Open Journal of Safety Science and Technology
Vol.3 No.4(2013), Article ID:40737,11 pages DOI:10.4236/ojsst.2013.34009
Non-Fatal Occupational Injuries and Safety Climate: A Cross-Sectional Study of Construction Building Workers in Mit-Ghamr City, Dakahlia Governorate, Egypt
Department of Community, Environmental and Occupational Medicine, Faculty of Medicine, Zagazig University, Zagazig City, Egypt
Email: reemabbasabbas@yahoo.com
Copyright © 2013 Reem Abbas Abbas et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received July 24, 2013; revised August 24, 2013; accepted August 31, 2013
Keywords: Occupational Injuries; Occupational Accidents; Construction Building Workers; Safety Climate; Risk Factors
ABSTRACT
Background: Construction is a dangerous industry, with high rates of fatal and non-fatal injuries. Although, safety climate has been linked with safety performance and work-related accidents, yet it is scarcely studied and considered in injury prevention programs in developing countries. So, the objectives of this study are to find out the magnitude, pattern and risk factors of non-fatal occupational injuries among a sample of construction building workers and to explore the level of safety climate and its relationship with occupational injuries. Methods: A cross-sectional study was conducted on 91 workers, who fulfilled the inclusion criteria, in 18 large construction sites in Mit-Ghamr city, Dakahlia Governorate. Data about socio-demographic and occupational characteristics, description of occupational injuries, and work-related and behavioral risk factors were collected using a structured questionnaire. Results: Occupational injuries in the past 12 months were reported by 46.2% of workers. The most common body parts injured were upper and lower limbs (31.0% and 26.2%). The majority of injuries were cuts/lacerations (30.9%) and contusions (28.6%). Falls (47.6%) and injuries by manual tools (23.8%) were the main causes of injuries. The majority of injured workers (90.5%) reported complete recovery after the most serious injury. The average of working days was lost per year due to occupational injuries (18.6 ± 7.8 days/year). None of the injured workers reported receiving sufficient first-aid treatment at worksite or filling an accident notification form. Extended working hours, poor safety climate, short duration of work, job dissatisfaction, young age, and job stress were significant risk factors of occupational injuries. Conclusion: Non-fatal occupational injuries are common among this sample of construction workers with significant relation to extended working hours and poor safety climate and other risk factors. So, it is important to build upon this research in order to help develop successful policies to prevent work-related injuries and promote safer work practices for construction building workers.
1. Introduction
Construction industry is both economically and socially important. It involves many other types of activities aside from the building process, such as painting, landscaping, electrical supply, telecommunications, plastering, and paving [1,2].
The construction sector in Egypt is a major contributor to the country’s economy and one of its fastest-growing sectors. It is fueled by the continuously increasing demand for housing and by the country’s large infrastructure projects [3]. It makes up at least 70% of casual wage workers in urban areas and constitutes the largest share of employment growth and absorbs many of the poor workers [4].
Construction industry is one of the most hazardous and accident prone occupations as reported by the International Labor Organization, which is because several potential hazards are present in the construction sites that can lead to serious injury or death [3]. Construction workers face a risk of fatal and non-fatal injuries higher than any other groups of workers [5]. Although countries differ substantially in their structural industrial distribution or level of occupational health and safety, the construction workers’ injuries are the major occupational injuries in many countries [6]. Moreover, the rate of death of workers is higher in construction industry than in any other industry [3].
Globally, 17% of all work-related fatalities are in the construction sector [7]. In Egypt, about 13% of workrelated deaths and 18% of occupational injuries were recorded among construction workers [8]. The number of reported occupational injuries in governmental, public and private sectors of the construction industry with more than 50 workers in Egypt was 790 in the year 2010 and 677 in the year 2011 [9]. Statistics showed that about 90% of the fatalities in two large construction companies in the USA and Egypt resulted from four major causes; falls from heights (33%), being struck by an object (22%), being caught in-between two objects (18%), and contact with an electric current (17%) [3]. Similar Egyptian study found that lower and upper limbs (35.3% and 32.9%, respectively) were the most injured body parts, mostly in the form of contusions (29.4%) and cuts (22.4%), followed by head and eye injuries (14.1%) [10].
Several researches show that the major causes of accidents are related to the unique nature of the construction industry, human behavior, difficult worksite conditions, and poor safety management [11]. The concept of safety climate attracts much attention across a broad number of industries and sectors [12]. Safety climate generally refers to workers’ perceptions regarding managements’ attitudes towards occupational safety and health. A recent hypothesis links safety climate with workers’ behavior at work. It is suggested that more favorable safety climate perceptions are related to safer behavior and consequently less occupational accidents happen [13].
In developing countries, safety consideration during different construction activities is not given a priority and the employment of safety measures during construction is considered a burden [14]. Although dramatic improvements have taken place in recent decades, the safety record in the construction industry continues to be one of the poorest [15]. Moreover, workers’ perceptions and experience in relation to occupational health and safety are scarcely considered in programs for the prevention of work-related injuries and diseases [13]. So, the main objectives of this study are; 1) to find out the magnitude, pattern and risk factors of non-fatal occupational injuries among a sample of construction building workers and 2) to explore the level of safety climate and its relationship with occupational injuries.
2. Subjects and Methods
2.1. Study Design and Setting
This cross-sectional study was conducted in 18 large construction sites in Mit-Ghamr city during the period from January to April 2013. Mit-Ghamr is a famous industrial overpopulated city in Dakahlia Governorate (Total population = 116,593) [16].
2.2. Sample Size Determination and Sampling Method
The estimated sample size was 107 workers. It was calculated using EPI-INFO program version 6 [17]; taking into account the total number of construction building workers in the 18 selected large construction sites (n = 1100 workers) and the prevalence of occupational injuries among construction workers from a previous study (44.7%) [10], and assuming 95% confidence interval and 80% power of the test. Workers were selected using simple random sampling technique. The selected workers were interviewed by the investigators, where they were recruited in the study according to the following inclusion criteria; working in the same construction company for at least 2 consecutive years, with no past history of chronic diseases or disability on joining the current job, and their body mass index is lower than 30 Kg/m2 [18]. Thus, 98 workers were invited by the investigators to an interview, where they were asked to give their consent after explaining the purpose and the steps of the study.
2.3. Ethical Issues
Proposal acceptance was obtained from the Research Ethics Committee of the Faculty of Medicine; Zagazig University. Moreover, informed consent was obtained from all participants after explaining the aim of the study and confidentiality of the information was assured.
