Vol.1, No.3, 164-166 (2011)
doi:10.4236/ojpm.2011.13021
C
opyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/OJPM/
Open Journal of Preventive Medicine
Examine a dynamic of mother-to-child transmission of
HIV in the population-based surveys
Rathavuth Hong1*, Rathnita Them2
1Measure Demographic and Health Survey, ICF Macro, Calverton, USA;
*Corresponding Aut h o r : rhong@icfi.com
2College of Health and Human Services, George Mason University, Fairfax, USA.
Received 29 June 2011; revised 23 September 2011; accepted 14 October 2011.
ABSTRACT
The main source of HIV infection in young chil-
dren is of their mothers, during pregnancy, la-
bor and delivery, or by breastfeeding. The rate
of HIV transmission from infected mothers to
their newborn children varies from 15% to 40%
with one-thirds of these infections was through
breastfeeding. This paper examines cross-sec-
tional population-based survey data of HIV test
results among mothers and their children in
Uganda, Swaziland to estimates of mother-to-
child transmission (MTCT) rate of HIV infection.
The prevalence of HIV among women aged 15 -
49 who gave birth in the past 5 years in Uganda
is 7.3%, and in Swaziland is 37.9%. The HIV
prevalence of children who mothers were HIV
positive were very similar: 10.3% in Uganda and
11.5 % in Swaziland. This association represents
the crude rate of MTCT in these two countries at
the time of the survey. Presence of HIV antibody
in early age (0 - 11 months) is due to both true
infection and passive antibody from mothers.
The seroconversion dropped nearly half in the
second year of age which was likely that many
of these children died before reaching the age
of 12 - 23 months and passive antibody were
gradually cleared at this point. This analysis
demonstrated that cross-sectional data can be
used to estimate indirectly the magnitude and
dynamic of MTCT.
Keywords: HIV/AIDS; Mother-to-Child;
Transmiss ion; Demographic and Health Survey;
Uganda; Swaziland
1. INTRODUCTION
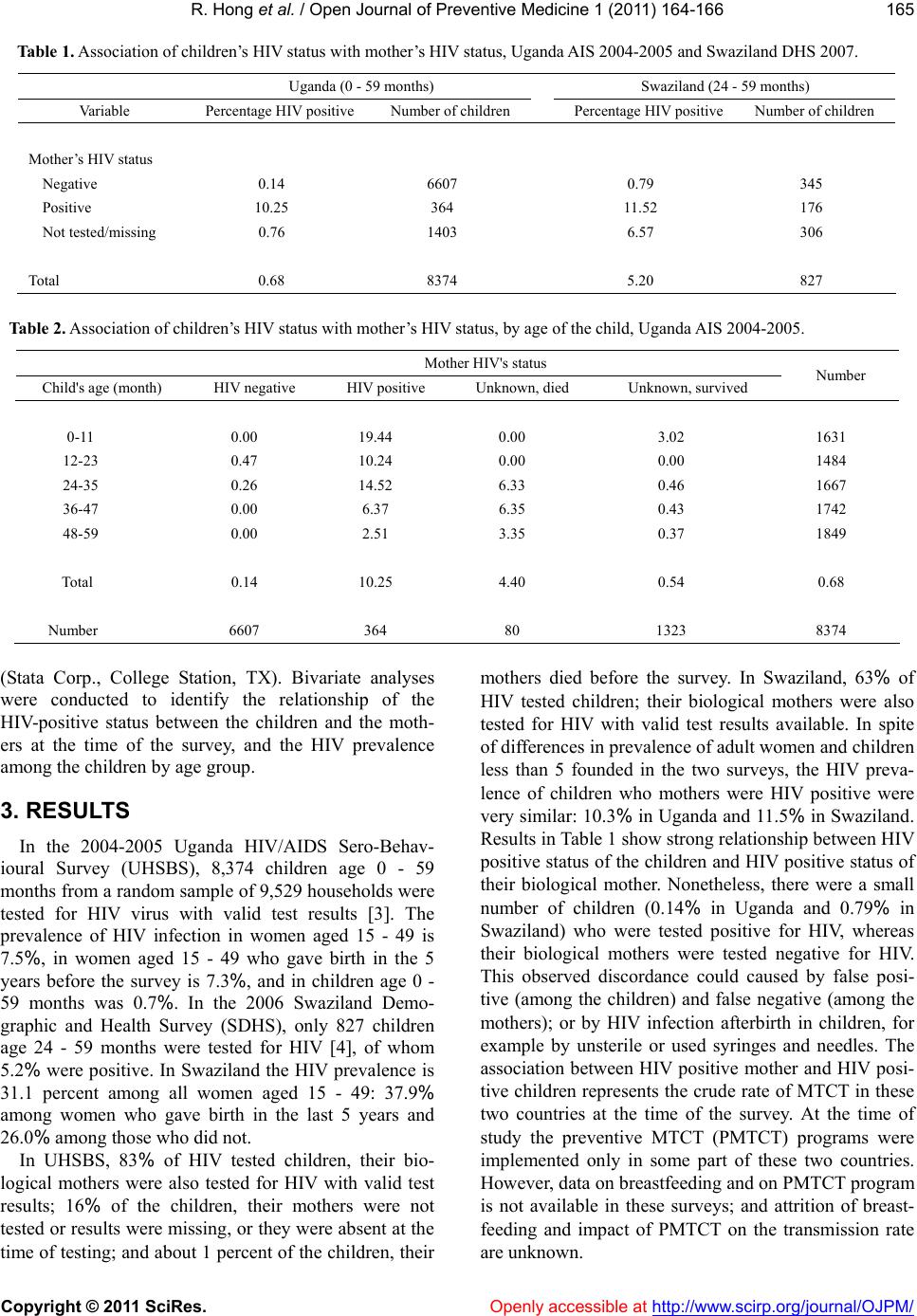
The source of HIV infection in young children is
overwhelming of their mothers, during pregnancy, labor
and delivery, o r by breastfeeding. In the region where the
rate of HIV infection among pregnant women is very high,
for example exceeds 35%, HIV/AIDS infection contrib-
utes to as high as 42% of child mortality [1]. In develop-
ing countries, the rate of HIV transmission from infected
mothers to their newborn children varies from study to
study, and is estimated from about 15% to 40%. Among
those children who are infected HIV through the trans-
mission from their mothers, one-third received the virus
through breastfeeding [2].
We examine whether data on HIV testing in the
cross-sectional data such as population-based survey
provide good estimates of mother-to-child transmission
(MTCT) rate of HIV infection. The testing procedure
used two ELISAs parallel testing algorithm according to
WHO testing algorithm. All discordant samples were
subjected to a second round of testing using both tests.
The discordances from the second round are “indeter-
minate” and were then subjected to a third confirmatory
Western-Blot test. The Western-Blot result was consid-
ered final for the indeterminate samples.
2. METHODS
2.1. Data
We used data from the 2004-2005 Uganda HIV/AIDS
Sero Behavioural Survey (UHSBS) and from the 2006
Swaziland Demographic and Health Survey (SDHS).
These are national representative household surveys that
include HIV testing among children and adults. UHSBS
tested HIV among 8,374 children aged 0 - 59 months,
10,227 women age 15 - 59 years, and 8,298 men age 15 -
59 years in a random sample of 9,529 households across
the country. Information on birth history from the women
questionnaire was used to establish the link between
mothers and her biological children for the analysis of
this study.
2.2. Statistical Methods
Statistical analysis was performed using Stata 10.0