Open Journal of Stomatology
Vol.3 No.3(2013), Article ID:33701,3 pages DOI:10.4236/ojst.2013.33038
The effectiveness of local anesthetic and sodium hyaluronate injection for the posterior disc displacement: A case report
![]()
1Second Department of Oral and Maxillofacial Surgery, Osaka Dental University, Osaka, Japan
2Department of Oral Radiology, Osaka Dental University, Osaka, Japan
Email: *akiyama@cc.osaka-dent.ac.jp
Copyright © 2013 Yui Mori et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 12 April 2013; revised 12 May 2013; accepted 1 June 2013
Keywords: Posterior disc displacement without reduction; Temporomandibular joint; Local anesthetic with sodium hyaluronate injection; Intermaxillary traction; Magnetic resonance imaging.
ABSTRACT
Posterior disc displacement of the temporomandibular joint is rare. We present a unique treatment method and magnetic resonance (MR) images of this condition. The patient was a 43-year-old male with a chief complaint of abnormal occlusion. Regarding the present status, there was no occlusion on the right side. No temporomandibular joint pain, myalgia, or clicking were observed while mouth opening. On MR images, the posterior disc displacement without reduction on the right was observed and it was assumed that occlusal abnormality was due to this condition. We treated him with the following methods. After injection into the superior articular cavity with 2% lidocaine, a sodium hyaluronate preparation was injected followed by intermaxillary traction applied using rubber. The recovery of occlusion was confirmed in follow-up at 5 days after treatment. In the 13th days, the intermaxillary traction was removed. On MR images, the right disc condition was changed to anterior disc displacement with reduction. We consider our treatment methods are effective for this clinical condition.
1. INTRODUCTION
Temporomandibular joint (TMJ) arthritis shows various kind of conditions and, up to now, many authors have reported the treatment methods. However, posterior disc displacement of the TMJ is very rare, and only a few cases have been reported [1-10]. In addition, the cause or treatment method has not been clarified. In our hospital we treated it with the local anesthetic and sodium hyaluronate injection into the superior articular cavity combined intermaxillary traction, and achieved early improvement and favorable recovery. Herein, we report the case.
2. CASE REPORT
The patient was a 43-year-old male and his chief complaint was abnormal occlusion. His right occlusion was suddenly lost 3 months before visiting our hospital, and it did not resolve. So, he visited an oral surgery department of another hospital, but no therapeutic policy could be established, and he was referred to our hospital on September 2011.
Regarding the present status, the distance of mouth opening was 40 mm, and there was no occlusal contact at the right side of the mandible. On the left side, there was occlusal contact and the mandibular midline deviated rightward (Figure 1). Previously, clicking had noted while mouth opening. However, no TMJ pain, myalgia, or clicking while mouth opening was noted. Past medical history was median mandibular fracture (15 years ago, treated with intermaxillary fixation).
To take magnetic resonance (MR) imaging, we used a 1.5 tesla MR scanner, Signa Horizon LX (General Electric, Milwaukee, WI, USA). We took T2 and Proton Density weighted images in mouth closing position and T1 weighted images in mouth closing and opening position with fast spine echo sequence. On para-sagittal
 (a) (b) (c)
(a) (b) (c)
Figure 1. Occulusion was shown at the first examination (b). There was no occlusal contact at the right (a). On the left side, there was occlusal contact (c).
MR images of the TMJ, posterior disc displacement without reduction on the right side and anterior disc displacement with reduction on the left side were observed and no bone change was observed (Figure 2). Joint effusion was not observed on T2 weighted images.
The injection into the superior articular cavity with pharmaceutical agents and intermaxillary traction using rubber (Elastics® HEAVY 4 mm) were performed 4 weeks after the first examination. For injection, a local anesthetic, 2% lidocaine (Xylocaine Polyamp®, epinephrine-free) was used. There was resistance to injection, suspected to be due to stenosis of the superior articular cavity, but injection of 0.5 ml of the anesthetic was possible. Finally, 2.5 ml of sodium hyaluronate preparation was injected, followed by strong traction of the right side by handing grade-III elastics and traction of the upper and lower jaws using vertical rubber on the left side (Figure 3). After treatment, mouth opening was limited and the patient ate a liquid diet. The patient stated that right occlusion resumed 30 minutes after treatment. Occlusion was improved on follow-up at 5 days after pumping (Figure 4). Since no change was noted in the occlusal condition on follow-up at 13 days, intermaxillary traction was removed (Figure 5). The condition of the right disc altered to anterior disc displacement with reduction on MRI (Figure 6). No change was noted in the occlusal condition on follow-up at 6 weeks, and the recovery course was favorable without temporomandibular symptom.
