Atmospheric and Climate Sciences
Vol. 2 No. 3 (2012) , Article ID: 21402 , 11 pages DOI:10.4236/acs.2012.23032
Effects of Quarry Activities on Some Selected Communities in the Lower Manya Krobo District of the Eastern Region of Ghana
1Department of Chemistry, University of Ghana, Accra, Ghana
2Environmental Science Programme, Faculty of Science, University of Ghana, Accra, Ghana
Email: vknartey@gmail.com, vknartey@ug.edu.gh
Received April 16, 2012; revised May 11, 2012; accepted May 19, 2012
Keywords: Quarries; Air Pollution; Dust; PM10; Dust Related Diseases; Water Related Diseases
ABSTRACT
Extraction of Limestone is an economically important and widespread activity in Ghana and has existed since historical times. However, in spite of its remarkable contribution towards economic development, some adverse impacts have been noticed, especially where extraction is carried out without proper planning and use of modern technology and scientific methods. We have carried out an assessment on the environmental effects of limestone quarrying on some communities in the Lower Manya Krobo District in the Eastern region of Ghana. Dust emission is one of the major effects of the practice of limestone extraction and as such, dust (PM10) sampling was conducted at the affected communities. Mean dry season results recorded in these communities stand at 125.0 µg/m3 for Bueryonye, 116.0 µg/m3 at Odugblase and 109.3 µg/m3 at Klo-Begoro. Oterkpolu community which served as the control recorded an average of 50.5 µg/m3. Average rainy season values recorded for the communities were 83.3 µg/m3 for Bueryonye, 113.1 µg/m3 at Odugblase and 74.4 µg/m3 at Klo-Begoro. The control community, Oterkpolu, had 43.3 µg/m3. These values are above the EPA, Ghana daily guideline level of 70 µg/m3 over a time-weighted average per 24 hours. Questionnaires administration and health records obtained from the health facilities in the communities revealed notable deteriorations in the health of the people as a result of the quarrying activities in the area. Notable among these is the prevalence of malaria though not related to dust emissions, it results from mosquitoes breeding in the stagnant pools of water found in pits created as a result of the mining activity. Other common health cases recorded were acute respiratory tract infection, ear and eye infections, cough and pneumonia.
1. Introduction
Quarrying is the process of obtaining quarry resources, usually rocks, found on or below the land surface [1]. The difference between mining and quarrying is that quarrying extracts nonmetallic rocks and aggregates while mining excavates the site for metallic mineral deposits. Some of the stones extracted are sandstone, limestone, perlite, marble, ironstone, slate, granite, rock salt and phosphate rock. The suitability of the stone for quarrying depends on its quality, the possibility of cheap and ready conveyance to a large market; and its inclination and depth below the surface.
The two principal branches of the industry are the dimension stone and crushed-stone quarrying. In the former, blocks or sheets of stone, such as marble, are extracted in different shapes and sizes for different purposes. In the crushed stone industry, granite, limestone, sandstone, or basaltic rocks are crushed for use principally as concrete aggregate or roadstone.
During the commissioning of the largest quarry in West Africa in the Brong-Ahafo Region of Ghana on 29 May 2009, the minister for Lands and Natural Resources reiterated that the Ministry was mindful of the legitimate concerns of the surrounding communities of the potential impacts usually associated with quarry operations such as blasting vibrations, noise, fly rocks, and dust among others [2].
A very high degree of respiratory morbidity is associated with this industry. Fine rock and mineral dust of many kinds have been shown to be carcinogenic when inhaled [3]. Control of particulate pollution is a matter of both health and aesthetics. Increasing attention is being paid to the impacts of dust on human health, as finer particles can be inhaled and breathed into the lungs and cause harm. It is generally recognised that dust up to 10 μm can be inhaled beyond the larynx and dust up to 4 μm can be breathed into the lungs.
Potential health impacts are almost exclusively linked to the presence of airborne dusts, in particular respirable particles, i.e. those that are less than 10 µm in diameter (also known as PM10), have the potential to affect human health, including effects on the respiratory and cardiovascular systems [1]. According to Banez, et al. [1] inhalation of dusts can cause “pneumoconiosis” which is a term that refers to a group of lung diseases.
