Journal of Cancer Therapy
Vol.5 No.6(2014), Article
ID:46236,8
pages
DOI:10.4236/jct.2014.56063
Influence of GSTT1, GSTM1 and GSTP1 Polymorphisms on the Development of Breast Cancer
Marisol Rodríguez1, Fernando Mejia2, Mariana Lecourtois3, Victoria Domínguez2, Julieta Castillo2*
1Facultad de Química, Universidad Autónoma del Estado de México, Toluca de Lerdo, México
2Centro de Investigación en Ciencias Médicas, Universidad Autónoma del Estado de México, Toluca de Lerdo, México
3Facultad de Odontología, Universidad Autónoma del Estado de México, Toluca de Lerdo, México
Email: *jcastilloc@uaemex.mx
Copyright © 2014 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 11 January 2014; revised 10 February 2014; accepted 18 February 2014
ABSTRACT
Introduction: Every year, more than 10 million women are diagnosed worldwide with breast cancer. Breast cancer remains the leading cause of death from malignancy in women. In Mexico about 12 Mexican women die every day from this disease. Glutathione S-transferase (GST) family consists of a group of isoenzymes involved in Phase II detoxification of xenobiotics by glutathione conjugation. There have been reports showing GST polymorphisms as a risk factor for developing cancer. Objective: Determine if the frequencies of polymorphisms of GSTT1, GSTM1 and GSTP1 are associated with breast cancer development. Materials and Methods: We studied 22 women with breast cancer and a control group of 30 women. DNA was extracted from blood. Polymorphisms of T1 and M1 were identified by multiplex PCR. The identification of GSTP1b (exon 5) and GSTP1c (exon 6), was performed separately by RFLP-PCR, using BsmAI and AciI enzymes respectively. Results: Frequencies of polymorphisms were as follows: for breast cancer group 33% null GSTT1 vs 40% null in the control, 32% null GSTM1 vs 63% of control; 63% heterozygote GSTP1b P1a/P1b and 18% homozygote P1b/P1b, vs 53% heterozygote and 20% homozygote in the control, 41% heterozygote P1a/P1c GSTP1c and 0% homozygote vs 10% heterozygote P1c/P1c and 0% homozygote control. Significant differences were found between GSTM1 and GSTP1c polymorphisms with GSTM1 null percentage higher in the control group and a higher frequency of P1c heterozygotes in the cancer group. Conclusion: As this is a pilot study where the results showed no association with breast cancer, further investigation is required on the involvement of GST genes in neoplasm development.
Keywords:Breast Cancer, Polymorphisms, GSTM1, GSTT1, GSTP1

1. Introduction
Cancer arises from the accumulation of genetic and epigenetic alterations; the most common alterations include amplification of proto-oncogenes and loss of chromosomal material; this causes loss of control of the cell cycle and sidestepping DNA repair and apoptosis, al-lowing the cell to replicate uncontrollably [1] [2] .
It is estimated that each year more than 10 million women worldwide are diagnosed with breast cancer and about 7 million deaths directly or indirectly occur due to this malignancy, which remains the leading cause of cancer death in women. There were 4206 deaths from breast cancer in Mexico in 2005; this means that about 12 Mexican women die from it every day. In year 2006, incidence of breast cancer outdid cervical cancer and ranked as the second leading cause of death among women 30 to 54 years old [3] -[5] .
Age, sex, immune status, preexisting conditions, the environment, nutrition and genetic load are some factors that influence susceptibility to cancer; genetic load being one of the most important ones for the interaction between etiological agents and subjects [3] [5] .
The presence of polymorphisms or variations in the base sequences of metabolic genes give rise to variable enzyme activity which leads to differing abilities in the metabolism of xenobiotics [6] , of which the glutathione S-transferase family (GST) is a part. It consists of several genes coding for a group of isozymes involved in Phase II metabolism, protecting the cell from oxidative injury [7] -[10] . The most studied GST subclasses in mammals are Mu (μ), Pi (π) and Theta (θ) [11] [12] .
The GSTM1 (μ) gene, located on chromosome 1p13.3, consists of 8 exons, with a length of 4.2 kb and 4 allelic variants: A (wild), B, C and 0 (zero). GSTM10 is the most frequent polymorphism, resulting in the loss of enzymatic activity [11] [13] -[15] .
