Open Journal of Blood Diseases Vol.05 No.01(2015), Article ID:54277,7
pages
10.4236/ojbd.2015.51001
The Efficacy and Safety of a 1.6 mg/m2 Increase in a Bortezomib Regimen
Sohsuke Meshitsuka, Kenshi Suzuki
Department of Hematology, Japanese Red Cross Medical Center, Tokyo, Japan
Email: sohmeshi@gmail.com
Copyright © 2015 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 21 January 2015; accepted 22 February 2015; published 27 February 2015
ABSTRACT
We conducted a single-center, prospective clinical trial in which a subcutaneous bortezomib (Bor) regimen [1.6 mg/m2 per month (BD 1.6 mg/m2 therapy)] was administered to 22 multiple myeloma patients. All patients had been treated sufficiently with once-monthly subcutaneous Bor injections (BD 1.3 mg/m2therapy). Of the 22 patients, 13 had IgG-, 2 had IgA-, and 7 had Bence-Jones protein (BJP)-type multiple myeloma. The observation period for therapeutic effect determination ranged from 84 to 412 days (median: 400 days). Therapeutic effects were investigated in 15 patients during the increase in Bor from 1.3 to 1.6 mg/m2, and none achieved complete remission (CR), very good partial remission (VGPR), or partial remission (PR). Given the small number of patients, a significant conclusion must be reached carefully. However, the chance of stronger success with increases in Bor is low for patients who have already undergone long-term 1.3 mg/m2 Bor treatment. Furthermore, non-hematological toxicity was seen in 12 of 22 patients, so increasing Bor to 1.6 mg/m2 should be considered carefully. However, the statuses of patients in this study suggest that once-monthly Bor could inhibit disease progression. In future we should investigate low-frequency Bor maintenance therapy.
Keywords:
Multiple Myeloma, Bortezomib, Maintenance Therapy

1. Introduction
Previously, we investigated the maximum tolerated dose and dose-limiting toxicity in 3 phase 1 trials involving a total of 123 patients with hematopoietic malignancies and various solid tumors [1] -[3] . Based on our findings, it was decided to recommend a dosing schedule in which 1.3 mg/m2 of bortezomib (Bor) is administered twice a week for 2 weeks, followed by a 10-day washout period. Bor at 1.3 mg/m2 is also usually given for multiple myeloma via subcutaneous injections administered once or twice weekly. Although several trials involving increased amounts of Bor have been conducted [4] -[6] , there have been no reports of long-term, once-monthly 1.3 mg/m2 of Bor administration as maintenance therapy. Moreover, we could find no examples in the literature that evaluated the efficacy and safety of increasing the Bor dose to 1.6 mg/m2 in such patients. Moreover, to date there have been no reports in which subcutaneous Bor injections were administered at a once-monthly dosage of 1.6 mg/m2.
Bor therapy, which can offer equivalent therapeutic efficacy while reducing the adverse event frequency, is administered by a subcutaneous injection from an intravenous infusion; non-inferiority studies of subcutaneous Bor injections also exist [7] . However, the blood concentration of Bor at the time of subcutaneous administration is known to have a lower peak value than that during intravenous administration [8] [9] ; considering the fact that a larger dosage may be more appropriate when subcutaneously injecting Bor roughly once monthly as maintenance therapy, we conducted this clinical trial to investigate the optimum Bor dosage for maintenance therapy.
2. Materials and Methods
This clinical trial was a single-center, non-randomized, prospective study. The main endpoint was safety and the secondary endpoint was therapeutic efficacy. Twenty-two patients with multiple myeloma who were already receiving BD 1.3 mg/m2 therapy were administered BD 1.6 mg/m2 therapy (Table 1). Of the 22 patients, 13 had IgG-, 2 had IgA-type, and 7 had Bence-Jones protein (BJP)-type multiple myeloma. The median age was 68.5 years (range: 44 - 90 years). The period during which Bor was administered at 1.3 mg/m2 at least once monthly as a pretreatment ranged from 8 to 52 months, with a median of 26.5 months. Table 2 uses different colors to indicate the treatment history of each patient. Bor-increase therapy specifically involved increasing Bor alone from 1.3 to 1.6 mg/m2, while retaining the same doses of concomitant drugs [melphalan (Mel), thalidomide (Tha), lenalidomide (Len), dexamethasone (Dex), and prednisolone (Psl)] used during the previous treatment.