Local communities can potentially be affected by dust up to 1 km from the source, although concerns about dust are most likely within 100 meters. Deposited dust gives rise to the greatest number of complaints to quarries from local communities, particularly for contrasting colours that are more noticeable on deposition. Settled particles may show up particularly on clean or polished surfaces such as cars, windows and window ledges, or surfaces that are usually expected to remain free from dust. The impacts from quarrying activities on the health of the people are quite significant as blasting vibrations have also resulted in cracks in several buildings exposing the occupants to danger. Other potential quarrying effects which are of concern to environmentalists include biodiversity loss, land degradation, nuisance effects, reduced plant growth, etc.
Particulates are the tiny solid or liquid particles that are suspended in air and which are usually individually invisible to the naked eyes [4]. The particulates include soot, smoke, ash from fuel (mainly coal) combustion, dust released during industrial processes like quarrying and other solids from accidental and deliberate burning of vegetation [3].
Quarrying generates a lot of particulate matter (dust) with diameter 1 - 75 µm (micron). Particles with aerodynamic diameters of less than 50 µm (termed Total Suspended Particulate matter, or TSP) can become suspended in the atmosphere, and those with aerodynamic diameters of less than 10 µm termed PM10 (inhalable particles) can be transported over long distances [5] and enter the human respiratory system [6,7].
TSP is the concentration of all particles in the atmosphere. Particles with aerodynamic diameters of less than 2.5 µm (respirable particles) are most effective at scattering light and have a great effect on visibility or visual intrusion [8], impairment and the earth’s radiation balance [9]. PM4 and PM2.5 inhaled penetrate deeply into the lungs and are capable of making their way to the air sacs deep within the lungs where they may be deposited and cause respiratory problems [10]. Air pollutants such as dust are unhealthy particles (solids, liquid gas mixtures) that are liable to harm both living and non-living things [11].
When air quality is monitored, the most common measure of the concentration of suspended particles is the PM index which is the amount of particulate matter that is present in a given volume of air [4]. In spite of the dangers of the dust emission resulting from limestone quarrying, there has not been any study on the effects of this activity on the environment and the health of the people living in this community. The objectives of this study are therefore to assess the environmental effects of limestone quarrying and its effects on the health status of the community. It is hoped that the results of this study will not only help environmental scientists but also politicians in policy formulation.
2. Materials and Methods
2.1. The Study Area
The study area is located in the Lower Manya Krobo District in the Eastern region of Ghana. The district is surrounded by Yilo Krobo in the west, Upper Manya Krobo in the north, Asuogyaman in the east and Dangme West in the south. Figure 1 shows the map of the study area carved from the map of Ghana and that of Lower Manya Krobo district while Table 1 shows the codes used in describing the sampling sites. Lower and Upper Manya Krobo districts which were created from the original Manya-Krobo District. A range of mountains called Yogwa stretches across the district west-east.
Lower Manya Krobo District covers a land area of 71787.350 acres or 29,053 hectres (CERGIS, UG, Legon). Lower Manya Krobo has a population of 30,655 [12]. The three communities in the study area had a total population of 696 (Bueryonye: 304, Odugblase: 188, Klo-Begoro: 204). The population includes 363 males and 233 females. The study area has 89 houses (Bueryonye: 32, Odugblase: 25, Klo-Begoro: 32) and 135 households (Bueryonye: 53, Odugblase: 37, Klo-Begoro: 45).
Three construction companies are located in the study area. These are A. J. Fanj, Kamsad and Love. The largest of the three, A. J. Fanj Company Limited, was contracted by Ghana Cement Factory (GHACEM) which was founded by the Government of Ghana in collaboration with Norcem A. S. of Norway, on 30 August 1967 to mine limestone on 17 November 2004.
2.2. Sampling Framework
Data on the impact of quarrying activities on the communities in the study area was collected between January and October, 2011 using two main methods which were branded as primary and secondary data collections.
Primary data collection: involved data collected by dust level measurement, PM10 in the study area.
Secondary data collection: data collected from health records in the clinics/hospital most patronized by the people. Social survey was also conducted by questionnaire administration in the communities sampled.