The GSTT1 (θ) gene is located on chromosome 22p11.2; it consists of 6 exons and is flanked by two homologous regions HA3 and HA5. It has two allelic variants: wild GSTT1a and GSTT10, null. This polymorphism is due to a homologous recombination of the HA3 and HA5 regions resulting in a deletion of 5.4 kb [13] [15] -[17] .
GSTP1 gene (π) is located on chromosome 11q13; it consists of nine exons, with a length of 3.2 kb and has three allelic variants: wild allele GSTP1a, the polymorphic allele GSTP1b, located in exon 5 which is the result of the mutation of ATC (Ile) to GTC (Val) at codon 104. The third allele, GSTP1c, also polymorphic, has the same mutation at codon 104 as GSTP1b and, additionally, a second mutation in exon 6, consisting of a base substitution of GCG (Ala) to GTG (Val) at codon 113 [8] [15] [18] -[21] . The enzymes coded by these alleles have been implicated in the regulation of cell proliferation and apoptosis via direct interaction with c-Jun N-terminal kinase (JNK) [22] [23] .
Null or heterozygote genotypes of different classes of GSTs have been linked to susceptibility to developing lung, bladder, colon, skin, liver and breast cancer. The pharmacological interest of GSTs is their influence on the development of cancer on one hand, and on the response to therapy on the other [13] -[15] [19] [24] [25] . The aim of this study was to determine the frequency of M1, T1 and P1 polymorphisms in patients with breast cancer and to determine its association with the development of this malignancy.
2. Materials and Methods
2.1. Studied Group
This study was cross-sectional, descriptive and comparative in nature. The patient group consisted of 22 women with a clinical diagnosis of breast cancer at different stages of from the ISSEMyM State Oncology Center (Toluca, México). The control group was integrated by 30 healthy women in the same age range, native from the Toluca valley, Mexico. Participation was by invitation and voluntary; those who agreed to participate signed a letter of informed consent. A 3 mL sample of peripheral blood from each participant was drawn into a Vacutainer tube with heparin, which was kept refrigerated until processed.
2.2. DNA Extraction
DNA extraction was performed using the Quick-gDNAMiniPrep Kit (Zymo Research). The products were verified by horizontal electrophoresis in 1% agarose.
2.3. PCR for GSTT1 and GSTM1
Identification of polymorphisms of T1 and M1 was performed by multiplex PCR with CYP1A1 gene as control. The mixture had a final volume of 10 μL, containing 1 μL 5x PCR buffer (Promega), 0.6 μL of 25 mM MgCl2 (Promega), 1 μL 50 μM dNTP (Fermentas), 0.3 μL of molecular biology grade H2O, 0.1 μL 5 U/μLTaq Polymerase (Promega), 1 μL of DNA template and 1 μL of each primer CYP1A1-f, CYP1A1-r, GSTM1-f, GSTM1-r GSTT1-f, GSTT1-r, all primers had a concentration of 30 pm, Table 1. PCR conditions for these amplifications were: 5 minutes at 94˚C, denaturation 1 minute at 94˚C, alignment 1 minute at 59˚C, extension 1 minute at 72˚C and a final elongation of 5 minutes at 72˚C, for 35 cycles. PCR products were verified by horizontal electrophoresis using 1.5% agarose. The determination of the polymorphism of GSTT1 was based on the presence of a 480 bp band, corresponding to wild GSTTl, while its absence denoted a null GSTT1. Similarly, for GSTM1 the presence of a 215 bp band indicated wild GSTM1 while its absence implied null GSTM1. Finally, a 312 bp band, corresponding to CYP1A1, was always present and was employed as a PCR control gene [15] [25] -[27] .
2.4. PCR-RFLP for GSTP1
Identification of P1b (exon 5) and P1c (exon 6), was carried out in two separate PCRs, one for each polymorphism, both with a final volume of 25 μL in order to obtain a sufficient amount of product for subsequent enzymatic digestions. The mixture for the PCR reaction contained 2 μL of template DNA, 5 μL of 5x PCR buffer (Promega), 1.5 μL of 25 mM MgCl2 (Promega), 0.1 μL of 5 U/μLTaq Polymerase (Promega), 0.5 μL 50 μM dNTPs (Fermentas), 13.9 μL molecular biology grade H2O and 1 μL of each primer according to the gene to be amplified GSTP1b-f, GSTP1b-r GSTP1c-f or GSTP1c-r; all primers had a concentration of 30 pm, Table 1. For GSTP1c PCR, the conditions were the same as those used for GSTT1 and GSTM1, while conditions for GSTP1b PCR were: 5 minutes at 94˚C, denaturation 1 minute at 94˚C, alignment 1 minute at 62˚C, extension 1 minute at 72˚C and a final elongation of 5 minutes at 72˚C for a total of 35 cycles [28] .