The actual therapeutic approachesare as follows with 28 days comprising one cycle of treatment: Bor 1.6 mg/m2 subcutaneously administered on Day 1 and Dex 20 mg/body on Days 1 and 2 (BD), 13 patients; Bor 1.6 mg/m2 subcutaneously administered on Day 1, Dex 20 mg on Days 1 and 2, Mel 8 mg/body on Days 1-4, and Psl 20 mg/body on Days 1-4 (BMP), 2 patients; Bor 1.6 mg/m2 subcutaneously administered on Day 1, Dex 20 mg on Days 1 and 2, and Tha 50 mg/body on Days 1-28 (BDT50), 13 patients; Bor 1.6 mg/m2 subcutaneously administered on Day 1, Dex 20 mg on Days 1 and 2, and Tha 100 mg/body on Days 1-28 (BDT100), 2 patients; Bor 1.6 mg/m2 subcutaneously administered on Day 1, Dex 20 mg on Days 1 and 2, and Len 10 mg/body on Days 1-28 (BDL10), 1 patient; and Bor 1.6 mg/m2 subcutaneously administered on Day 1, Dex 20 mg on Days 1 and 2, and Len 15 mg/body on Days 1-28 (BDL15), 1 patient.
In all therapeutic approaches, Dex was administered at 20 mg/body on the same day as and the day after Bor administration. Psl, which is used in bone morphogenetic protein (BMP) therapy, was administered at 20 mg/day for roughly 4 days per month; however, appropriate increases or decreases were made at the attending physician’s discretion. Tha was administered every day at 50 or 100 mg/body without a washout period. Len was administered every day for 28 days at 10 or 15 mg/body. The therapeutic effect of increasing the Bor dose was only investigated in IgG- and IgA-type patients, and the evaluation period was the entire period during which the Bor dose was increased. Tha was later added to the regimens of 2 patients who underwent BMP therapy and 7 patients who underwent bortezomib and dexamethasone (BD) therapy; however, because 1 patient in the BMP therapy group and 4 patients in the BD therapy group had IgG- or IgA-type multiple myeloma, they were also subject to therapeutic evaluation.
Meanwhile, the safety of Bor-increase therapy was evaluated throughout the entire period, during which subcutaneous injections of Bor were administered once monthly at a dose of 1.6 mg/m2 to all IgG-, IgA-, and BJP- type patients. The observation period ranged from 28 to 435 days, with a median of 400 days.
The clinical research ethics committee of the institution with which the authors are affiliated approved this study following review (review reference number 431, clinical trial registration number 431). All patients received advance explanations of the purpose of this study and gave their written consent to participate.
2.1. Prophylactic Administration of Antibiotics
No acyclovir, sulfamethoxazole/trimetoprim combinations, or other antibiotics were administered.

Table 1. Patient characteristics.
ISS, International Staging System; DS, Durie-Salmon Staging System; BJP, Bence-Jones protein multiple myeloma; Bor, bortezomib; Mel, melphalan; Tha, thalidomide; Len, lenalidomide; Dex, dexamethasone; Psl, prednisolone; ND, no data; CR, complete response; VGPR, very good partial respose; PR, partial respose; SD, stable disease; PD, progressive disease; $Age at the initiation of increased bortezomib therapy; *ISS stage at diagnosis; ¶DS stage at diagnosis; # indicates continuation of the initial increased dose bortezomib therapy; BMP: Bor 1.6 mg/m2 on Day 1, Mel 8 mg/body on Days 1-4, Dex 20 mg/body on Days 1-2, and Psl 50 mg/body on Days 1-4; BD: Bor 1.6 mg/m2 on Day 1 and Dex 20 mg/body on Days 1-2; BDT50: Bor 1.6 mg/m2 on Day 1, Dex 20 mg/body on Days 1-2, and Tha 50 mg/body on Days 1-28; BDT100: Bor 1.6 mg/m2 on Day 1, Dex 20 mg/m2 on Days 1-2, and Tha 100 mg/body on Days 1-28; BDL10: Bor 1.6 mg/m2 on Day 1, Dex 20 mg/m2 on Days 1-2, and Len 10 mg/body on Days 1-28.