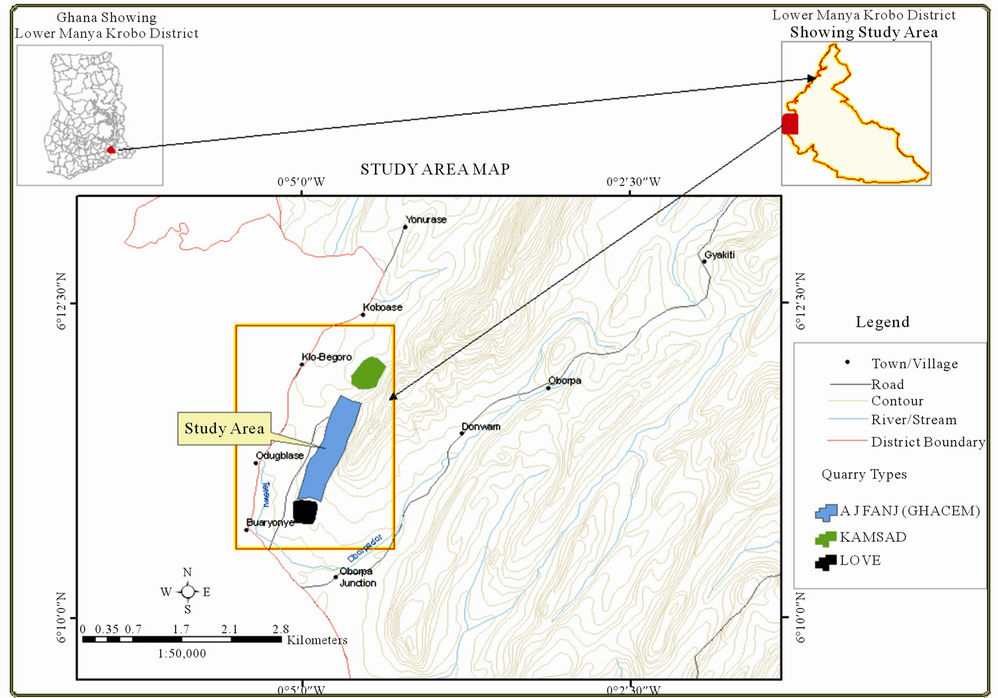
Figure 1. Map showing the study area (Source: CERGIS, UG, Legon).
2.3. Measurement of Particulate Matter (PM10)
PM10 (inhalable particles) was collected at three monitoring stations in January, April, June, August and October, 2011 in the study area. A fourth site located about one and half kilometres away from the quarries was used for comparative purposes. PM10 was sampled for a period of 24 hours using Mini Volume Portable Air Samplers to pump about 5 litres of air per minute. Flow rates of the systems were checked and recorded before and after sampling. The average flow rates were then determined.
2.4. PM10 Sampling Method
Filter papers of pore size less than 10 microns on which the particulates were collected were first stabilized in a desiccator for 24 hours. The stabilized papers were then pre-weighed with an electronic balance (AG104 Mettler Toledo) of milligram sensitivity (M1). The filter papers were then fitted into the PM10 samplers which were meant to draw air at a rate of 5.000 m3 per minute. Sampling was done for 24 hours after which loaded filters with PM10 were removed and stored in a dessicator to avoid absorption of moisture. This was later weighed (M2) and PM10 calculated using the relation:

PM10 = Particles with aerodynamic diameter of 10 microns;
M1 = Weight of filter paper before sampling (g);
M2 = Weight of filter paper after sampling (g);
FR = Average flow rate (l/min or m3/min);
T = Sampling duration in minutes.
2.5. Health Data Collection
Three health facilities mostly patronized by the indigenes in the study area were visited and the required data on Out Patient Morbidity was gathered. This data was collected so that the impact of quarrying activities on the health of the people could easily be analysed. The health facilities were Atua Government Hospital, Obenyemi and Oborpa Clinics.

Table 1. Definition of codes describing sampling sites in the study area.
2.6. Social Survey
Questionnaire was used to collect data from a fraction of the population under investigation and the responses were used to provide a quantitative description of the effects of the quarrying activities on the communities. The questionnaire was structured into four broad sections which sort for background information, knowledge about quarrying processes and implications, environmental issues and mitigation measures.
Households used for the study were obtained from a reconnaissance survey. The target person used in each house was the household head. A household was defined based on the 2000 Ghana Population and Housing Census household definition which stated a household as “people who eat from the same pot”. The questionnaire was administered to a cluster of three, four or five respondents at a time due to large number of questions, which comprised sixty questions in all.