For the identification of P1 polymorphisms, enzymatic digestions were carried out using BsmAI (Fermentas) for P1b (exon 5) and AciI (Fermentas) for P1c (exon 6). The digestion mixture consisted of 17 μL molecular biology grade H2O, 2 μL Fast-Digest Green buffer (Fermentas), 1 μL Fast-Digest Enzyme (Fermentas) and 10 μL PCR product DNA, for a total volume of 20 μL. Both digestion reactions were incubated at 37˚C for 5 minutes. The digestion products were verified by horizontal electrophoresis, using a 2% concentration of agarose. The identification of polymorphisms was based on the presence of DNA fragments of different sizes. For exon 5, 176 bp, 91 bp and 85 bp fragments correspond to heterozygote P1b while 91 bp and 85 bp P1b fragments correspond to homozygote and a 176 bp fragment corresponds to wild P1a [26] -[28] . Regarding exon 6 polymorphisms, the 332 bp fragment corresponds to homozygote P1c; three fragments, 332 bp, 174 bp and 158 bp correspond to heterozygote P1c and two fragments, 158 bp and 174 bp, to wild P1a [29] .

Table 1. Primers for GSTM1, GSTT1, CYP1A1 and GSTP1 genes.
2.5. Statistical Analysis
A X2 test was used to compare the frequencies of polymorphisms of GSTT1, GSTM1 and GSTP1 between the two groups, using the Sigma Stat 3.5 program.
3. Results
3.1. Socio-Demographic Attributes
The average age of patients with breast cancer was 49.4 years, ranging from 30 to 66. In the control group, the average age was 46 years, ranging from 30 to 65 years.
With respect to patients with breast cancer, the majority, 91.4%, had infiltrating ductal type and 8.6% were of the infiltrating lobular type.
3.2. Genotyping
Frequencies of polymorphisms obtained for the breast cancer group were: 77% wild GSTT1 and 33% null; 68% was wild GSTM1 and 32% null, while in the control group 60% was wild GSTT1 and 40% null; 37% was wild GSTM1 and 63% null. The statistical analysis showed a significant X2 difference in GSTM1 polymorphisms between the two groups. These results are presented in Figure 1.
The frequencies of GSTP1b polymorphisms (exon 5) in the breast cancer group were: 19% for wild P1a/P1a, 63% heterozygote P1a/P1b and 18% P1b/P1b homozygote; for GSTP1c (exon 6), 59% was wild P1a/P1a, 41% heterozygote P1a/P1c and 0% homozygote P1c/P1c. In the control group frequencies for GSTP1b (exon 5) were 27% wild P1a/P1a, 53% heterozygote P1a/P1b and 20% homozygote P1b/P1b; regarding GSTP1c (exon 6), 90% was wild P1a/P1a and 10% heterozygote P1a/P1c; homozygote P1c/P1c was not found. The X2 statistical analysis showed significant differences for heterozygote P1a/P1c and wild P1a/P1a GSTP1c polymorphisms, between the two groups.