2.4. Data Collection and Measures
Data were collected using a pre-tested and structured questionnaire that was translated into Arabic. It was based on those of other relevant studies [2,19-22]. The questionnaire focused on four main parts:
Part one: included socio-demographic and occupational data as: age, marital status, education, residence, job category, duration of work in years, working hours per week, and shift work. For the purpose of this study, extended working hours were referring to working more than 48 hours per week [23]. Moreover, a skilled worker was defined as any worker who has some special skill, knowledge, or ability in the work. A skilled worker may have attended a college/university or technical school or, may have learned skills on the job. An unskilled worker is a person lacking skill or technical training [24].
Part two: included description of the pattern of occupational injuries. At first, participants were asked about their involvement in an occupational accident in the past 12 months and if this accident was associated with injury or not. Then, they were also asked to describe their workrelated injuries according to the most common type (nature), causes, and anatomical location and body part injured. Moreover, data about injury management at worksite, working days lost, the outcome of the most serious injury, and filling an accident notification form were obtained.
Part three: Included information about common work-related determinants of injuries such as regular workplace supervision, machinery design and maintenance, and health and safety training.
Part four: Included a list of common behavioral risk factors such as using personal protective equipment, substance abuse, smoking, sleeping disturbance, job satisfaction, job stress, and safety climate (Appendix).
Job stress was measured using the workplace stress scale. It included five negative statements and three positive statements. Job stress was categorized according to the calculated score into; yes (16 to 40) and no (lower than or equal 15) [25].
Job satisfaction was measured using the generic job satisfaction scale. It is a valid and reliable scale that is short and easily administered in the workplace. It included ten statements. The degree of agreement ranged from 1 = strongly disagree to 5 = strongly agree, thus the total estimated score = 50. Job satisfaction was categorized according to the calculated score into; yes (32 - 50) and no (10 - 31) [26].
Items in the safety climate questionnaire included one general item and 10 specific items with a scale from 0 to 10 for each item. A safety climate index (SCI) was then calculated by adding accorded scores for each specific item (items 2 - 11). As these 10 items were each answered on a scale of 0 - 10, the SCI range was 0 - 100. For the purpose of this study, SCI was categorized into poor (SCI less than 50) and good (SCI equal or more than 50) [13].
2.5. Pilot Study
A pilot study was done on 4 workers before the main study and they were not included in the main survey. Some changes were done to the questionnaire following the pilot study to improve clarity and convenience.
2.6. Data Management
Data were coded and statistically analyzed using SPSS version 19 [27]. Comparison between group means was done using student’s t test and comparison between categorical variables was done by x2 test. Bivariate analysis was carried out to identify risk factors in terms of unadjusted odds ratios (OR) with their 95% confidence intervals (CIs). Subsequently, stepwise multiple logistic regression analysis was carried out to identify independent determinants whilst adjusting results by potential confounders. A P-value < 0.05 was considered statistically significant.
3. Results
Ninety one construction workers agreed to participate in the present study out of 94 workers who met the inclusion criteria, with a response rate of (96.8%). Respondents had an age range of (23 - 48 years) with a mean of (33.4 ± 8.6 years). The majority of them was from rural areas (65.9%) and was married (78.0%). Those with basic education constituted (43.9%); while illiterates constituted 23.1%, and those graduated from college/technical institutes constituted (33.0%). Most of the participants were unskilled workers (62.6%) and only (37.4%) were skilled workers. The average duration of work was (13.8 ± 6.5 years) (range 4 - 21 years). Their average working hours per week (48.2 ± 5.3) ranged from (42 - 54 hours/week). All participants were daytime workers with no shift work (Table 1).
Occupational injuries in the past 12 months were reported by 42 out of 91 workers (46.2%). The most com-
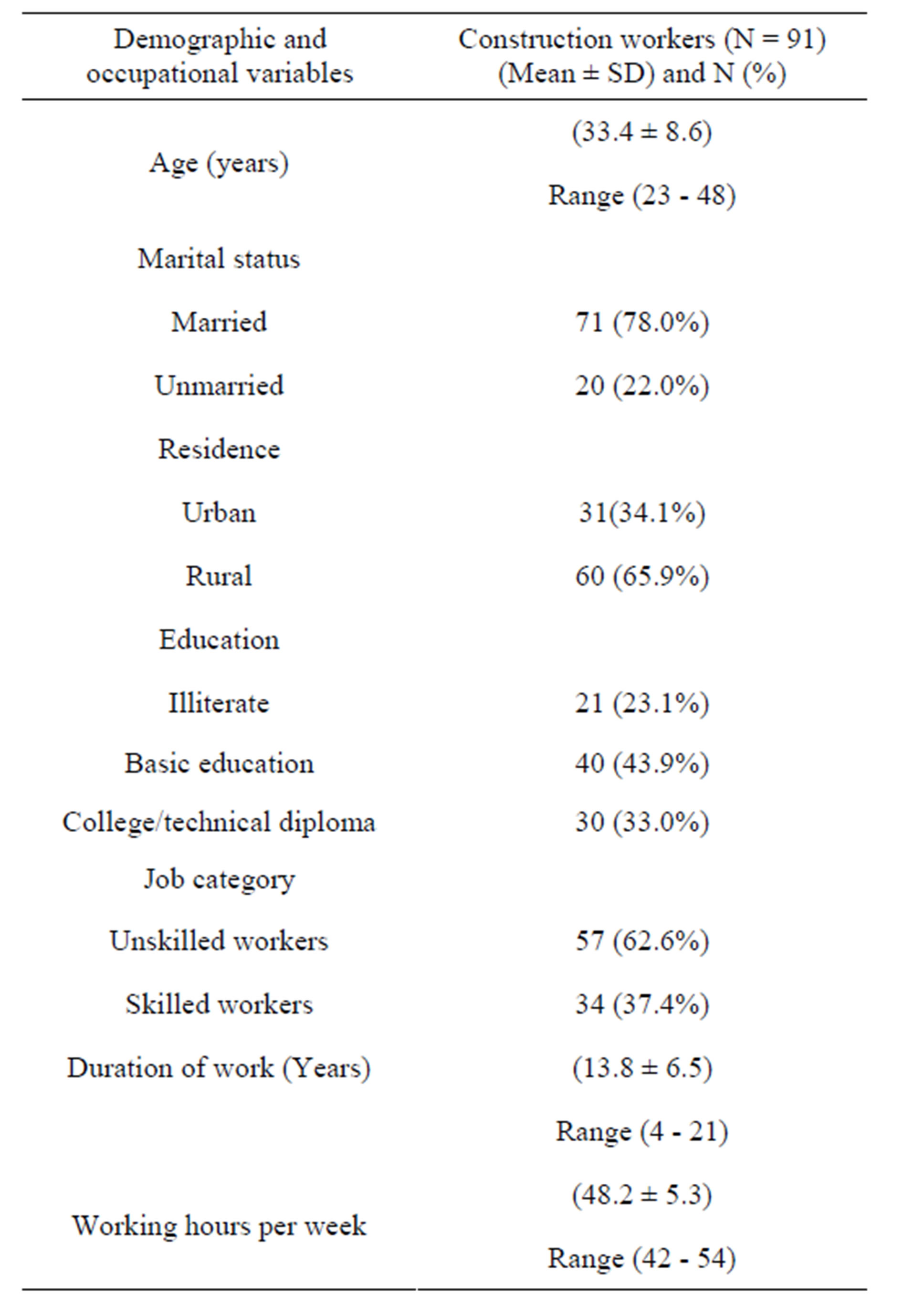
Table 1. Socio-demographic and occupational characteristics of construction workers.