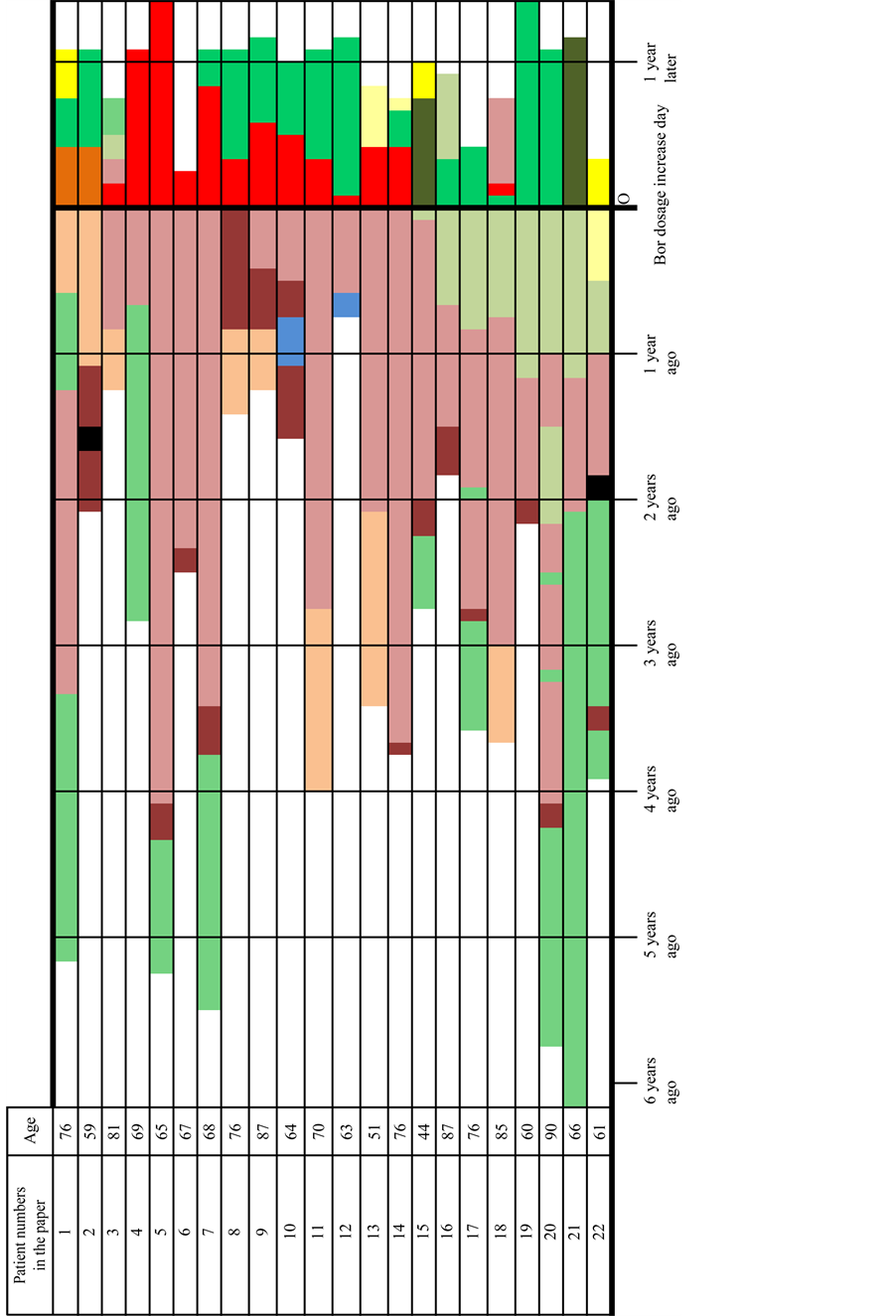
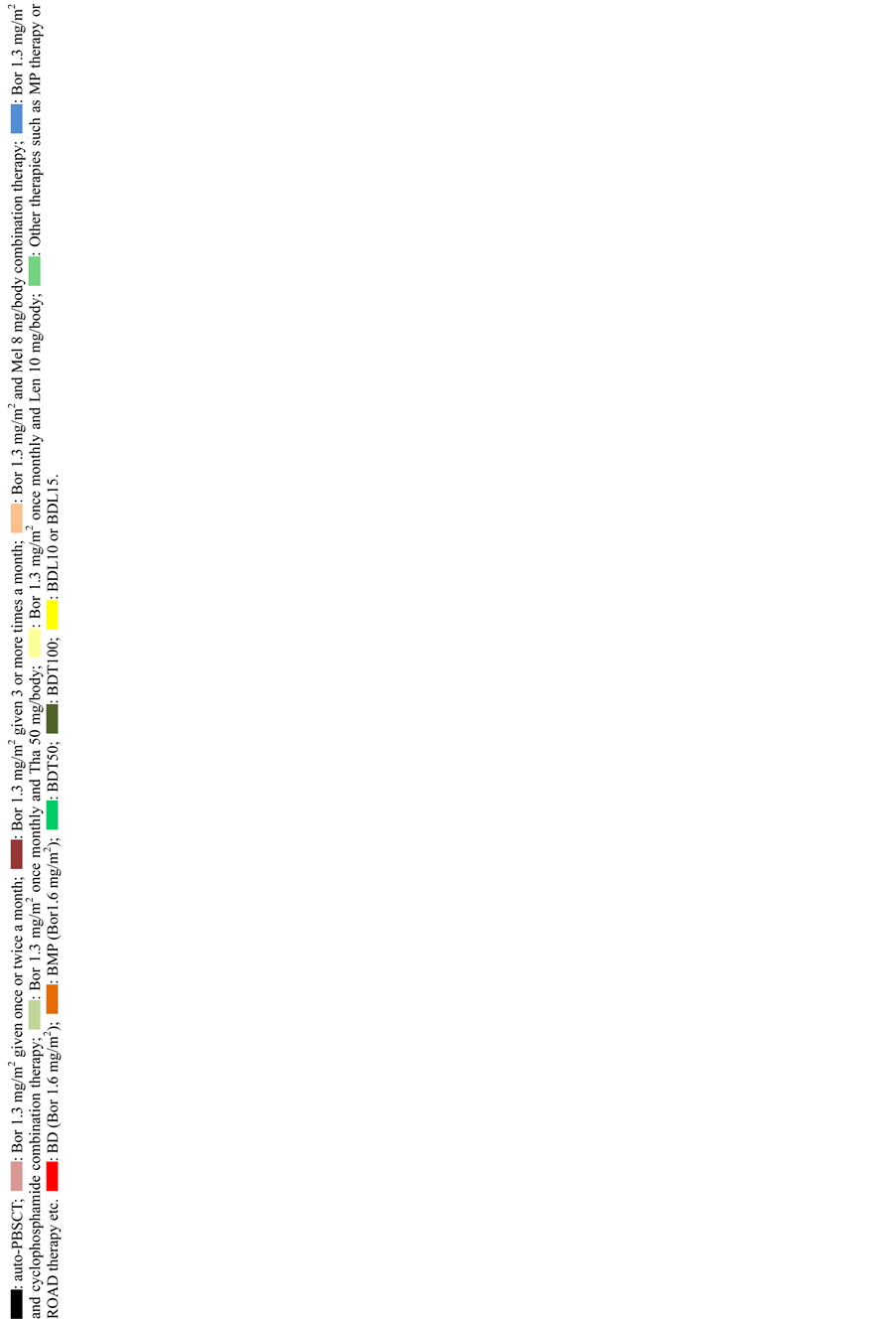
Table 2. Patient characteristics.
2.2. Adverse Events
Adverse events were described according to the Common Terminology Criteria for Adverse Events (CTCAE), version 4, published by United States department of health and human services National Institutes of Health and National Cancer Institute 2009.
2.3. Determining Therapeutic Efficacy
Judgments were made based on the criteria of the International Myeloma Working Group (IMWG).