Once genotype frequencies were individually determined, we proceeded to evaluate combinations of them. We found that for the breast cancer group, the most common genotypes were, firstly, wild GSTM1, wild GSTT1, homozygote (P1b/P1b) GSTP1 exon five and exon six wild GSTP1 (P1a/P1a) with 18% and secondly, with 15%, wild GSTM1, wild GSTT1, exon five heterozygote GSTP1 (P1a/P1b) and exon six heterozygote GSTP1 (P1a/P1c). While the two most common genotypes in the control group were wild GSTM1, wild GSTT1, exon five heterozygote GSTP1 (P1a/P1b) and exon six wild GSTP1 (P1a/P1a) with 20% and secondly, with 17%,
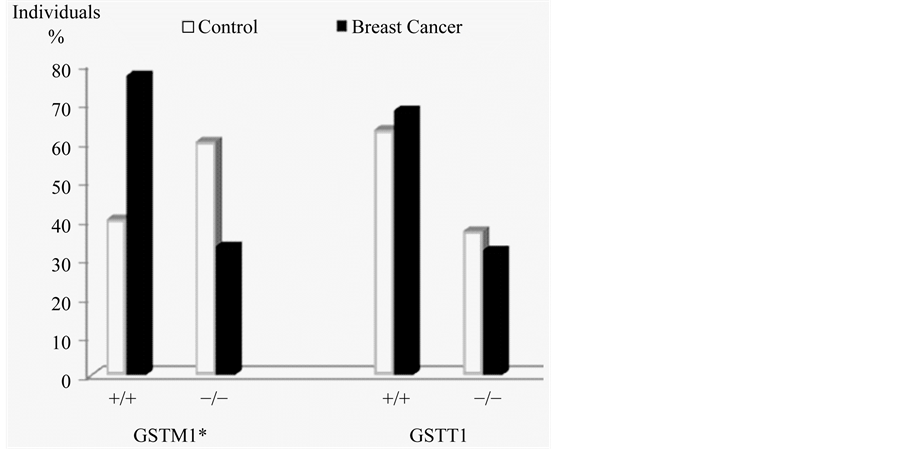
Figure 1. Frequencies of GSTM1 and GSTT1 polymorphisms. *Significant difference for GSTM1 between groups, p ≤ 0.05.
GSTM1 null, wild GSTT1, exon five heterozygote GSTP1 (P1a/P1b) and exon six wild GSTP1 (P1a/P1a). The details of these results are presented in Figure 2 and Table 2.
4. Discussion
Breast cancer is a disease of multifactorial etiology that is associated with age, for this reason the individuals in the control group for this study were within the age range of patients, to prevent age from being a misleading factor.
The presence of polymorphisms in susceptibility genes such as the GST family has been associated with an in-creased risk for developing bladder, head, larynx, breast, skin, colon, stomach, lung, and testicle cancer [20] [25] [30] -[32] .
Upon examination of our results for each gene individually, we found a significant difference of frequencies for GSTM1 between the two groups, since the wild type allele had a greater presence in the breast cancer group than in the control group, these results are similar to those obtained by Zheng et al. (2003), in a study of 326 patients with this neoplasm, finding an association between wild GSTM1 and alcohol consumption with susceptibility to breast cancer [33] . However, these results are contrary to expectations, since an individual with a GSTM1-null polymorphism, would be expected to have an increased susceptibility to cancer, as demonstrated by Garcia et al. (1999). Studying a group of 466 women with breast cancer, they conclude that GSTM1-null increases the risk of developing this malignancy [34] .
Regarding the frequencies of the GSTT1 genotypes, no significant difference between the groups was found, these results agree with those obtained in previous studies, one of them by Hashemi et al. (2012), on 134 patients with breast cancer and another by Vogl et al. (2004), on 2048 patients, no association between GSTT1 genotypes and the presence of breast cancer [35] [36] was found in either study. This is in contrast with the findings of Garcia et al. (1999), who in studying this gene concluded that GSTT1null genotype substantially increases the risk of developing this neoplasm [34] .
Sohail et al. (2013) conducted a study on 100 patients diagnosed with breast cancer and Lu et al. (2011) conducted a meta-analysis of 34,658 patients; both studies found an increased susceptibility of heterozygote genotypes for breast cancer [37] [38] . On the other side, studies by Vogl et al. (2004), Hashemi et al. (2012), as well as the present investigation found no relationship between GSTP1b genotypes with breast cancer [35] [36] .
Particularly striking is the absence of information in literature on the involvement of GSTP1 exon 6 polymorphisms with breast cancer. Our results show significant difference for this polymorphism between patients and the control group, from which we infer a possibility that the heterozygote polymorphism (P1a/P1c), may be associated with breast cancer. This seems inviting to continue studies on this gene.