mon body parts injured were upper and lower limbs (31.0% and 26.2%, respectively). The most common injuries were cuts and lacerations (30.9%), contusions (28.6%) sprains/strains/musculoskeletal pain and multiple injuries (14.3% for each). Falls (47.6%) and injuries by manual tools (23.8%) were the main causes of injuries. The vast majority of injured workers (90.5%) reported complete recovery after the most serious injury; while disability occurred in only (9.5%) of them. The average of working days lost per year due to occupational injuries was (18.6 ± 7.8 days/year) (range 7 - 31 days/year). None of the injured workers reported receiving sufficient firstaid treatment at worksite or filling an accident notification form (Table 2).
Bivariate analysis showed that young age (workers

Table 2. Pattern of occupational injuries among construction workers.
younger than 30 years old) and short working duration (less than 10 years) were significantly associated with occupational injuries. Extended working hours (more than 48 hours/week) and poor machinery design and maintenance were also significantly associated with occupational injuries among this sample of construction building workers (Table 3).
Moreover, sleeping disturbance, job dissatisfaction, job stress, and poor safety climate were significantly associated with occupational injuries (Table 4). Multiple logistic regression analysis of the significant risk factors showed that extended working hours, poor safety climate, short duration of work, job dissatisfaction, young age, and job stress were significant risk factors of occupational injuries. While, sleeping disturbance and poor machinery design and maintenance didn’t show significant association with occupational injuries among the studied sample of construction workers (Table 5).
The mean score level of the general item of safety climate was significantly higher among non-injured construction workers than that among injured workers (6.8 ± 1.7 Vs 3.2 ± 0.9) with a range of (3 - 8 Vs 1 - 6). Moreover, the mean score level of safety climate index (SCI) was significantly higher among non-injured workers than that among injured workers (69.6 ± 12.2 Vs 39.7 ± 11.3) with a range of (41 - 78 Vs 16 - 52) (Table 6).
4. Discussion
Nearly, 317 million accidents occur on the job annually most of them occurred in low and middle income countries; many of these resulting in extended absence from work or death. Every day, 6300 people die as a result of occupational accidents or work-related diseases. The human cost of this daily adversity is vast and the economic burden of poor occupational safety and health practices is estimated at 4% of global Gross Domestic Product each year [28]. Despite this, only 5% to 10% of the workforce in developing countries has access to some occupational health and safety services [29].