3. Results
The therapeutic efficacy was determined for a total of 15 patients with IgG- and IgA-type multiple myeloma. The observation period ranged from 84 to 421 days, with a median of 400 days. No patients achieved complete remission (CR), very good partial remission (VGPR), or partial remission (PR) with increased Bor doses alone; 10 patients had a stable disease (SD) and 5 had a progressive disease (PD; Table 3). Nine patients subsequently changed to BDT50 therapy, and the therapeutic efficacy was determined for 5 of these patients (numbers 1, 7, 8, 11, and 12). Of these, 2 patients achieved PR (patient numbers 8 and 11), and the remaining patients had SD (2 patients; numbers 7 and 12) or PD (1 patient; number 1).
Meanwhile, adverse events were evaluated in all patients, including those with BJP-type multiple myeloma. This observation period ranged from 28 to 435 days, with a median of 400 days. Grades 3 and 4 hematological toxicity was observed for a total of 5 times in 3 patients, whereas Grades 3 and 4 non-hematological toxicity was observed for a total of 14 times in 12 of 22 patients (Table 4). No patients died. 8 of the 22 patients discontinued Bor at 1.6 mg/m2because of herpes zoster (1 patient; number 3), malaise (1 patient; number 6), interstitial pneu- monia (1 patient; number 13), and PD (3 patients; numbers 14, 17, and 22). Patients 16 and 18 were aged 87 and 85 years, respectively, and given the frequency of adverse events, they discontinued Bor at 1.6 mg/m2 owing to old age at the discretion of their attending physician.
4. Discussion
Although there are only a few existing reports of Bor administration at doses 1.3 mg/m2 or higher [4] -[6] , it was typical in earlier reports to administer Bor once weekly. We found no reports that directly compared Bor doses of 1.3 mg/m2 and 1.6 mg/m2, and few reports investigated the boosting effect of increasing the Bor dose in patients receiving long-term1.3 mg/m2 Bor therapy or once-monthly Bor administrations as maintenance therapy.
In actual clinical settings, frequent outpatient clinic visits by elderly patients incur significant costs for medical professionals, patients, and insurers, and future increases in the number of elderly individuals means that discussions regarding costs cannot be avoided. One vial of Bor currently contains 3 mg; however, the amount of wasted Bor is extremely large, given the Japanese physique. In fact, Bor was used a total of 2986 times at our hospital in the 1-year period beginning in July 2013, of which 2549 instances (approximately 85%) involved doses of less than 2.5 mg/body. In the present study, we investigated whether unnecessary waste could be reduced and illness could be improved by increasing the dosage of Bor per injection.
A higher frequency of infectious diseases, including herpes zoster, was observed compared to the past report [4] . This is, to some extent, since no prophylactic medication was administered in the present study. Although infections may be caused by not only the increase of Bor but also dexamethasone, there are few available literatures that indicate their precise doses of dexamethasonein the case of increased Bor regimen. If higher doses of Bor were to be used, at least prophylactic medication for herpes zoster should be provided. Only 1 of 22 patients exhibited a neurological disorder, which developed once Tha was added to the regimen. The reason for the very small number of patients in whom a neurological disorder was observed is that we selected patients with no major problems following previous long-term Bor treatment, which may have resulted in selection bias.
Although our sample size was too small to permit definitive conclusion, unfortunately the chance of greater success was low even when the Bor dosage administered to patients with a stable condition was increased following long-term Bor treatment at 1.3 mg/m2. However, a stable condition may indicate that a once-monthly injection of Bor is effective. Bor therapy at our hospital mostly involves once-monthly injections, with the exception of the induction therapy period, and the median length of the period during which Bor was administered 3 or more times per month was 2 months (0 - 10 months; Table 1). In other words, the period during which
Table 3. Treatment outcomes.
Bor, bortezomib; Tha, thalidomide; Len, 1 enalidomide; Dex, dexamethasone; Psl, prednisolone; ND, no data; SD, stable disease; PD, progressive disease; * indicates not to be included in the evaluation; - indicates no administration of increased dose bortezomib; BD: Bor 1.6 mg/m2 on Day 1 and Dex 20 mg/body on Days 1-2; BDT50: Bor 1.6 mg/m2 on Day 1, Dex 20 mg/body on Days 1-2, and Tha 50 mg/body on Days 1-28; BDL15: Bor 1.6 mg/m2 on Day 1, Dex 20 mg/m2 on Days 1-2, and Len 15 mg/body on Days 1-2; # indicates continuation of the initial increased dose bortezomib therapy; ## indicates continuation of the second increased dose bortezomib therapy.