Previous studies have explored susceptibility on a single gene, taken individually; joint participation, the way it occurs in vivo, has not been reported. Far from finding the variants corresponding to deletions (GSTM1-null
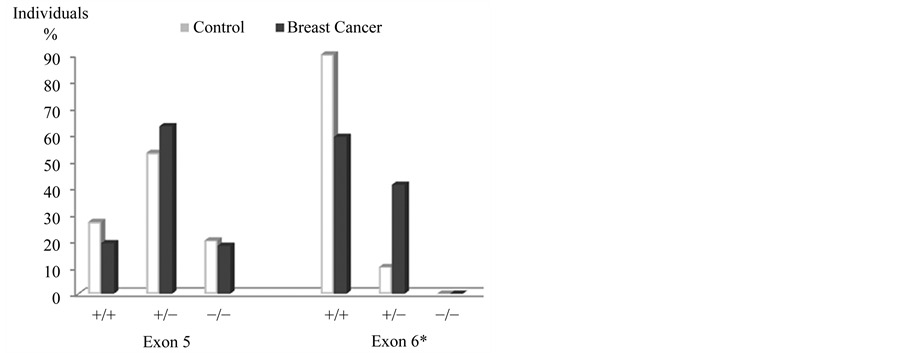
Figure 2. Frequencies of GSTP1 polymorphisms, exon five and six. *Significant differences in GSTP1, exon 6: wild P1a/P1a and heterozygous GSTP1b P1a/P1c, p ≤ 0.05.
Table 2. Frequencies for GSTM1, GSTT1 and GSTP1 genotypes by group.
and GSTT1-null), and mutations in exon 5 (GSTP1b) and exon 6 (GSTP1c), as could be expected in the group with breast cancer, we found that the genotype with GSTM1-wild, GSTT1-wild, exon five GSTP1 homozygote (P1b/P1b) and exon 6 (P1a/P1a) wild was the most frequent in the group with breast cancer, while the most frequent genotype in the control group was that with GSTM1-wild, GSTT1-wild, exon five GSTP1 heterozygote (P1a/P1b) and exon six (P1a/P1a) wild. Given the preferential presence of wild genotypes in both groups, our results do not allow us to infer that these polymorphisms confer an increased risk of developing breast cancer. Similar results were obtained by Vogl et al. (2004) [35] .
5. Conclusions
Studies such as this invite to document triggering or precipitating factors such as habits, habitat and work activities, among others, to have a more comprehensive picture of cancer development.
The different combinations of gene polymorphisms reported here showed no association with the development of breast cancer.
Acknowledgements
Extended to Dr. José Luis Barrera and Dr. Paula Cabrera ISSEMyM State Oncology Center and the Adolfo Lopez Mateos State Medical Center in Toluca, México, for their support in obtaining the samples. To all participants in this study. To Dr. Eduardo Ramirez San Juan for his advice on data analysis. This project was partially funded by the UAEMéx, agreement No. 3452/2013CHT.
References
- Menéndez, P., Villarejo, P., Padilla, D., et al. (2012) Epigenética y cáncer colorrectal. Cirugía Española, 90, 277-283. http://dx.doi.org/10.1016/j.ciresp.2011.11.006
- Meza, J., Montaño, L.A. and Aguayo, G.A. (2006) Bases moleculares del cáncer. Revista de Investigación Clínica, 58, 56-70.
- Romero, F.M., Arreygue, L.S., Hernández, P.O., et al. (2008) Frecuencia de factores de riesgo de cáncer de mama. Ginecología y Obstetricia de México, 76, 557-572.
- Mohar, A., Bargallo, E., Ramírez, M.T., et al. (2009) Recursos disponibles para el tratamiento del cáncer de mama en México. Salud Pública de México, 51, 263-269.
- Marie, K.F. (2009) Cáncer de mama en México: Una prioridad apremiante. Salud Pública de México, 52, 335-230.
- Brockmöller, J. (1996) Combined Analysis of Inhereted Polymorphisms in Arylamine N-Acetyltransferase-2, Glutatione S-Transferases M1 and T1, Microsomal Epoxidehydrolase and Cytochrome 450 Enzymes as Modulators of Bladder Cancer Risk. Cancer Research, 56, 3915-3925.
- Pavanello, S. and Clonfero, E. (2000) Indicatori biologici di rischio genotossico e polimorfismi metabolici. Medicina del Lavoro, 91, 431-469.
- Castillo, C.J., Contreras, S.C., Poblano, R.B., et al. (2007) Actividad en la enzima Glutatión S-transferasa T1 en floricultores expuestos a plaguicidas. Bioquímia, 32, 138.
- Guo, X., Zeng, Y., Deng, H., et al. (2010) Genetic Polymorphisms of CYP2E1, GSTP1, NQO1 and MPO and the Risk of Nasopharyngeal Carcinoma in a Human. Chinese Population of Southern China. Biomedical Central Research Notes, 3, 212-321.