Construction is a dangerous industry with high rates of both fatal and non-fatal occupational injuries. Till now it continues to face serious challenges in safety and health despite the declining rates of accidents over time [2]. In a study of non-fatal occupational injuries among construction workers that was carried out in Kuwait, injured construction workers constituted more than half of the total number of occupationally injured workers, (57.1%, 61.99% and 54.2%) in the years 2003, 2004 and 2005, respectively. However, it should be noticed that countries vary substantially in the education and training background of their workers [30]. Moreover, construction workers are exposed to a wide variety of safety hazards, this exposure differs according to the job demands [2].
In the current study, occupational injuries in the past
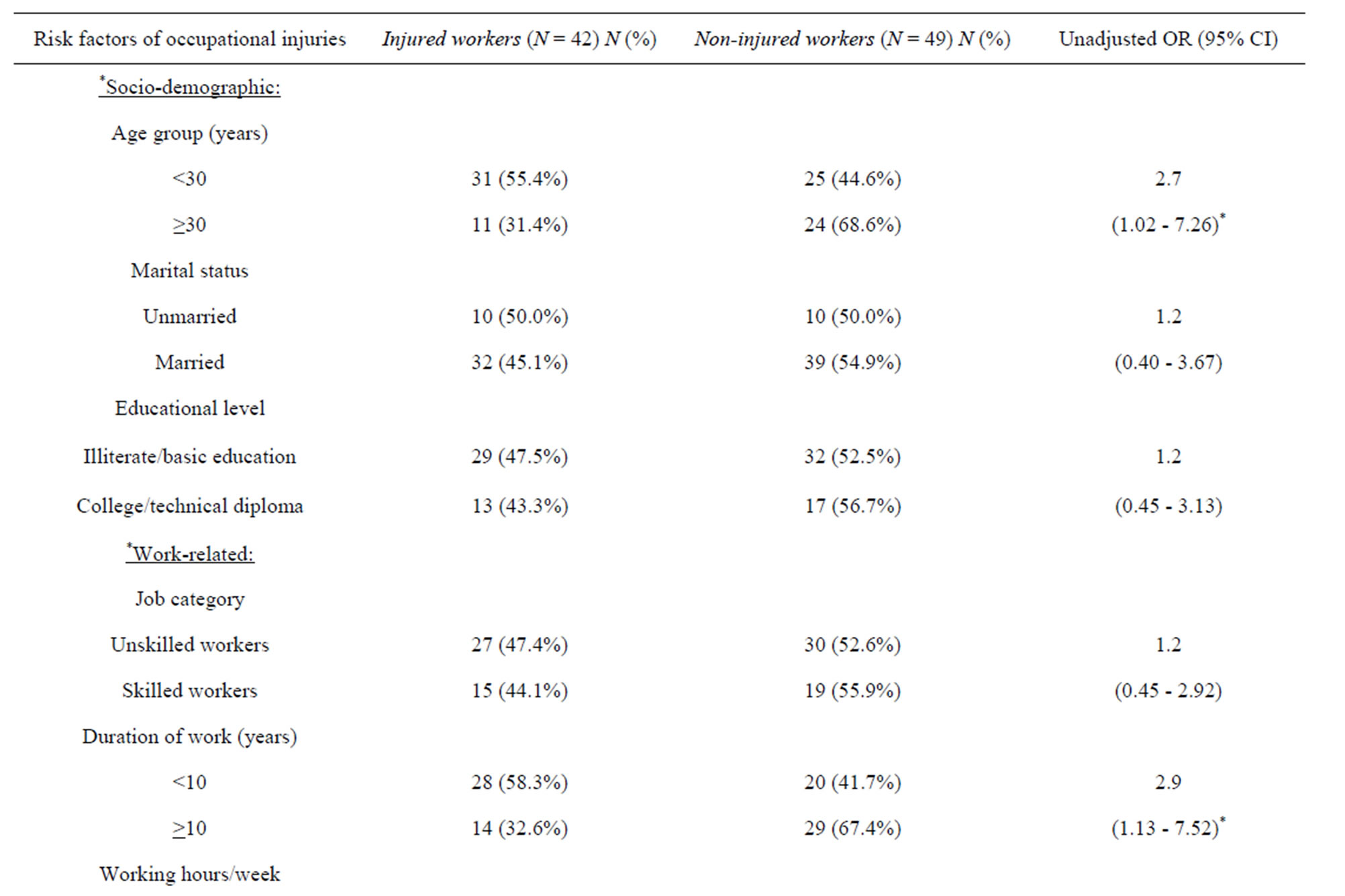
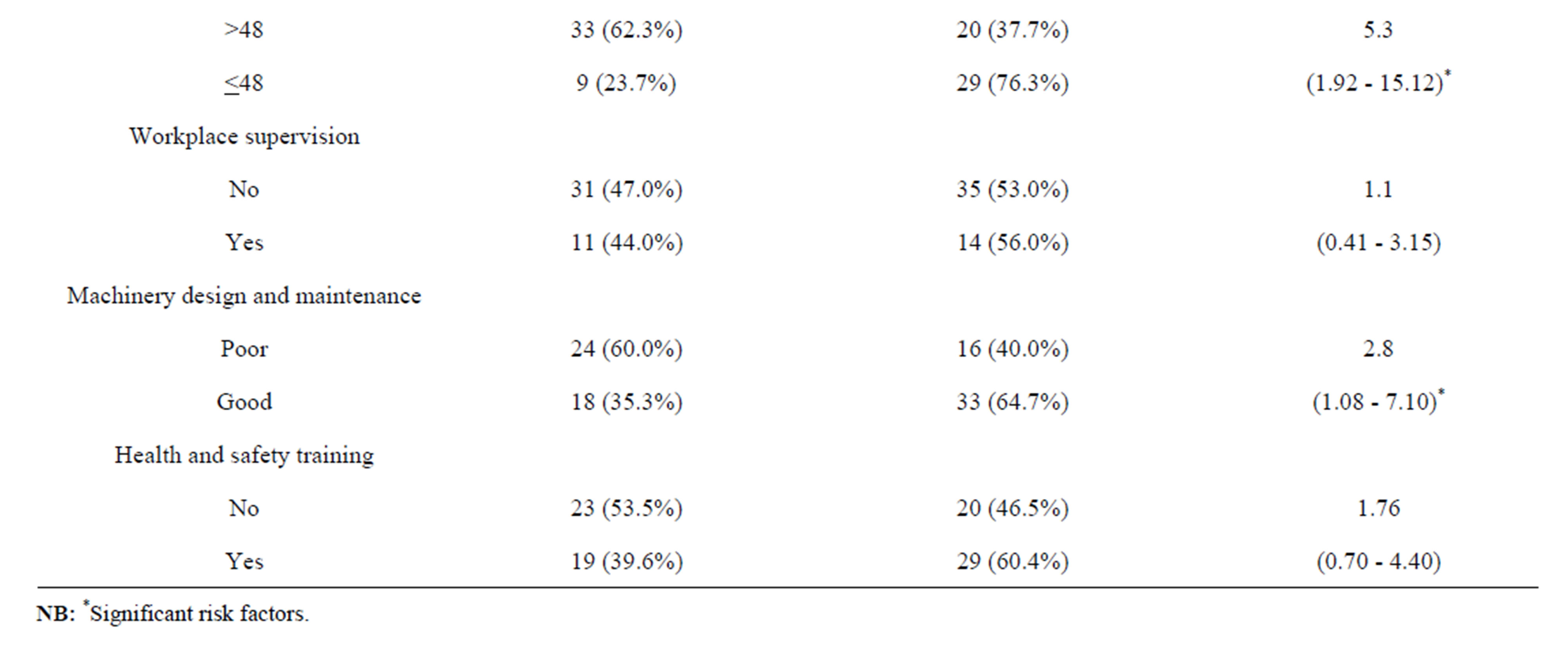
Table 3. Socio-demographic and work-related risk factors of occupational injuries among construction building workers: Results of bivariate analysis.
12 months were reported by 42 out of 91 construction workers (46.2%). This finding wasn’t surprising, where in most construction worksites, that were investigated by a recent Egyptian study, no training programs for workers existed, no orientation for new workers has been conducted, hazards were not pointed out as safety meetings were not held, inspection schedules and maintaining the equipment were often not fulfilled, and lack of workers’ compliance with safe work practices including negligence of wearing personal protective equipment were noticed [3].
A very interesting finding was that all participants with history of occupational injury didn’t fill an accident notification form. This finding also was not surprising, as

Table 4. Behavioral risk factors of occupational injuries among construction building workers: Results of bivariate analysis.
till now many developing countries including Egypt do not have reliable information about worksite injuries due to lack of proper recording and notification particularly for minor non-fatal injuries. Underreporting of occupational injuries means that preventative measures are not taken and early treatment is not conducted [3,31].