3. Results and Discussion
Results of the PM10 values recorded for the sampling sites are shown in Table 2 and it can be observed that, N1
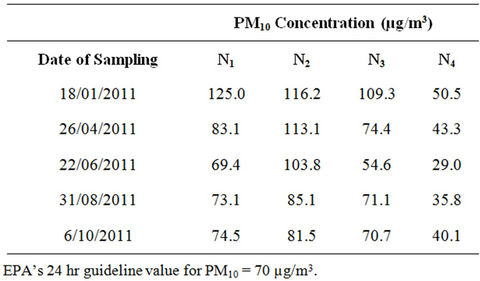
Table 2. Comparative results of PM10 concentration from January to October.
recorded 125.0 µg/m3 as the highest level and 69.4 µg/m3 as the lowest, N2 had 116.2 µg/m3 as the highest and 67.5 µg/m3 as the lowest with N3 recording 109.3 µg/m3 as the highest and 54.6 µg/m3 as the lowest. The highest concentration of 125.0 µg/m3 was recorded in January whilst the lowest value of 54.6 µg/m3 was recorded in June. Oterkpolu, N4 the control site had 54.5 µg/m3 as the highest in January as against 29.0 µg/m3 as the lowest in June. On the whole, the dry season values are higher than the wet or rainy season results (Figure 2). Also, areas closer to the quarries recorded higher results than those farther away. This is evident from the fact that, Bueryonye, N1 and Odugblase, N2 have recorded higher values both in January and June than Klo-Begoro, N3 because they are closer to quarries operated by Love and A. J. Fanj (GHACEM) companies respectively (Figure 1). Klo-Begoro, N3 showed lower results than N1 and N2 since the nearest quarry to this community which is operated by Kasad is not as close as observed for the other two cases.

Figure 2. Comparative results of PM10 levels from January to October (Source: Field Data).
4. Environmental Impacts of Quarrying Activities
A survey of the communities and the quarries revealed worrying issues concerning the impacts of the mining activity on the environment which included impact on buildings, farmlands, crops and water systems. Several buildings were observed to have developed different degrees of cracks with some near collapse. These cracks were basically due to strong vibrations coming from rock blasting. Farmlands are usually lost to flood waters which are water pumped from the quarry pits and runoffs. Figure 3 shows a photograph of one such river system that has been affected by water pumped from mine pits.
Dust from rock processing and unpaved (dusty) roads have settled on crops and other plants as a result of sedimentation. High concentrations of dust on the plants result in poor plant performance and yield. Figure 4 shows crops on farmlands near (a) and far away (b) to a quarry site.
5. Health Impact of Quarrying Activities
It has not been possible to separate the health records of the people from the control community, N4 from those of the study area, N1, N2 and N3 because all residents attend the same health facilities. The study could therefore not compare the health records of the two sets of communities. This notwithstanding, responses from the communities which was based on health status before and after the establishment of the quarrying facilities offer strong grounds for attributing the deterioration in the people’s health to the impact of the quarrying activities and this is supported by the observed increase in dust related diseases from the time of start of quarrying activity.
It could be observed that health records obtained from the health centres have shown a noticeable increase in dust related diseases in the study area. Figure 5 has shown a hike in dust related diseases from 2005 onwards when the GHACEM quarrying was fully operational. Ear infection and acute respiratory tract infection (ATI) are

Figure 3. River Tetewu polluted by quarry run-off.
 (a)
(a) (b)
(b)
Figure 4. The effect of dust from mining activities on crops in the study area. (a) Crops on farmland close to a quarry; (b) Crops on farmland far away from a quarry.
still on the increase. Cases of cough are also slightly on the increase with pneumonia and eye infections noticeable among the people.
Water related sicknesses, noticeably malaria infection rose significantly from 2005 onwards and cases of diarrhoea also rose slightly. Schistosomiasis and typhoid infections were rather insignificant as can be seen in Figure 6.