- Kiran, B., Karkucak, M., Ozan, H., et al. (2010) GST (GSTM1, GSTT1 and GSTP1) Polymorphisms in the Genetic Susceptibility of Turkish Patients to Cervical Cancer. Journal Gynecologic Oncology, 21, 169-173. http://dx.doi.org/10.3802/jgo.2010.21.3.169
- Hayes, J.D., Fanagan, J.U. and Jowsey, I.R. (2005) Glutathione Transferases. Annual Review of Pharmacology and Toxicology, 45, 51-88. http://dx.doi.org/10.1146/annurev.pharmtox.45.120403.095857
- Sailaja, K., Surekha, D., Nageswara, D.R., et al. (2010) Association of the GSTP1 Gene (Ile105Val) Polymorphism with Chronic Myeloid Leukemia. Asian Pacific Organization for Cancer Prevention, 11, 461-464.
- Bolt, H.M. and Their, R. (2006) Relevance of the Deletion Polymorphisms of the Glutathione S-Transferases GSTT1 and GSTM1 in Pharmacology and Toxicology. Current Drug Metabolism, 7, 613-628. http://dx.doi.org/10.2174/138920006778017786
- Ruzzo, A., Graziano, F., Loupakis, F., et al. (2007) Perfil farmacogenético en los pacientes con cáncer colon-rectal avanzado tratados con quimioterapia FOLFOX-4 de primera línea. Journal of Clinical Oncology, 25, 1247-1254. http://dx.doi.org/10.1200/JCO.2006.08.1844
- Oliveira, A.L., Rodríguez, F.O., Santos, R.E., et al. (2010) GSTT1, GSTM1, and GSTP1 Polymorphisms and Chemotherapy Response in Locally Advanced Breast Cancer. Genetics and Molecular Research, 9, 1045-1053. http://dx.doi.org/10.4238/vol9-2gmr726
- Laffon, B.L., Pérez, C.B. and Méndez, F.J. (2004) Influencia de determinados polimorfismos de enzimas metabólicas en la genotoxicidad del estireno. Premio Alca Llíber de la Real Academia Nacional de Farmacia, 70, 95-123.
- Parl, F.F. (2005) Glutathione S-Transferase Genotypes and Cancer Risk. Cancer Letters, 221, 123-129.
- Ali-Osman, F., Akande, O., Antoun, G., Mao, J.X. and Buolamwini, J. (1997) Molecular Cloning, Characterization, and Expression in Escherichia coli of Full-Length cDNAs of Three Human Glutathione S-Transferase Pi Gene Variants. The Journal of Biological Chemistry, 272, 10004-10012. http://dx.doi.org/10.1074/jbc.272.15.10004
- Eaton, D. and Bammler, T. (1999) Concise Review of the Glutatione S-Transferases and Their Significance to Toxicology. Toxicological Sciences, 49, 156-164. http://dx.doi.org/10.1093/toxsci/49.2.156
- Young, W.A., Young, H.O., Grady, J., Salama, S.A. and Heo, M.Y. (2001) Usefulness of Genetic Susceptibility and Biomarkers for Evaluation of Environmental Health Risk. Environmental and Molecular Mutagenesis, 37, 215-225. http://dx.doi.org/10.1002/em.1030
- Custódio, A.C., Almeida, L.O., Pinto, G.R., et al. (2010) GSTP1 Ile105Val Polymorphism in Astrocytomas and Glioblastomas. Genetics and Molecular Research, 9, 2328-2334. http://dx.doi.org/10.4238/vol9-4gmr971
- Holley, S.L., Fryer, A.A., Haycock, J.W., et al. (2007) Differential Effects of Glutathione S-Transferase Pi (GSTP1) Haplotypes on Cell Proliferation and Apoptosis. Carcinogenesis, 28, 2268-2273. http://dx.doi.org/10.1093/carcin/bgm135
- Peklak-Scott, C., Smitherman, P.K., Morrow, C.S. and Townsend, A.J. (2008) Role of Glutathione S-Transferase P1-1 in the Cellular Detoxification of Cisplatin. Molecular Cancer Therapeutics, 7, 3247-3255. http://dx.doi.org/10.1158/1535-7163.MCT-08-0250
- Matheson, M.C., Stevenson, T., Akbarzadeh, S. and Propert, D.N. (2002) GSTT1 Null Genotype Increases Risk of Premenopausal Breast Cancer. Cancer Letters, 181, 73-79. http://dx.doi.org/10.1016/S0304-3835(02)00046-0
- García, A.D., Rubio, A.R., Cima, M.L., et al. (2007) Metabolic Gene Polymorphisms and Lung Cancer Risk. Mapfre Medicina, 18, 292-304.