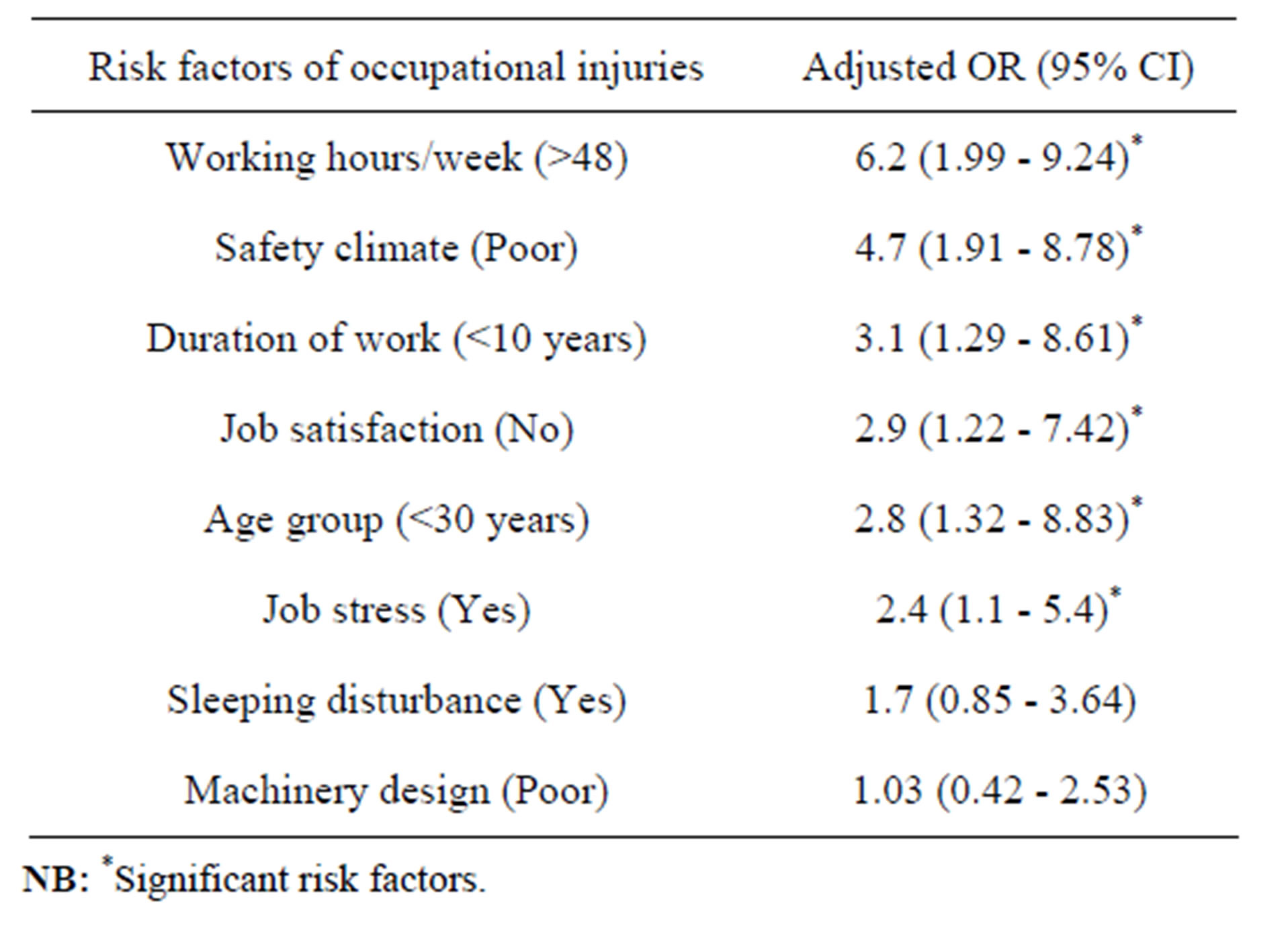
Table 5. Risk factors of occupational injuries among construction building workers: Results of stepwise multiple logistic regression analysis.
One of the strengths of the present study is that the data depend on self-reported injuries, where in other studies the data of injuries were obtained mostly from the official companies records with a possibility of underreporting, as there is a consistent trend among construction workers of “willful underreporting” of occupational injuries or diseases due to fear of missing work, or a promotion in a competitive market [32]. On the other hand, self-reported data might create a problem with information bias [33].
Many safety hazards are present in the construction industry, consequently knowing the causes of an accident is useful to develop and implement a program for preventing accidents in the future. Falls from elevation represented the leading cause of fatal injuries (33% of all deaths), getting struck by an object (22%), caught inbetween two objects (18%), and electrical shock (17%) are also important factors of construction fatalities in Egypt. In the same way, falls is the number one killer in construction work; where falls cause 100,000 injuries and up to 200 deaths annually in Europe [3]. Nearly similar findings were detected by the present study, where falls (47.6%), and injuries by manual tools (23.8%) were the main causes of injuries. Also, struck by an object (11.9%) and caught in-between two objects (9.5%) were important causes of injury. In a study that was conducted on construction workers (n = 2916) treated at the

Table 6. Safety climate level and its relationship with occupational injuries in construction building workers.
George Washington University Emergency Department over a 7-year period, the main causes of injury were sharp objects (26.1%), struck by/against an object (19.9%), and falls (17.1%). Machinery (4.9%) and caught between (4.4%) were less important mechanisms [34]. Moreover, other studies revealed that struck by an object (33.6% and 29.9%) and falls (30.2% and 29.3%) were the major causes of injury among construction workers [2,30].
Regarding the types of injury, the results of the present study agree with those of another similar study, where the data indicated that contusions (29.4%) and cuts (22.4%) were the most common injury types among a sample of construction workers [10]. Nearly similar results were obtained by another hospital-based study, where lacerations (37%), sprain, strains, and pain (22.3%), and contusions/abrasions (15.3%) were the main types of injury. Eye injuries (10.8%) and fractures (8.7%) were less important injury types [34]. Whereas, a three years period study in Kuwait revealed that fractures (59.4%) and wounds (cut, contused, and penetrating) (24%) were the commonest types of injuries among construction workers [30].
In agreement with the present study, hands (39.8%), lower extremities (31.2%) and upper limbs (arms and forearms) (16.2%) were the most frequently injured body parts among construction workers in Kuwait [30]. Moreover, in Egypt and in the same studied city, lower and upper limbs (35.3% and 32.9%, respectively) were the commonest anatomical locations of injuries [10]. While, the results of a hospital-based study partially agree with those of the present study, where upper limb (42.7%), head and neck (23.7%), and lower limb (18.5%) were the main body parts injured [34]. Whereas, in another Egyptian study, the most frequently recorded body parts affected in disabling injuries were head (23.7%), upper limb (15.1%), eyes (14.6%), and trunk and lower limb (13.8% for each) [2].
The construction industry accidents usually result in lost fingers, herniated discs, smashed toes, and crushed bodies by machines [3]. In the present study, the vast majority of injured workers (90.5%) reported complete recovery after the most serious injury; while disability occurred in only (9.5%) of them. In one Egyptian study that was conducted in a big construction company on 487 workers throughout three years, 59 workers had disabling injuries (12.1%) and 4 had fatal injuries (0.8%) in the year 2000, 68 workers had disabling injuries (13.9%) and 3 workers had fatal injuries (0.6%) in the year 2001, and 105 workers had disabling injuries (21.6%) and 2 workers had fatal injuries (0.4%) in the year 2002. The variation of the estimates of disabling injuries between the studies was explained by the same study as exposure to safety hazards differs according to the job demands [2]. Also, it may be due to that workers with major disabling injuries usually leave their jobs because of high physical demands of the construction work [21].