There is an observed rise in cough, pneumonia, chest pains, common cold, eye problems and other respiratory tract infections (ATI) like catarrh, sore throat from 2005 to 2010 at Oborpa clinic (Figure 7). Headache, eye infection, ear infection and asthma have also increased significantly as portrayed in Figure 7. The increase in respiratory tract infection from 2005 can be attributed to patients suffering from the effects of quarry dust.
Records of some water-related or borne diseases obtained from Oborpa clinic show an upsurge in malaria cases from 2005 to 2010 (Figure 8). Diarrhoea cases also increased gradually since 2005. Cholera cases are rather low with no records of Schistosomiasis and dysentery during the period. The high malaria infection could be attributed to flooded lands as a result of quarrying leading to mosquito breeding in stagnant waters created by the quarrying activities.
All dust related diseases have risen sharply from 2005 onwards. The most observable diseases are cough, chest pains, common cold headache, pneumonia, asthma, ATI and eye infection which rose steadily from 2005 to date as can be seen in Figure 9. The rise in ear infection may be due to the high levels of noise from machinery and trucks especially among quarry workers.
As can be seen from Figure 10, there has been a steady rise in malaria and diarrhoea cases since 2005 to 2010 from the records obtained from Obenyemiclinic. Typhoid, cholera, schistosomiasis and dysentery have not been noticed among the water related or borne diseases at this clinic. The upsurge in malaria and diarrhoea cases could be attributed to flooding of lands which often create stagnant waters which serve as mosquito breeding grounds.
6. Social Survey on Impact of Quarrying Activities on the Health Status of Communities
The questionnaire sort to gather information on the health health status respectively. The apparently poor health status of the people could be attributed to the high concentration of particulate matter (dust) generated from the quarries, drinking of unclean rain water and perhaps status of the residents before and after the inception of the quarrying activities. These residents are engaged in farming or other forms of livelihood with some working

Figure 5. Atua government hospital out-patient morbidity returns (dust related) (Source: Atua Government Hospital).
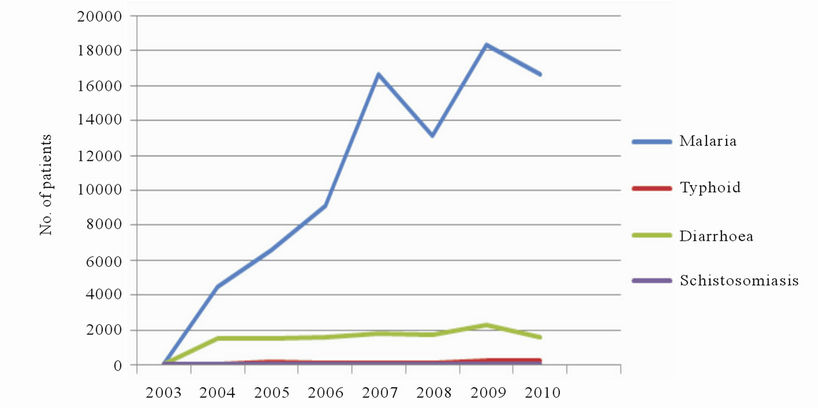
Figure 6. Atua government hospital out-patient morbidity returns (water related/borne).
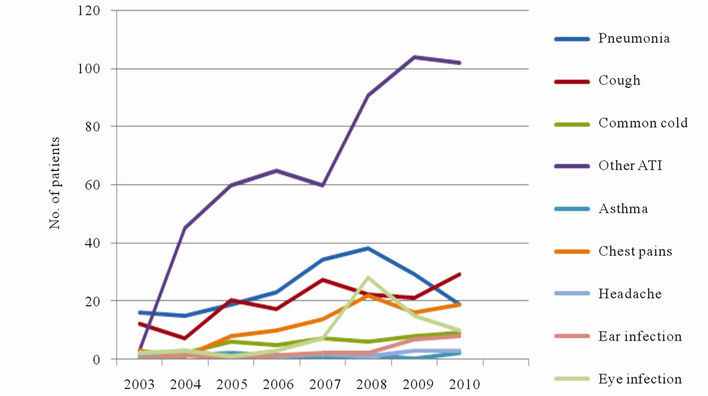
Figure 7. Oborpa clinic out-patient morbidity returns (dust related) (Source: Oborpa Clinic).