3. DISCUSSION
Concerning internal derangement in TMJ, the disk is often displaced anteriorly with or without reduction. Therefore, posterior disc displacement is very rare [1-10], and the cause or treatment method has not been clarified. Posterior disc displacement of TMJ occurs at the end of mouth closing or on wide mouth opening [2,3,9,10]. The former is associated with posterior disc displacement without reduction and the latter is associated with temporomandibular dislocation (posterior disc displacement without reduction on wide mouth opening) or open lock (posterior disc displacement with reduction on wide mouth opening): articular disc incoordination. MRI is ne-
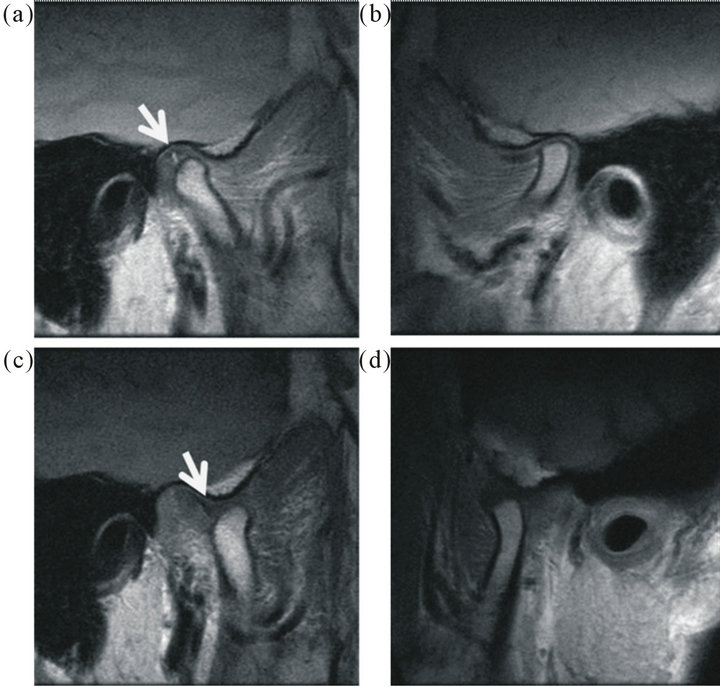
Figure 2. On para-sagittal MR images at the initial visit, non-reducible posterior displacement of the right disc (arrow, (a) proton density weight image; (d) T1 weighted image) and reducible anterior displacement of the left disc were noted (b) proton density weighted image; (c) T1 weighted image).
 (a) (b) (c)
(a) (b) (c)
Figure 3. Intermaxillary traction was shown (b). After injection of the anesthetic and sodium hyaluronate, we followed by strong traction of the right side by hanging grade-III elastics to correct occlusal contact (a) and traction of the upper and lower jaws using vertical elastics on the left side to restrict mouth opening (c).
 (a) (b) (c)
(a) (b) (c)
Figure 4. Occlusion was improved on follow-up at 5 days after injection. Lateral view on the right (a), frontal view (b) and lateral view on the left (c) were shown.
ssary to differentiate these diseases.
Since the condyle was located anterior to the articular disc while opening and closing the mouth on MRI, in addition to clinical findings reported by Blankestijn et al. [1], the patient was diagnosed posterior disc displace-
 (a) (b) (c)
(a) (b) (c)
Figure 5. Since no change was noted in the occlusal condition on follow-up at 13 days after injection, intermaxillary traction was removed. Lateral view on the right (a), frontal view (b) and lateral view on the left (c) were shown.
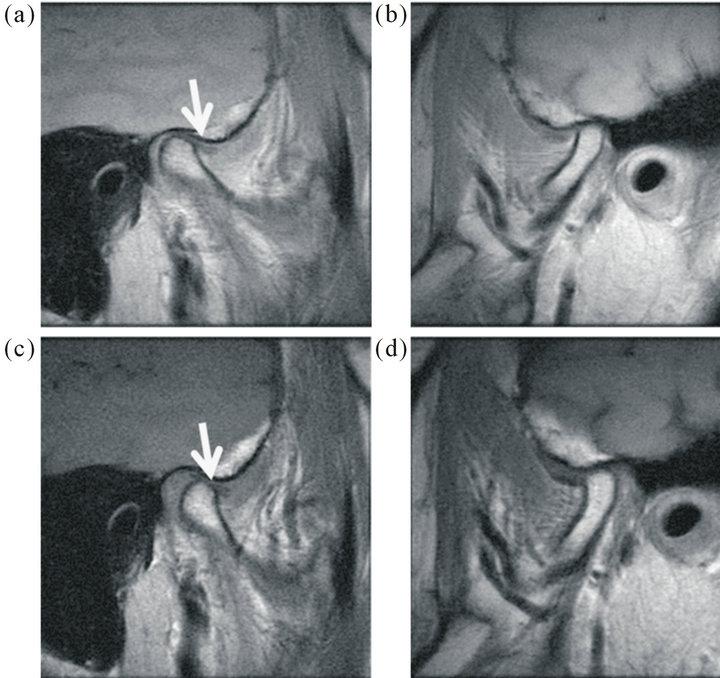
Figure 6. The closed-mouth proton density weighted image for the right side (a) and for the left side (b) and the open mouth T1 weighted image for the right side (c) and for the left side (d) after treatment were shown. The condition of the right disc altered to anterior displacement with reduction on MR images (arrow, (a), (b)).
