Open Journal of Clinical Diagnostics, 2011, 1, 26-28 OJCD
doi:10.4236/ojcd.2011.13006 Published Online December 2011 (http://www.SciRP.org/journal/ojcd/).
Published Online December 2011 in SciRes. http://www.scirp.org/journal/OJCD
Enlarged cauda equina nerve roots in cerebrotendinous
xanthomatosis
Peter Kalina
Division of Neuroradiology, Department of Radiology, Mayo Clinic, Rochester, USA.
Email: kalina.peter@mayo.edu
Received 20 October 2011; revised 29 November 2011; accepted 8 December 2011.
ABSTRACT
CXT is a rare inherited autosomal recessive lipid
storage disease due to the impaired metabolic path-
way of cholesterol secondary to a deficiency in 27-
sterol hydroxylase, an enzyme in the synthesis of
chenodeoxycholic acid (CDCA), a primary bile acid.
Abnormal bile acid synthesis leads to elevated plasma
Cholestanol (a derivative of cholesterol) accumula-
tion, especially in the lens, central nervous system
(CNS) and tend ons.
Keywords: Cerebrotendinous X anthomat osis; Cauda Equina;
Peripheral Neuropathy
1. CASE REPORT
A 41 year old male from Kuwait presented with imbal-
ance, lower extremity weakness and spasticity, difficulty
walking and standing. Physical examination revealed
hyperreflexia, positive Babinski sign, vibratory sensory
loss, bilateral pes cavus, arched feet, hammer toes, val-
gus deformity of the ankles, atrophic changes of the
calves and thighs, Achilles tendon nodules and bilateral
cataracts. EMG findings were compatible with periph-
eral neuropathy. Laboratory examination was notable for
elevated plasma cholesterol and increased urine bile al-
cohol. Serum enzyme studies confirmed the diagnosis of
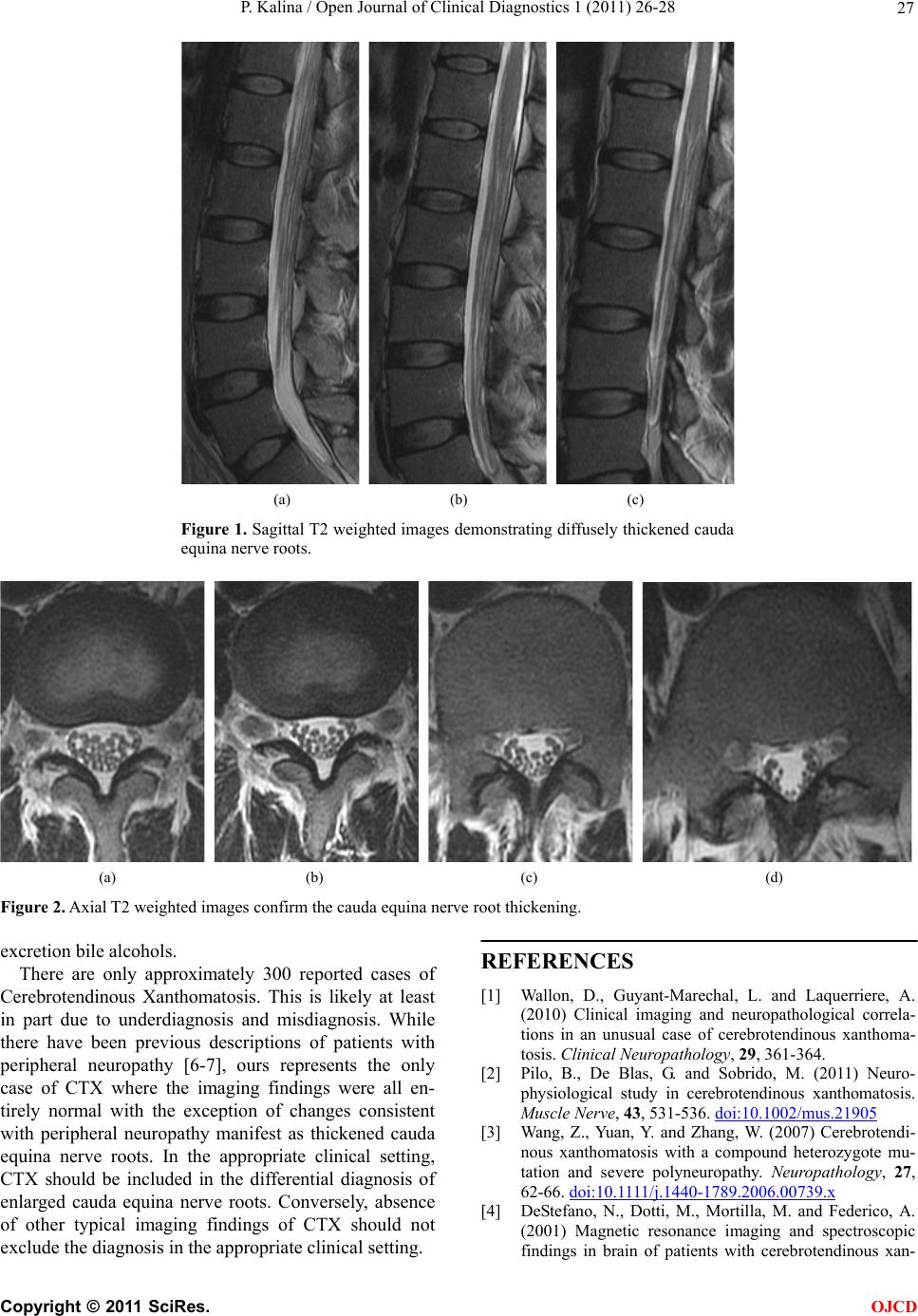
Cerebrotendinous Xanthomatosis (CTX). Magnetic res-
onance imaging (MRI) of the brain and entire spin e with
contrast were normal with the exception of diffusely
thickened caud a equi na ne rv e roots (Figures 1 and 2).
2. DISCUSSION
The classic clinical triad of CTX is Achilles tendon xan-
thomas, juvenile cataracts and progressive neurological
impairment. These clinical hallmarks then prompt a
search for increased urine bile alcohol and serum cho-