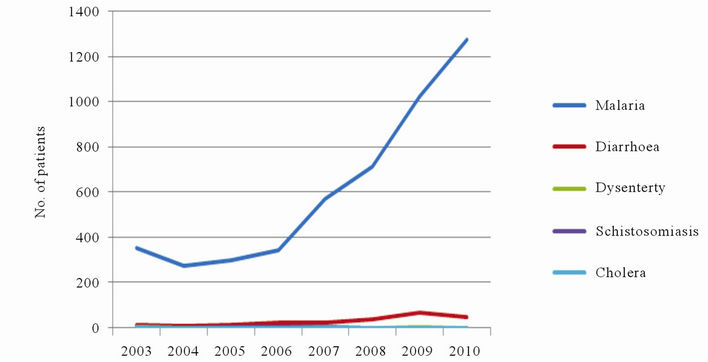
Figure 8. Oborpa clinic out-patient morbidity returns (water related) (Source: Oborpa Clinic).

Figure 9. Obenyemi clinic out-patient morbidity returns (dust related).
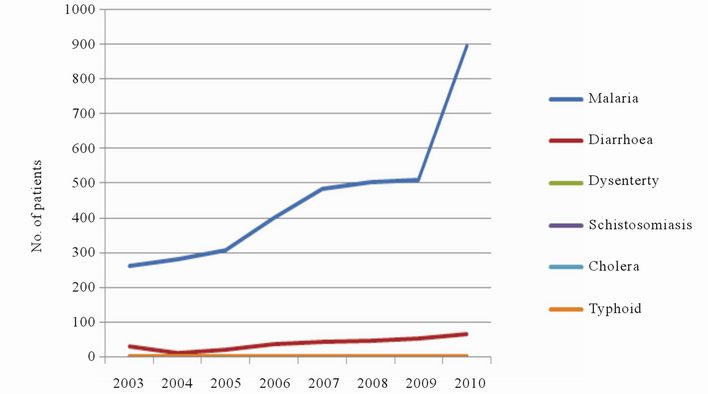
Figure 10. Obenyemi clinic out-patient morbidity returns (water related) (Source: Obenyemi Clinic).
directly at the quarries. Figure 11 shows the results of the responses gathered from this survey where 75% of the respondents stated they had excellent health and 25% had a very good health status before quarrying began. No respondent, 0%, had good, fair or poor health condition before the start of the quarry activities. The health status of the people could be generally classified as excellent before the start of quarrying.
The respondents indicating that all of them had very good or excellent conditions of health before the start of quarrying activity show some possibility of bias. Nonetheless, it is still fair to accept their stated current condition of health given the observations made from the health data collected from the health facilities after the start of the quarrying activity.
From Figure 12, it would be observed that the health status of the people has declined. Only 10% of the respondents maintained their excellent health status, 0% responded of having very good health status while 5% responded of having good health status. A large percentage of 40% and 45% had reported of having fair and poor floods providing conducive atmosphere for disease causing organisms. On the whole, the present health status of the people can only be judged as fair.
As can be seen from Figure 13, there has been a significant rise in the percentages of respondents who suffer currently from the dust related diseases. Notable among these are cases such as cough where 33.3% of respondents stated they suffered from the sickness but this number rose significantly to 100% of respondents after the inception of the quarry activity. Other significant cases that have seen major increase in percentage of sufferers are catarrh, asthma, headache, eye problems and spitting of phlegm.
In Figure 14 illustrates the effect of water related diseases on respondents. Significant changes have been noticed in cases where, 40% and 5% of the respondents suffered from malaria and diarrhoea only; 20% had malaria and cholera; 35% had malaria, typhoid and diarrhea; nobody (0%) was infected with malaria, typhoid and diarrhea and then malaria, cholera and diarrhoea. During quarrying 3% and 0% suffered from only malaria and diarrhoea; 16.7% had malaria and diarrhea; 33.3% had malaria and cholera, 25% had malaria, typhoid and diarrhoea. Twenty percent (20%) were infected with malaria, cholera and diarrhoea. According to Figure 14, 95% of the respondents suffered from malaria where as 100% suffered from the same disease during quarrying. The rise could be attributed to more mosquitoes due to the inundated farmlands.