ment without reduction which occurred at the end phase of mouth opening.
The cause was unclear in many cases, but, yawning, trauma, a facial blow, unilateral chewing, and malocclusion were assumed to be inducers [3,4,10]. This patient had a past medical history of a median mandibular fracture caused by a blow 15 years ago, and underwent open reduction and fixation at the department of plastic surgery at another hospital. This trauma may be a cause. However, because clicking while mouth opening was already present before the injury, we suggested that anterior disc placement had already occurred.
For the treatment of posterior disc displacement, conservative treatment is considered to be the first-choice [2-4]. Reportedly, pumping manipulation is useful because it dilates the superior articular cavity with local anesthetic, facilitating reduction of the articular disc [2,10]. We performed local anesthetic and sodium hyaluronate injection, and applied only intermaxillary traction without manipulation, expecting spontaneous mobility of the disc. The local anesthetic and sodium hyaluronate injection may have dilated the articular cavity and increased articular disc mobility, leading to the original anterior disc displacement without reduction. The occlusion resumed 30 minutes after treatment. The improvement was earlier than those in previously reported cases, suggesting that local anesthetic and sodium hyaluronate injection which had combined intermaxillary traction were particularly effective for these clinical conditions.
REFERENCES
- Blankestijn, J. and Boering, G. (1985) Posterior dislocation of the temporomandibular disc. International Journal of Oral Surgery, 14, 437-443. doi:0.1016/S0300-9785(85)80076-4
- Kakudo, K., Higashino, Y., Shirasu, R. and Shibata, T. (1991) A case report of posterior disc displacement without reduction of TMJ. Journal of the Japanese Society for the Temporomandibular Joint, 3, 137-142.
- Fukumoto, Y., Sugisaki, M., Iwamoto, S., Shigematsu, S., Takigawa, Y. and Ohtsuru, H. (2002) Mouth closing disturbance caused by the disc of the temporomandibular joint. Japanese Journal of Oral and Maxillofacial Surgery, 48, 284-287. doi:10.5794/jjoms.48.284
- Ohhara, A., Kobayashi, R., Sato, R., Nesori, F., Wagai, F. and Sekiyama, S. (2002) A case of posterior disc displacement of the temporomandibular joint treated by arthroscopic surgery. Japanese Journal of Oral and Maxillofacial Surgery, 49, 47-50. doi:10.5794/jjoms.49.47
- Sumiyoshi, S., Shimoda, T. and Honda, T. (1995) A case of posterior disc displacement of TMJ treated by arthroscopic surgery. Japanese Journal of Oral and Maxillofacial Surgery, 41, 653-655. doi:10.5794/jjoms.41.653
- Xu-Chen, M., Zhao-Ju, Z. M. and Zhen-Kang, Z. (1983) Temporomandibular joint arthrography. A study of some diagnosis at superior joint cavity arthrography. Dentomaxillofacial Radiology, 12, 17-24.
- Kai, S., Kai, H., Nakayama, E. and Tashiro, H. (1991) Convervative treatment of a patient with habitual anterior dislocation of the temporomandibular joint. Relation to incoordination of the disc. Japanese Journal of Oral and Maxillofacial Surgery, 37, 481-491. doi:10.5794/jjoms.37.481
- Nara, J., Toriyabe, Y., Shimazu, S., Nishimura, T. and Kita, S. (1991) A case report posterior disc displacement without reduction of TMJ. Japanese Journal of Oral and Maxillofacial Surgery, 43, 79-81.
- Honda, T., Shimoda, T. Moses, J.J. and Harada, H. (1994) Traumatically induced posterior disk displacement without reduction of the TMJ. Cranio, 12, 128-132.
- Fujita, Y., Sugisaki, S., Soma, K. and Ohnishi, M. (1993) A case of malocclusion with posterior disc displacement of the temporomandibular joint. Japanese Journal of the Japanese Society for the Temporomandibular Joint, 5, 108-119.
NOTES
*Corresponding author.