Table 4. Adverse events.
- indicates that no Grades 3 and 4 adverse events were observed.
patients’ conditions were stable following low-frequency Bor injection-based therapy was above a median of 24.5 months (7 - 49 months) when counted from the pretreatment phase, suggesting the presence of patients whose conditions could be controlled with once-monthly Bor (Velcade) administration.
The statuses of the subjects in the present study suggest that at least once-monthly Bor injection could inhibit disease progression. In future, it will be necessary to clarify whether any patient’s condition could be stabilized with low-frequency therapy. We also hope for a more detailed investigation of the optimum low-frequency Bor maintenance therapy.
Conflict of Interest
The authors declare that they have no conflicts of interest.
References
- Aghajanian, C., Soignet, S., Dizon, D., Pien, C., Adams, J., Elliott, P., et al. (2002) A Phase I Trial of the Novel Proteasome Inhibitor PS341 in Advanced Solid Tumor Malignancies. Clinical Cancer Research, 8, 2505-2511.
- Orlowski, R., Mitchell, B., Shea, T., Baldwin, A., Stahl, S., Adams, J., et al. (2002) Phase I Trial of the Proteasome Inhibitor PS-341 in Patients with Refractory Hematologic Malignancies. Journal of Clinical Oncology, 20, 4420-4427. http://dx.doi.org/10.1200/JCO.2002.01.133
- Papandreou, C., Daliani, D., Nix, D., Yang, H., Madden, T., Wang, X., et al. (2004) Phase I Trial of the Proteasome Inhibitor Bortezomib in Patients with Advanced Solid Tumors with Observations in Androgen-Independent Prostate Cancer. Journal of Clinical Oncology, 22, 2108-2121. http://dx.doi.org/10.1200/JCO.2004.02.106
- Hainsworth, J., Spigel, D., Barton, J., Farley, C., Schreeder, M., Hon, J., et al. (2008) Weekly Treatment with Bortezomib for Patients with Recurrent or Refractory Multiple Myeloma. Cancer, 113, 765-771. http://dx.doi.org/10.1002/cncr.23606
- Craig, B., Reeder, C., Reece, D., Kukreti, V., Chen, C., Trudel, S., et al. (2010) Once- versus Twice-Weekly Bortezomib Induction Therapy with CyBorD in Newly Diagnosed Multiple Myeloma. Blood, 115, 3416-3417. http://dx.doi.org/10.1182/blood-2010-02-271676
- Wang, Y., Ai, L., Cui, G., Gowrea, B., Li, M. and Hu, Y. (2012) Once- versus Twice-Weekly Bortezomib Induction Therapy with Dexamethasone in Newly Diagnosed Multiple Myeloma. Journal of Huazhong University of Science and Technology, 32, 495-500. http://dx.doi.org/10.1007/s11596-012-0086-7
- Moreau, P., Pylypenko, H., Grosicki, S., Karamanesht, I., Leleu, X., Grishunina, M., et al. (2011) Subcutaneous versus Intravenous Administration of Bortezomib in Patients with Relapsed Multiple Myeloma. The Lancet Oncology, 12, 431-440. http://dx.doi.org/10.1016/S1470-2045(11)70081-X
- Moreau, P., Coiteux, V., Hulin, C., Leleu, X., Velde, H., Acharya, M., et al. (2008) Prospective Comparison of Subcutaneous versus Intravenous Administration of Bortezomib in Patients with Multiple Myeloma. Haematologica, 93, 1908-1991. http://dx.doi.org/10.3324/haematol.13285
- Moreau, P., Karamanesht, I., Domnikova, N., Kyselyova, M., Vilchevska, K., Doronin, V., et al. (2012) Pharmacokinetic, Pharmacodynamic and Covariate Analysis of Subcutaneous versus Intravenous Administration of Bortezomib in Patients with Relapsed Multiple Myeloma. Clinical Pharmacokinetics, 51, 823-829. http://dx.doi.org/10.1007/s40262-012-0010-0