Figure 15 shows the comparative levels of the health status of the respondents before and after the inception of the quarrying activities. As is evident from Figure 15, health status before quarrying which were deemed excellent (75% of respondents) decreased to (10% of respondents) after the inception of quarrying while to fair health condition has been reported by 40% of respondents with 45% reporting of having poor health condition which was recorded for 0% of respondents before the starting of quarrying. Obviously the health status of the average respondent suffered some deterioration as a result of the limestone extraction which is impacting negatively on the people.
7. Conclusions
Limestone quarrying has brought about both benefits and costs to Lower Manya Krobo District. The benefits include employment creation, infrastructural development, and revenue generation for the District Assembly. The devastating effects of limestone mining include the lowering of water tables, creation of labour bottlenecks for
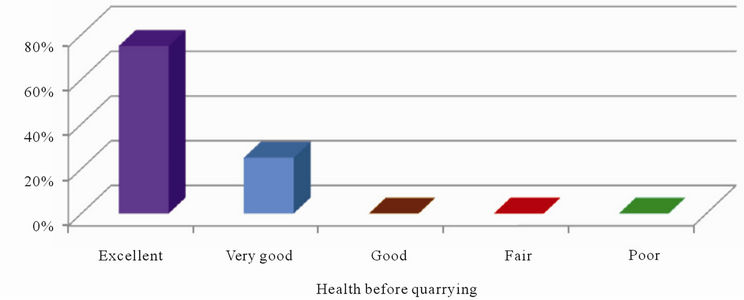
Figure 11. Health status of the respondents before quarrying (Source: Field Data (Questionnaire)).

Figure 12. Health status of respondents after inception of quarrying activities (Source: Field Data (Questionnaire)).

Figure 13. Percentage of respondents suffering from dust related diseases before and during Quarrying (Source: Field Data (Questionnaire)).
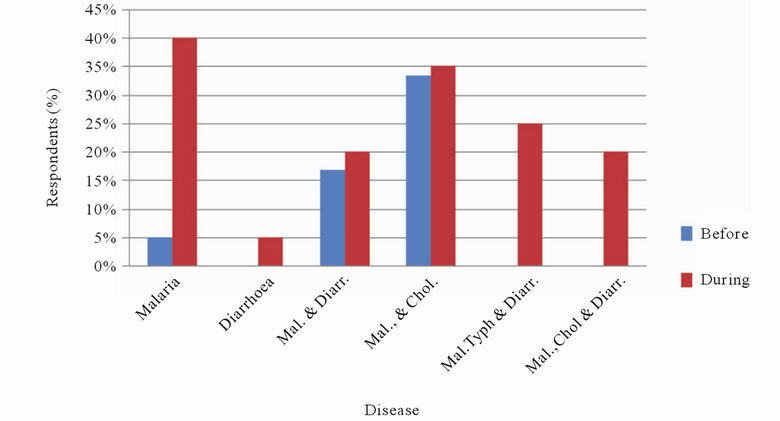
Figure 14. Percentage of respondents suffering from water related diseases before and during quarrying (Source: Field Data (Questionnaire)).
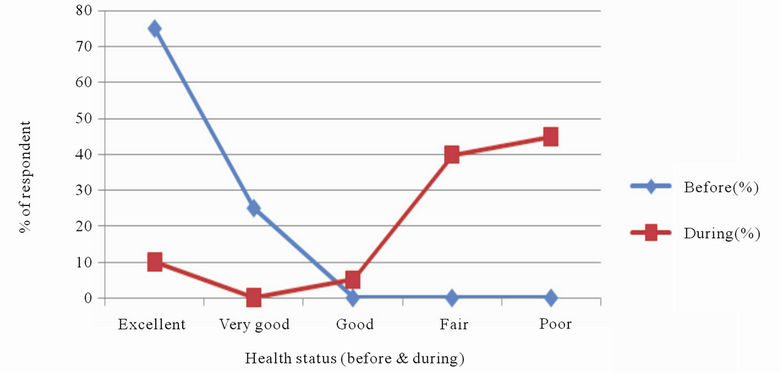
Figure 15. Comparative health status before and during quarrying (Source: Field Data (Questionnaire)).
peasant agriculture, encroachment onto agricultural land, destruction of buildings due to cracks, pollution of rivers, loss of biodiversity, destruction of crops and unclean rain water harvested from roofs. Inhalation of dust resulting in respiratory tract infections and habitat destruction also add to the list of the negative effects of limestone quarrying in the Lower Manya Krobo District.