In the current study, the average of working days lost per year due to occupational injuries was (18.6 ± 7.8 days/year) (range 7 - 31 days/year).The International Labor Organization (ILO) reported that about 25 million people have workplace injuries, causing them to take time off. In Europe, 15 out of every 100 full-time construction workers suffer a lost-time injury (sprains and muscle strains accounts for 38%) annually, which is more than other industries. In addition, 85% of fall injuries results in lost time that costs employers $2 billion annually due to compensations and reduced productivity [3].
A very interesting finding was that, none of the injured workers reported receiving sufficient first-aid treatment at worksite. This finding confirms that of another Egyptian study, where only a few companies out of the surveyed sample provided workers with formal safety orientation and trained safety personnel in first-aid. In addition, there was lack of medical facilities and standard sanitation in the studied projects worksites [3]. A commonly used argument is that poor countries and companies cannot afford safety and health measures [2].
Regarding the risk factors of occupational injuries among construction workers, the results of the current study partially coincide with those of another study, where it was found that unsafe working environment and certain individual factors, including young age, lack of formal education and safety training, lack of experience, inadequate risk perception, personality, behavior, smoking habits, body weight, sleep disorders, and lack of physical activity can increase the risk of accidents [35]. Other studies found that young workers experienced higher risk of injuries. This was explained by the fact that, young age and shorter duration of employment are associated with less experience and less awareness about workplace hazards which contribute to risk taking behavior [36,37]. Also, young workers did not usually comply with safe work procedures [22]. Consistent with our results, a recent literature review demonstrated that shift work (afternoon and night shifts) and extended working hours were significantly related to increased risk of occupational accidents [38].
In contrast to our results, different studies in developing and developed countries found that sleep disturbances such as difficulty in initiating sleep, sleeping poorly at night, sleep insufficiency, and insomnia symptoms were significantly associated with the occurrence of occupational injuries. It was suggested that sleeping disturbance problems affect the ability to maintain wakefulness, concentration, ability in assessing or watching the work environment and working conditions and performing duties safely [22,39].
In the industrialized countries physical environments are now less important and dangerous than before, while organizational threats are becoming more important in many workplaces [13]. In the present study, job stress was found to be a significant risk factor for occupational injuries among the studied sample of construction workers. This finding can be explained as job stress can result in physiological and psychological problems that may increase the risk of sustaining more occupational injury at worksites [22]. Moreover, the results of this study showed significant association between job dissatisfaction and occupational injuries among the studied sample of construction workers. This is may be due to that job satisfaction plays an important role in the overall productivity and workers’ safety at any given industry [39].
The concept of safety climate was raised as an issue many years ago. Safety climate is the psychological aspects of the safety culture “how workers feel”. It reflects individuals’/groups’ values as well as attitudes and perceptions of safety [13]. From series of studies, it was evident that it is necessary to scientifically grasp the idea of and improve the workers’ safety climate in order to develop a safe organization [40,41].
Evaluating safety climate is much simpler than evaluating safety culture. Surveys based on questionnaires, which can be performed by the organization or by an external resource, are more common when evaluating safety climate. Both safety climate and culture are poorly defined and no consensus exists on how to distinguish or operationalize them and their relation with safety performance [1]. However, generally there is some supportive evidence for a relationship between safety climate measures and accidents [12].
Some studies have evaluated safety climate in relation to safety levels in the workplace, judgment of risk among employees [42], and accident rates [41,43]. A number of studies have also focused on the relation between healthcare workers’ perceptions of their organization’s prevention programs and compliance with universal precautions [44].
In the present study the mean score level of the general item of safety climate “In my company workers’ health and safety are sufficiently protected” among non-injured construction workers (6.8 ± 1.7) was nearly similar to that detected by a recent Spanish cross-sectional study of workers at the pottery industry (6.8 ± 2.2). While, the mean of safety climate index (SCI, summary of answers to items 2 - 11) was found to be slightly higher (71.9 ± 19.2) by the same study [13] compared to that detected by the present study (69.6 ± 12.2).
As safety climate in any organization is relatively changeable, self-reported injuries and workers’ perception in the past 12 months were recorded in the present study. It was found that the mean score levels of the general item of safety climate and of the safety climate index (SCI) were significantly higher among the non-injured construction workers than those among the injured workers. This is in accordance to the findings of a previous study, where poor safety climate perceptions of workers were related to workers’ unsafe behaviors and to lack of compliance with safety rules [13]. Consistent with those findings, many researchers found that poor safety climate was associated with unsafe behavior, and on a group-level related to work-related accidents [41]. Moreover, safety climate was considered as one way of identifying characteristics that might distinguish between employees with high or low injury rates [20].
Also, workers with a positive perception of their workplace safety (positive safety climate) have registered fewer accidents and fewer self-reported injuries. Thus, it has been suggested that a good safety culture actually contributes to an increased productivity and reduced costs in the long run [33,45].
5. Conclusions
Non-fatal injuries in the form of cuts/lacerations and contusions in upper and lower limbs were common among this sample of construction workers due to falls and handling of manual tools. However, none of the injured workers reported receiving sufficient first-aid treatment at worksite or filling an accident notification form. Extended working hours, poor safety climate, short duration of work, job dissatisfaction, young age, and job stress were significantly associated with self-reported injuries.
So, successful injury control programs that are based on a strong management commitment to safety should be implemented in the construction industry, including the responsibilities of safety officers within the organization, workers training and orientation to raise safety awareness and consciousness and to improve safety practices, effective communication between management and workers, general housekeeping, first-aid measures at worksites with trained safety personnel, and a stable workforce. Since falls represented the main cause of injuries among the studied sample of construction workers, fall protection requirements should be fulfilled at worksites.
Also, there is a need for implementing an occupational surveillance system to monitor and enforce safety requirements at worksites. The laws in Egypt need to be addressed to recommend changes in the insurance legislations to reflect the company’s record of safety. These legislations should provide incentives for construction companies to enhance their safety programs. Occupational Safety and Health Administration (OSHA) injury recordable criteria should be implemented, including death, loss of consciousness, days away from work, restricted work, job transfers, factors affecting routine job functions, serious injuries such as fractures or punctured eardrums, and medical treatment beyond first-aid.
Prospective study designs are recommended to find out the causal association between safety climate and other risk factors, particularly behavioral ones and occupational accidents and to evaluate the predicative value of the safety climate on self-reported injuries.
6. Acknowledgements
The authors would like to thank all participants of this study and the contractors for their great cooperation.
