Journal of Cosmetics, Dermatological Sciences and Applications
Vol.2 No.2(2012), Article ID:20082,4 pages DOI:10.4236/jcdsa.2012.22010
Reconstruction of Chin Defects Using an O to Z Bilateral Rotation Flap*
![]()
Department of Dermatology, Emory University, Atlanta, USA.
Email: {sasha.nicole.jenkins, kchille}@emory.edu
Received April 1st, 2012; revised May 6th, 2012; accepted May 15th, 2012
Keywords: Skin Cancer; Reconstruction; Mohs Micrographic Surgery; Cosmetic
ABSTRACT
Reconstruction of defects on the chin represents a challenge given the functional, multidirectional movement of the chin subunit. In this article, we describe the surgical technique of a bilateral O to Z rotation flap on the chin, as well as complications, cosmetic outcome, and patient satisfaction. A retrospective chart review from January 2009-June 2011 identified twelve patients where an O to Z flap was used to repair a surgical defect. Of the twelve patients identified, one patient had a presumed post-operative infection, and one patient required additional corrections. There were no complications of hematomas or flap necrosis. Overall patient cosmetic outcome was excellent. An O to Z closure is an option for chin reconstruction of small to medium defects that offers a satisfactory cosmetic outcome, high patient satisfaction and low complication rate.
1. Background
Reconstruction of a defect on the chin following surgical excision represents a challenge to the surgeon. In this unique anatomical subunit of the face, direct muscle insertion into the skin causes functional, multidirectional movement of the area. The chin has multiple convexities and concavities, and involves multiple soft tissue components and muscle layers. Larger defects on the chin can involve the upper cutaneous lip and vermillion border. Thus, repairing defects of the chin can be technically difficult given poor design can lead to functional disabilities.
There are various options in repairing chin defects following Mohs micrographic surgery, such as secondary intention healing, full thickness skin grafts, or primary closure. However, these options do not represent satisfactory outcomes, as scars often appear hypertrophic, tethered or puckered. Full thickness grafts on the chin yield a poor cosmetic outcome given the inability of the graft to form to the natural chin concavity. Secondary intention healing is best used for concave surfaces, such as the medial canthus [1]. For large defects of the chin, use of lateral V-Y advancements and laterally based platysmal flaps have been used under general anesthesia [2-5]. However, there is a paucity of literature on surgical techniques used to repair small to medium sized chin defects. Thus, we sought to describe the O to Z closure of chin defects.
2. Methods
After approval from Sterling Institutional Review Board, a retrospective chart review was performed from January 2009-June 2011 to identify patients with surgical defects of the chin who underwent bilateral O to Z rotation flap following Mohs micrographic surgery. From this review, a total of twelve patients were identified. All patients were followed at Atlanta Skin Cancer Specialists, and digital photographs were taken preoperatively, post excision, and following defect closure. Patients were reassessed and additional pictures were taken at suture removal visit, eight-week follow up visit, and future visits (Figures 1-4). Occasionally patients did not return for their eight-week follow up appointment due to full cosmetic satisfaction. In these cases, a telephone call was made to the patient for satisfaction assessment. From these follow-up visits, necrosis, post-op infection, dehiscence, development of a hematoma, pin cushioning and if the patient required additional scar revision were recorded. In addition, to assess patients’ cosmetic satisfaction with their repair, all patients were contacted via telephone. Three attempts were made at calling all patients. Only two patients could not be contacted. Five patients, or 42%, were contacted after one year of their surgery and five patients were contacted seven months

Figure 1. Basal cell carcinoma on the chin of a 65 year old Caucasian female.

Figure 2. Surgical defect on the chin following Mohs surgery.

Figure 3. Chin reconstruction using the bilateral O to Z flap.
after their surgery. Two patients were contacted three months after their surgery. Patients were asked to evalu-

Figure 4. 65 year old female at her eight week follow up visit.
ate their scar based on three questions ranked from fair, good, or excellent. Patients were asked their overall satisfaction with their cosmetic results, if anyone has made a comment about their scar in the past 6 months, and if they felt the need to cover their scar with makeup.