With reference to Ghana EPA [13] standard for PM10 the communities in the study area recorded daily concentration that exceeds the daily minimum level of 70 µg/m3 over a time-weighted average per 24 hours. Out of the fifteen readings taken in the study area, 86.7% were above the 70 µg/m3 set by EPA, Ghana. Dust related infections have doubled according to data recorded from questionnaires (Figure 14). Air pollution due to quarry dust is very high during the dry season as PM10 concentration was highest in January. Dust suppression measures must, therefore, be effectively implemented during the dry season.
Trend analysis performed based on health data, PM10 sampling, observation and questionnaire administration really suggest that favourable conditions for infections due to dust emission, floods and other quarrying impacts are responsible for the persistence of the diseases in the communities. This assertion is so because people in the study area in the Lower Manya Krobo District live at the risk of the diverse infections in performing their daily activities which include farming, quarrying, trading and performing of domestic chores. Health data has also supported the deadly effects of quarrying activities on the people in the three communities. There has been a sharp rise in dust and water related or borne diseases from 2005 when limestone mining started in the community. Malaria is the most contracted water related disease whilst cough (100%), catarrh (75%), headache (95%), asthma (65%) and frequent issue of phlegm (75%) are the major dust related ailments suffered from; where the percentages were based upon the responses from respondents to the questionnaires administered.
REFERENCES
- J. Banez, S. Mae Ajaon, J. R. Bilolo and J. M. Dailyn, “Quarrying and Its Environmental Effects,” 2010. http:www.scribd.com
- Ghanaian Chronicle, “B/A Makes Strides in Exploiting Natural Resources, as Veep Commissions the Biggest Quarry Plant in W/A at Wenchi,” Ghanaian Chronicle, 29 May 2009.
- W. C. Montgomery, “Environmental Geology,” 3rd Edition, Wm C. Brown Publishers, Dubuque, 1992.
- C. Baird, “Environmental Chemistry,” 2nd Edition, W. H. Freeman and Company, New York, 1992.
- L. Nickling and A. Boas, “Influence of Vegetation Cover on Sand Transport by Wind: Field Studies at Owens Lake,” California Earth Surface Processes and Landforms, Vol. 23, No. 1, 1998, pp. 69-82.
- B. G. Ferris, F. E. Speizer and J. D. Spengler, “Effects of Sulphur Oxides and Respirable Particles on Human Health: Methodology and Demography of Populations in Study,” American Review of Respiratory Disease, Vol. 120, No. 4, 1979, pp. 767-779.
- F. J. Miller, D. E. Gardner, J. A. Graham, R. E. Lee, W. E. Wilson and J. D. Bachmann, “Size Considerations for Establishing a Standard for Inhalable Particles,” Journal of the Air Pollution Control Association, Vol. 29, No. 6, 1979, pp. 610-615. doi:10.1080/00022470.1979.10470831
- W. C. Malm, “Considerations in the Measurement of Visibility,” Journal of the Air Pollution Control Association, Vol. 29, No. 10, 1979, pp. 1742-1752.
- R. J. Charlson, S. E. Schwartz, J. M. Hales, R. D. Cess, J. A. Coakley, J. E. Hansen and D. J. Hofmann, “Climate Forcing by Anthropogenic Aerosols,” Science, Vol. 255, No. 5043, 1992, pp. 423-430. doi:10.1126/science.255.5043.423
- Z. Zheng, K. L. Dionisio, R. E. Arku, A. Quaye, A. F. Hughes and J. Vallarino, “Household and Community Poverty, Biomass Use and Air Pollution in Accra, Ghana,” Proceedings of the National Academy of Sciences of the United States of America, Washington DC, 20 June 2011.
- D. E. Ward, J. Peterson and W. M. Hao, “An Inventory of Particulate Matter and Air Toxic Emissions from Prescribed Fires in the USA for 1989,” 86th Annual Meeting and Exhibition of Air and Waste Management Association, Denver, 13-18 June 1993, p. 19.
- Population and Housing Census, “Ghana Statistical Service Report,” PHC, 2010.
- Environmental Protection Agency, “Ghana Environmental Protection Agency State of the environment Report,” SOE, 2004.