REFERENCES
- F. Guldenmund, “The Nature of Safety Culture: A Review of Theory and Research,” Safety Science, Vol. 34, No. 1-3, 2000, pp. 215-257. http://dx.doi.org/10.1016/S0925-7535(00)00014-X
- R. Alazab, “Work-Related Diseases and Occupational Injuries among Workers in the Construction Industry in Egypt,” African Newsletter on Occupational Health and Safety, Vol. 14, No. 2, 2004, pp. 37-42.
- A. Elsafety, A. Elsafety and M. Malek, “Construction Safety and Occupational Health Education in Egypt, the EU, and US Firms,” Open Journal of Civil Engineering, Vol. 2, No. 3, 2012, pp. 174-182. http://dx.doi.org/10.4236/ojce.2012.23023
- T. Afifi, “The Poor in the Egyptian Labor Market During an Adjustment Period: For Better or Worse?” Economic Research Forum, 2001, pp. 12-13. http://www.erf.org.eg/CMS/uploads/pdf/0117_Afifi.pdf
- H. Brenner and W. Ahern, “Sickness Absence and Early Retirement on Health Grounds in the Construction Industry in Ireland,” Occupational and Environmental Medicine, Vol. 57, No. 9, 2000, pp. 615-620. http://dx.doi.org/10.1136/oem.57.9.615
- H. Paivi, J. Takala and L. Kaja, “Global Estimates of Occupational Accidents,” Safety Science, Vol. 44, No. 2, 2006, pp. 137-156. http://dx.doi.org/10.1016/j.ssci.2005.08.017
- K. Bharara, P. Sandhu and M. Sidhu, “Issues of Occupational Health and Injuries among Unskilled Female Laborers in Construction Industry: A Scenario of Punjab State,” Studies on Home and Community Science, Vol. 6, No. 1, 2012, pp. 1-6.
- Ministry of Manpower and Immigration, “Analytical Study of Serious Accidents in Enterprises in the Arab Republic of Egypt,” Report prepared by the Safety and Occupational Health Department, 2002.
- Central Agency for Public Mobilization and Statistics (CAPMAS)—Arab Republic of Egypt, “Work Injuries Distributed according to Economic Activity at Construction Sector Containing 50 Workers and More,” 2012. http://www.capmas.gov.eg
- D. El-Shafei, “Some Occupational Health Hazards among a Group of Construction Workers with Emphasize on Accidents at Mit-Ghamr City, Dakahlia Governorate,” M.SC. Thesis, Zagazig University, Al Sharqia, 2007.
- T. Abdelhamid and J. Everett, “Identifying Root Causes of Construction Accidents,” Journal of Construction Engineering and Management, Vol. 126, No. 1, 2000, pp. 52-60.
- S. Clarke, “Safety Culture: Under-Specified and Overrated?” International Journal of Management Reviews, Vol. 2, No. 1, 2000, pp. 65-90. http://dx.doi.org/10.1111/1468-2370.00031
- A. Garcia, P. Boix and C. Canosa, “Why Do Workers Behave Unsafely at Work? Determinants of Safe Work Practices in Industrial Workers,” Occupational and Environmental Medicine, Vol. 61, 2004, pp. 239-246.
- I. Godwin, “Effect of Mechanization on Occupational Health and Safety Performance in the Nigerian Construction Industry,” Journal of Construction in Developing Countries, Vol. 16, No. 2, 2011, pp. 27-45.
- X. Huang and J. Hinze, “Owner’s Role in Construction Safety,” Journal of Construction Engineering and Management, Vol. 132, No. 2, 2006, pp. 164-173. http://dx.doi.org/10.1061/(ASCE)0733-9364(2006)132:2(164)
- Central Agency for Public Mobilization and Statistics (CAPMAS)—Arab Republic of Egypt, “Egypt in figures: Population Estimates by Governorate (Urban/rural areas),” 2011.
- A. Dean, J. Dean, D. Coulombeir and K. Brendel, “Epiinfo Version 6: A Word Processing Data Base and Statistics Program for Epidemiology on Microcomputers,” Center for Disease Control, Atlanta, 2001.
- Centers for Disease Control and Prevention (CDC), “Body Mass Index,” 2007. www.cdc.gov/nccdphp/dnpa/bmi/adult_bmi/about_adult_bmi.htm
- L. Fiala, R. Faris, S. Sobhy and J. Kraus, “Prevalence, Pattern of and Factors Affecting Occupational Injuries in the Conversion Industries in Ismalia,” Suez Canal University Medical Journal, Vol. 1, No. 1, 1998, pp. 13-20.
- C. Che Hassan, O. Basha and W. Wan Hanafi, “Perception of Building Construction Workers towards Safety, Health and Environment,” Journal of Engineering Science and Technology, Vol. 2, No. 3, 2007, pp. 271-279.
- A. Hassanein and R. Hanna, “Safety Performance in the Egyptian Construction Industry,” Journal of Construction Engineering and Management, Vol. 134, No. 6, 2008, pp. 451-455. http://dx.doi.org/10.1061/(ASCE)0733-9364(2008)134:6(451)
- Z. Aderaw, D. Engdaw and T. Tadesse, “Determinants of Occupational Injury: A Case Control Study among Textile Factory Workers in Amhara Regional State, Ethiopia,” Journal of Tropical Medicine, Vol. 2011, 2011, Article ID: 657275. http://www.hindawi.com/journals/jtm/2011/657275/
- J. Harrington, “Health Effects of Shift Work and Extended Hours of Work,” Occupational and Environmental Medicine, Vol. 58, No. 1, 2001, pp. 68-72. http://dx.doi.org/10.1136/oem.58.1.68
- K. Knowles and D. Robertson, “Differences between the Wages of Skilled and Unskilled Workers, 1880-1950,” Bulletin of the Oxford University Institute of Economics and Statistics, Vol. 13, No. 4, 2009, pp. 109-127. http://onlinelibrary.wiley.com/doi/10.1111/j.1468-0084.1951.mp13004002.x/abstract
- Marlin Company and the American Institute of Stress, “The Workplace Stress Scale: Attitudes in the American Workplace VII,” 2009. http://americaninstituteofstress.org/wp-content/uploads/2011/08/2001Attitude-in-the-Workplace-Harris.pdf
- S. Macdonald and P. Maclntyrem, “The Generic Job Satisfaction Scale: Scale Development and Its Correlates,” Employee Assistance Quarterly, Vol. l3, No. 2, 1997, pp. 1-16. http://faculty.capebretonu.ca/pmacintyre/research_pages/journals/job_staisfaction_1997.pdf
- IBM, “IBM SPSS Statistics 19 Core System Users’ Guide,” SPSS Inc., Chicago, 2010. http://www.ibm.com/software/analytics/spss/training
- ILO, “Safety and Health at Work,” 2013. http://www.ilo.org/global/topics/safety-and-health-at-work/lang--en/index.htm
- G. Eijkemans, “Occupational Health and Safety in Africa,” WHO/ILO, Vol. 14, No. 2, 2004, pp. 28-29.