3. Surgical Technique
Each patient with a skin cancer on their chin was individually assessed for the optimal repair, which was directed by the goals of surgical and cosmetic outcome. Patients with a small to medium size defect were chosen for a bilateral O to Z rotation flap. The O to Z flap is useful in patients where opposing sides of the defect, usually a circular defect, has available tissue. After clear margins, repair of the circular defect on the chin was performed. Two curvilinear incisions on opposite sides of the defect were made, roughly 1.5 to 2 times the diameter of the central defect. Undermining was performed on all sides of the defect, and then the two flaps were brought together with placement of one to two sutures in the center with additional corner sutures [6].
4. Results
A total of twelve patients underwent an O to Z closure of the chin following Mohs micrographic surgery from January 2009 to June 2011. The type of skin cancer in all of the patients was basal cell carcinoma. Of the twelve patients, four were men (33%) and eight (67%) were women. The average age of the patients was 63 years, ranging from 32 years old to 82 years old. The average defect size (largest diameter) was 1.5 cm, and the median was 1.05 cm. The average flap size (largest diameter) was 3.4 cm, and the median was 3.3 cm. The majority of cases required either 1 (33%) or 2 (50%) stages, and only 2 cases required 4 stages (Table 1).
Of the twelve patients reviewed, only one patient did not follow up at their designated clinic visit. However, this patient was reached by telephone and described no complications with their repair site. There were no incidents of flap necrosis, hematoma, dehiscence, or pin cushioning in the remainder of patients. Only one patient had a presumed post-operative infection. This patient was out of town and called the clinic with a complaint of drainage and tenderness at their surgical site. In addition, there was only one patient who required additional correction of their scar with intralesional kenalog at postoperative weeks 12 and 16.
Of the patients’ rating of their overall cosmetic satisfaction with their repair, 80% ranked their satisfaction as excellent or good, 80% responded that no one else commented on their scar in the past 6 months and only 40% felt the need to cover their scar up with make up.
5. Discussion
The chin presents a challenging subunit of the face to reconstruct following excision of skin cancer given the complexity of the anatomy and functionality of the chin. We describe a technique using an O to Z closure on defects < 4 cm on the chin that provides rarely any postoperative complications with a successful cosmetic outcome and patient satisfaction.
There are various options for repairing chin defects, including full thickness skin grafts, secondary intention healing, and flap options, such as bilobed, rhomboid, platysmal and V-Y advancement flaps. As mentioned earlier, the use of skin grafts on the chin leads to a suboptimal cosmetic outcome given the inability of the skin graft to conform to the multiple convexities of the chin. As described by Zitelli, concave surfaces provide the most optimal location for secondary intention healing [1].
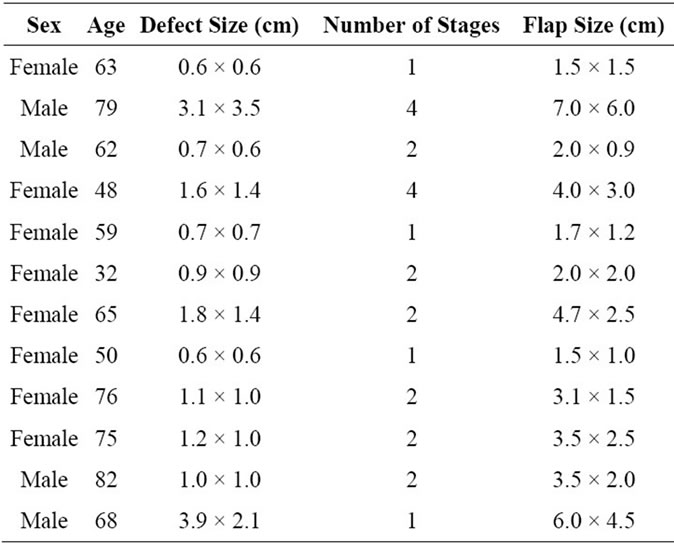
Table 1. O to Z reconstruction cases of the chin.