lestanol. Most severely affected is the cerebellar white
matter, optic pathways, brainstem and spinal cord.
Ischemic heart disease, premature atherosclerosis and
osteoporosis are also seen. Onset of signs and symptoms
is usually in childhood with bilateral cataracts, diarrhea,
neurological abnormalities, tendon xanthomas, gait dis-
turbance, epilepsy and polyneuropathy [1].
CNS findings include myelin loss and axonal degen-
eration. Enzyme defect leads to accumulation of neuro-
toxic metabolites leading to neuronal loss and axonal
degeneration. It remains uncertain whether the pathology
is demyelination or neuroaxonal disease with secondary
myelin loss [2].
Peripheral neuropathy is manifest clinically as Pes
cavus, hammer toes, weakness of small intrinsic muscles
of the foot and foot drawn into a claw-like position.
EMG confirms the peripheral nerve damage as slow
motor/sensory conduction due to demyelinating neu-
ropathy. Sural nerve biopsy confirms demyelinating pe-
ripheral neuropathy [3].
MRI findings include symmetric T2 hyperintense le-
sions in the white matter of the cerebellum and spinal
cord and may also be present in the internal capsule,
dentate, globus pallidus, substantia nigra, inferior olive
as well as adjacent white matter, especially adjacent to
basal ganglia and infratentorial, consistent with demye-
lination. Atrophy may be seen in the cerebrum, cerebel-
lum, brainstem, corpus callosum and cervical cord. MRS
findings include decreased NAA reflecting neuronal and
axonal damage and increased lactate due to mitochon-
drial dysfunction from toxic effect of elevated cho-
lestanol and bile alcohol [4].
CDCA replacement therapy slows or reverses disease
progression including improving neurological function
by suppressing abnormal bile acid synthesis and reduc-
ing elevated cholestanol synthesis thus decreasing
plasma cholestanol and its deposition [5]. Xanthomas
slightly decrease in size. Electrophysiologic studies im-
prove with reduced nerve conduction velocity; slowed
somatosensory evoked potentials. Diag nosis and therapy
are evaluated by serum cholestanol/cholesterol and ur ine