- N. Zawilla, H. Bader and A. Al Shatti, “Non-Fatal Occupational Injuries and Disability in Construction Workers in Kuwait 2003-2005,” The Egyptian Journal of Occupational Medicine, Vol. 32, No. 1, 2008, pp. 43-61.
- P. Hamalainen, J. Takala and K. Saarela, “Global Estimates of Occupational Accidents,” Safety Science, Vol. 44, No. 2, 2006, pp. 137-156. http://dx.doi.org/10.1016/j.ssci.2005.08.017
- J. Leigh, S. Markowitz, M. Fahs and P. Landrigan, “Costs of Occupational Injuries and Illnesses,” University of Michigan, Ann. Arbor, 2000.
- K. Nielsen and K. Mikkelsen, “Predictive Factors for Self-Reported Occupational Injuries at 3 Manufacturing Plants,” Safety Science Monitor, Vol. 11, No. 2, 2007, pp. 1-9.
- K. Hunting, J. Murawski and L. Welch, “Occupational Injuries among Construction Workers Treated at the George Washington University Emergency Department 1990-97,” The Center to Protect Workers’ Rights (CPWR), 2004. http://www.cpwr.com
- N. Chau, G. Gauchard, C. Seigrid and I. Benamgher, “Relationship of Job, Age and Life Conditions with Causes and Severity of Occupational injuries in Construction Workers,” International Journal of Occupational and Environmental Health, Vol. 77, No. 1, 2004, pp. 60-66.
- F. Benavides, J. Benach, C. Muntaner and G. Delcos, “Association between Temporary Employment and Occupational Injuries: What are the Mechanisms?” Occupational and Environmental Medicine, Vol. 63, No. 6, 2006, pp. 416-421.
- A. Nakata, T. Ikedo and S. Takala, “Prevalence and Correlates of Occupational Injuries in Small Scale Manufacturing Enterprises,” Journal of Occupational Health, Vol. 38, No. 2, 2006, pp. 366-376.
- S. Salminen, “Shift Work and Extended Working Hours as Risk Factors for Occupational Injury,” The Ergonomics Open Journal, Vol. 3, 2010, pp. 14-18.
- O. Yiha and A. Kumie, “Assessment of Occupational Injuries in Tendaho Agricultural Development S.C, Afar Regional State,” Ethiopian Journal of Health Development, Vol. 24, No. 3, 2010, pp. 167-174.
- A. Neal, M. Griffin and P. Hart, “The Impact of Organizational Climate on Safety Climate and Individual Behavior,” Safety Science, Vol. 34, No. 1-3, 2000, pp. 99- 109. http://dx.doi.org/10.1016/S0925-7535(00)00008-4
- U. Varonen and M. Mattila, “The Safety Climate and its Relationship to Safety Practices, Safety of the Work Environment and Occupational Accidents in Eight WoodProcessing Companies,” Accident Analysis & Prevention, Vol. 32, No. 6, 2000, pp. 761-769. http://dx.doi.org/10.1016/S0001-4575(99)00129-3
- T. Rundmo, “Safety Climate, Attitudes and Risk Perception in Norsk Hydro,” Safety Science, Vol. 34, No. 1-3, 2000, pp. 47-59. http://dx.doi.org/10.1016/S0925-7535(00)00006-0
- H. Shannon, V. Walters, W. Lewchulk, et al., “Workplace Organizational Correlates of Lost-Time Accident Rates in Manufacturing,” American Journal of Industrial Medicine, Vol. 29, No. 3, 1996, pp. 258-268. http://dx.doi.org/10.1002/(SICI)1097-0274(199603)29:3<258::AID-AJIM5>3.0.CO;2-M
- R. Gershon, C. Karkashian, J. Grosch, et al., “Hospital Safety Climate and Its Relationship with Safe Work Practices and Workplace Exposure Incidents,” American Journal of Infection Control, Vol. 28, No. 3, 2000, pp. 211-221. http://dx.doi.org/10.1067/mic.2000.105288
- C. Smith, G. Silverman, T. Heckert, et al., “A Comprehensive Method for the Assessment of Industrial Injury Events,” Journal of Prevention and Intervention in the Community, Vol. 22, No. 1, 2001, pp. 5-20.
Appendix
1) Measuring the job stress level (The workplace stress scale) [25]:
Thinking about your current job, how often does each of the following statements describe how you feel?
Ÿ For statements (A, B, C, D, and E) (Never = 1), (Rarely = 2), (Sometimes = 3), (Often = 4), and (Very often = 5).
Ÿ For statements (F, G, and H) (Never = 5), (Rarely = 4), (Sometimes = 3), (Often = 2), and (Very often = 1).
A. Conditions at work are unpleasant or sometimes even unsafe.
B. I feel that my job is negatively affecting my physical or emotional well being.
C. I have too much work to do and/or too many unreasonable deadlines.
D. I find it difficult to express my opinion or feelings about my job conditions to my superiors.
E. I feel that job pressures interfere with my family or personal life.
F. I have adequate control or input over my work duties.
G. I receive appropriate recognition or rewards for good performance.
H. I am able to utilize my skills and talents to the fullest extent at work.
2) Job satisfaction scale [26]:
For each statement please write the number to indicate your degree of agreement: (Strongly disagree = 1), (Disagree = 2), (Don’t know = 3), (Agree = 4), and (Strongly agree = 5).
1. I receive recognition for a job well done.
2. I feel close to the people at work.
3. I feel good about working at this company.
4. I feel secure about my job.
5. I believe management is concerned about me.
6. On the whole, I believe work is good for my physical health.
7. My wages are good.
8. All my talents and skills are used at work.
9. I get along with my supervisors.
10. I feel good about my job.
3) Safety climate questionnaire [13]:
(Level of accord on a numeric scale from 0 to 10)
General item
1. In my company workers’ health and safety are sufficiently protected.
Specific items
2. Management is seriously involved in occupational risk prevention.
3. Productivity and safety at work are equally important.
4. My company invests in risk prevention.
5. Supervisors encourage safe behavior.
6. Supervisors take into account my opinion and suggestions on health and safety.
7. There are persons exclusively devoted to health and safety.
8. Persons devoted to health and safety are competent.
9. There are explicit rules for safe working.
10. I have received adequate health and safety training.
11. I have received adequate equipment for personal protection.