- Wilson, M.H., Grant, P.J., Hardie, L.J. and Wild, C.P. (2000) Glutathione S-Transferase M1 Null Genotype Is Associated with a Decreased Risk of Myocardial Infarction. The Federation of American Societies for Experimental Biology Journal, 14, 791-796.
- Abdel-Rahman, S.Z., El-Zein, R.A., Anwar, W.A. and Au, W.W. (1996) A Multiplex PCR Procedure for Polymorphic Analisis of GSTM1 and GSTT1 Genes in Population Studies. Cancer Letters, 107, 229-233. http://dx.doi.org/10.1016/0304-3835(96)04832-X
- Mejia-Sanchez, F., Cadena-Castilo, J. and Sánchez-Meza, J.C. (2013) Development and Application in Mexican of a Method for the Identification of Polymorphisms of GSTP1. Journal of Medicine and Medical Sciences, 4, 287-290.
- Leite, J.L., Morari, C.E., Granja, F., et al. (2007) Influence of the Glutathione S-Transferase Gene Polymorphisms on the Susceptibility to Basal Cell Skin Carcinoma. Revista Médica de Chile, 135, 301-306. http://dx.doi.org/10.4067/S0034-98872007000300004
- Maugard, M.C., Charrier, J., Pitard, A., et al. (2001) Genetic Polymorphism at the Glutathione S-Tranferase (GST) P1 Locus Is a Breast Cancer Risk Modifier. International Journal of Cancer, 91, 334-339. http://dx.doi.org/10.1002/1097-0215(200002)9999:9999<::AID-IJC1057>3.0.CO;2-H
- Millikan, R., Pittman, G., Tse, C.K., et al. (2000) Glutathione S-Transferases M1, T1, and P1 and Breast Cancer. Cancer Epidemiology Biomarkers Prevention, 9, 567-573.
- Zhao, B. (2001) Dietary Isothiocyanates, Glutathione S-Transferase -M1, -T1 Polymorphisms and Lung Cancer Risk among Chinese Women in Singapore. Cancer Epidemiology, Biomarkers & Prevention, 10, 1063-1067.
- Zheng, T., Holford, T.R., Zahm, S.H., et al. (2003) Glutathione S-Transferase M1 and T1 Genetic Polymorphisms, Alcohol Consumption and Breast Cancer Risk. British Journal of Cancer, 88, 58-62. http://dx.doi.org/10.1038/sj.bjc.6600708
- García-Closas, M., Kelsey, T.K., Hankinson, E.S., et al. (1999) Glutathione S-Transferase Mu and Theta Polymorphisms and Breast Cancer Susceptibility. Journal of the National Cancer Institute, 91, 1960-1964. http://dx.doi.org/10.1093/jnci/91.22.1960
- Vogl, D.F., Taioli, E., Maugard, C., et al. (2004) Glutathione S-Transferases M1, T1, and P1 and Breast Cancer: A Pooled Analysis. Cancer Epidemiology, Biomarkers & Prevention, 13, 1473-1479.
- Hashemi, M., Eskandari-Nasab, E., Fazaeli, A., et al. (2012) Association between Polymorphisms of Glutathione STransferase Genes (GSTM1, GSTP1 and GSTT1) and Breast Cancer Risk in a Sample Iranian Population. Biomarkers in Medicine, 6, 797-803. http://dx.doi.org/10.2217/bmm.12.61
- Sohail, A., Kanwal, N., Ali, M., et al. (2013) Effects of Glutathione-S-Transferase Polymorphisms on the Risk of Breast Cancer: A Population-Based Case-Control Study in Pakistan. Environmental Toxicology and Pharmacology, 35, 143-153. http://dx.doi.org/10.1016/j.etap.2012.11.014
- Lu, S., Wang, Z., Cui, D., Liu, H. and Hao, X.S. (2011) Glutathione S-Transferase P1 Ile105Val Polymorphism and Breast Cancer Risk: A Meta-Analysis Involving 34,658 Subjects. Breast Cancer Research and Treatment, 125, 253- 259. http://dx.doi.org/10.1007/s10549-010-0969-x
NOTES

*Corresponding author.