In a study by Mott et al., they concluded that regardless of the degree of wound contraction, final cosmetic outcome is most dependent on location [7]. Thus, the chin does not provide an optimal location for secondary intention healing. Given the poor skin laxity and multidirectional movement on the chin, primary closure is not an ideal closure option. Primary closure in a horizontal plane can lead to lip eclabium, while closure in the vertical orientation requires significant undermining and dog-ear excision [8]. For larger defects on the chin, such as defects > 5 cm, use of V-Y advancement flaps or platysmal flaps may be necessary [3,4].
Although the O to Z flap design is most often used for closing defects on the scalp, and less commonly on the forehead and temple, the chin is another area where this type of rotational flap can be used. The O to Z repair is an excellent option for defects of the chin following Mohs surgery, providing a simple technique, minimal complication rate, with excellent functional and aesthetic outcome and patient satisfaction. The use of this technique on the chin provides a smooth closure, and keeps the contour of the chin intact without a dog-ear effect. In this series of patients, only one patient had a presumed post-operative surgical infection, and only one patient required additional scar revision using intra-lesional kenalog. The majority of patients were extremely satisfied with their cosmetic outcome. For chin defects < 4 cm in size, it is possible to perform an O to Z closure with optimal cosmetic outcome and patient satisfaction.
6. Conclusion
For chin defects < 4 cm in size, an O to Z closure is a simple technique that provides satisfactory functional and cosmetic outcome, as well as patient satisfaction. We consider it as an acceptable reconstruction technique for chin defects less than 4 cm in size.
7. Authors’ Contributions
Dr. Nalovic performed all surgeries described in this manuscript. Dr. Jenkins performed the chart review, collected data, and contacted all patients as described in the manuscript. Both Drs. Nalovic and Jenkins drafted the manuscript. Dr. Jenkins had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
REFERENCES
- J. A. Zitelli, “Wound Healing by Secondary Intention—a Cosmetic Appraisal,” Journal of the American Academy of Dermatology, Vol. 9, No. 3, 1983, pp. 407-415. doi:10.1016/S0190-9622(83)70150-7
- H. A. Khan and N. S. Niranjan, “Four V-Y Islanded Flap Reconstruction of Full Thickness Defect of Chin and Labial Sulcus,” British Journal of Plastic Surgery, Vol. 57, No. 3, 2004, pp. 278-281. doi:10.1016/j.bjps.2003.11.025
- J. Thornton and M. Reece, “Submental Pedicles Perforator Flap: V-Y Advancement for Chin Reconstruction,” Journal of Oral and Maxillofacial Surgery, Vol. 66, No. 12, 2008, pp. 2633-2637. doi:10.1016/j.joms.2008.01.028
- F. Moschella and A. Cordova, “Platysma Muscle Cutaneous Flap for Large Defects of the Lower Lip and Mental Region,” Plastic and Reconstructive Surgery, Vol. 101, No. 7, 1998, pp. 1803-1809. doi:10.1097/00006534-199806000-00005
- J. C. Posnick and J. B. McGraw, “Reconstruction of the Chin-Lower Cheek Complex with a Platysma Myocutaneous Flap,” Journal of Oral and Maxillofacial Surgery, Vol. 46, No. 2, 1988, pp. 152-155. doi:10.1016/0278-2391(88)90270-4
- J. Ratz, “Textbook of Dermatologic Surgery,” Lippincott Raven, Philadelphia, 1998.
- K. Mott, D. Clark and L. Stelljes, “Regional Variation in Wound Contraction of Mohs Surgery Defects Allowed to Heal by Second Intention,” Dermatologic Surgery, Vol. 29, No. 7, 2003, pp. 712-722. doi:10.1046/j.1524-4725.2003.29180.x
- S. Soliman, D. Hatef, L. Hollier and J. Thornton, “The Rationale for Direct Linear Closure of Facial Moh’s Defects,” Plastic and Reconstructive Surgery, Vol. 127, No. 1, 2011, pp. 142-149. doi:10.1097/PRS.0b013e3181f95978
NOTES
*Disclosures: No financial disclosures. No conflicts of interest. No funding support. No acknowledgments.