD is usually confined to the intracranial cavity. Ischemic symptoms are more common in children than adults, due to the increased cerebral metabolic demand in childhood. The most common presentation is intracranial hemorrhage usually due to rupture of collateral vessels [4]. The intracranial hemorrhage is sometimes associated with the extracranial arterial system, such as the renal 3 or coronary artery [2]. Pathological analysis has revealed that affected vessels do not show arteriosclerotic or inflammatory changes leading to occlusion. Rather, vessel occlusion results from a combination of luminal thrombosis and hyperplasia of smooth-muscle cells. Although a combination of moyamoya and renovascular hypertension is well described [3], the association of coronary artery disease and moyamoya is rare [2]. The combination could be a chance occurrence. However, brain protection during CABG for patients with severe cerebrovascular disorder is vital. It is important to optimize physiological parameters, such as hemoglobin, hydration, and blood pressure, particularly around the time of surgery. CPB for patients with MMD is a high-risk procedure because of decreased cerebral perfusion pressure and non-pulsatile flow during CPB [5].
It is commonly believed that preserving autoregulation of CBP is the most important means of preventing brain ischemia in cases of cerebrovascular disorder such as MMD. Some techniques for CBP have been reported, including maintenance of the mean perfusion pressure above 70 mmH; a-stat blood gas management; and pulsatile flow with systolic pressure above 100 mmHg [6,7].
Off-pump CABG is an alternative, but during distal anastomosis, it might induce unexpected hemodynamic instability and impede cerebral circulation [5,7]. Some authors used an intra-aortic balloon pump as cerebral protection in a patient with moyamoya disease undergoing coronary artery bypass grafting [8,9].
In conclusion, we performed a successful on-pump triple vessel CABG on a patient with MMS. Therefore, it is possible to protect the brain from ischemia during onpump CABG in a patient with MMS, preserving intraoperative hemodynamic parameters at appropriate levels.
REFERENCES
- Takeuchi, K. and Shimizu, K. (1957) Hypoplasia of the bilateral internal carotid arteries. Brain Nerve, 9, 37-43.
- Komiyama, M., Nishikawa, M., Yasui, T., Otsuka, M. and Haze, K. (2001) Moyamoya disease and coronary artery disease: Case report. Neurologia Medico-Chirurgica, 41, 37-41. doi:10.2176/nmc.41.37
- Halley, S.E., White, W.B., Ramsby, G.R. and Voytovich, A.E. (1988) Renovascular hypertension in moyamoya syndrome. Therapeutic response to percutaneous transluminal angioplasty. American Journal of Hypertension, 1, 348-352. doi:10.1093/ajh/1.4.348
- Scott, R.M. and Smith, E.R. (2009) Moyamoya disease and moyamoya syndrome. The New England Journal of Medicine, 360, 1226-1237. doi:10.1056/NEJMra0804622
- Komiyama, M., Ishikawa, T., Takanashi, S. and Shimizu, Y. (2003) Minimal invasive direct coronary artery bypass in moyamoya disease. Interactive Cardio Vascular and Thoracic Surgery, 2, 65-67. doi:10.1016/S1569-9293(02)00100-7
- Johnsson, P., Algotsson, L., Ryding, E., Stahl, E. and Messeter, K. (1991) Cardiopulmonary perfusion and cerebral blood flow in bilateral carotid artery disease. The Annals of Thoracic Surgery, 51, 579-584. doi:10.1016/0003-4975(91)90315-H
- Tsukube, T., Okada, M., Ataka, K. And Ozaki, N. (2001) Coronary artery bypass grafting in a patient with brainstem ischemia. The Journal of Cardiovascular Surgery, 42, 349-351.
- Kashima, I., Inoue, Y. and Takahashi, R. (2008) The use of intra-aortic balloon pump as cerebral protection in a patient with moyamoya disease undergoing coronary artery bypass grafting. Interactive Cardio Vascular and Thoracic Surgery, 7, 522-523. doi:10.1510/icvts.2007.173682
- Okamoto, Y., Minakata, K. and Katsu, M. (2010) Offpump coronary artery bypass grafting supported by intraaortic balloon pumping in a patient with moyamoya disease. Kyobu Geka, 63, 1057-1060.