B. MARIJANA ET AL. 705
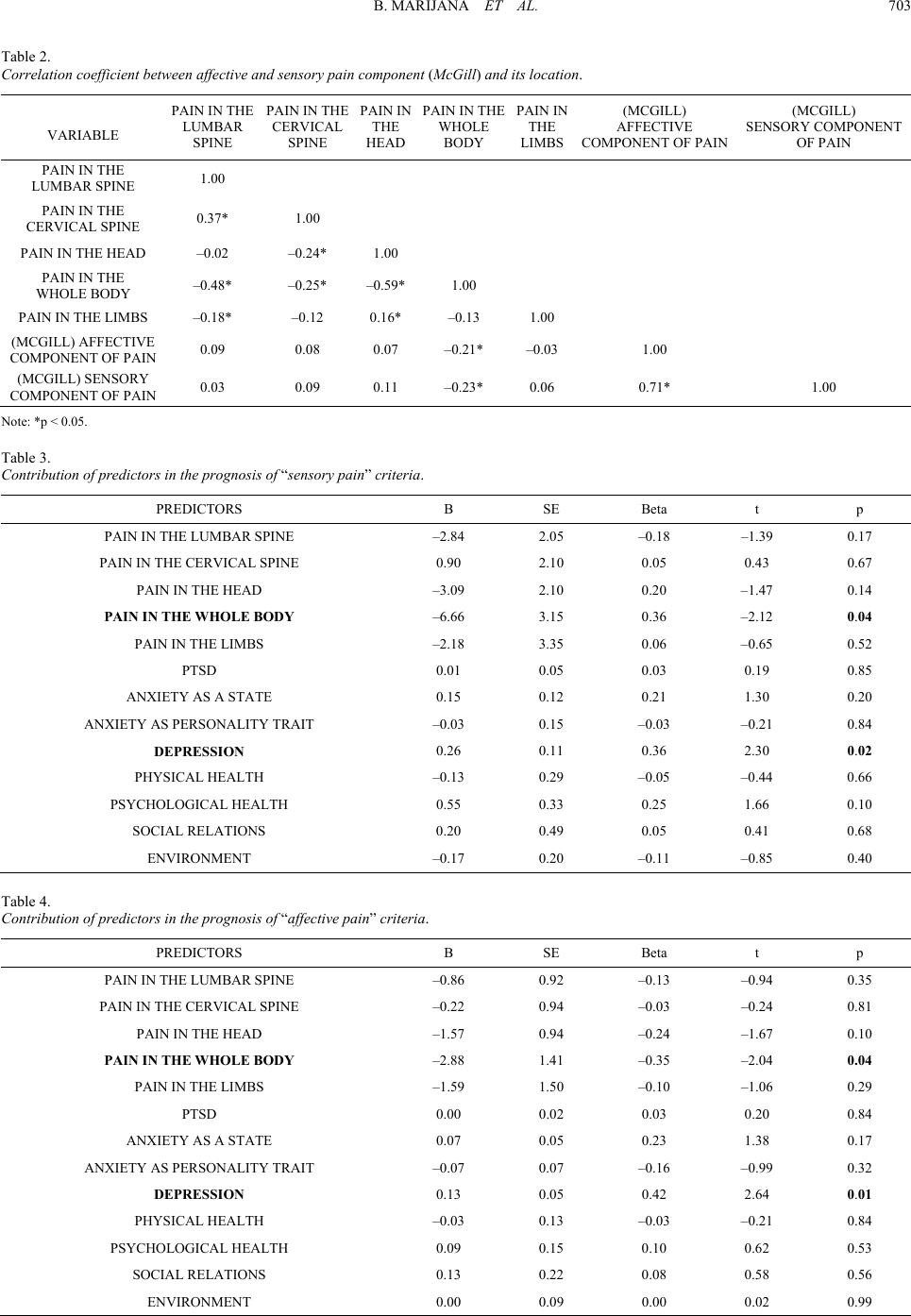
anxiety as a personality trait and as a state are of particular
interest, and so are the PTSD levels and sensory and affective
components of pain. The importance of the intensity of depress-
sion has been noticed, especially for its significantly positive
correlation between pain experience and PTSD level.
There is significant relation between posttraumatic stress
disorder and chronic pain syndromes, which in clinical practice
occur together with negative interaction in terms of the course,
outcome, and treatment of each individual disorder. It is as-
sumed that when compared with acute stressful stimulus the
chronic stress disorder has similar pattern of development as
does the chronic neuropathic pain in relation to peripheral
painful stimulus. The study has confirmed the assumption about
the relation between PTSD and chronic pain.
References
Arnow, B. A., Hunkeler, E. M., & Blasey C. M. (2006). Comorbid
depression, chronic pain, and disability in primary care. Psychosomatic
Medicine, 68, 262-268. doi:10.1097/01.psy.0000204851.15499.fc
Beckham, J. C., Moore, S. D., Feldman, M. E, Hertzberg, M. A., Kirby,
A. C, & Fairbank, J. A. (1998). Health status, somatization, and se-
verity of posttraumatic stress disorder in Vietnam combat veterans
with posttraumatic stress disorder. American Journal of Psychiatry,
155, 1565-1569.
Bouckoms, A. J. (1999). Chronic pain: Neuropsychopharmacology and
adjunctive psychiatric treatment. In J. Rundel, & M. Wise (Eds.),
Textbook of consultation-liaison psychiatry (Vol. 41, pp. 1006-1036).
Washington: American Psychiatric Press Inc.
Bryant, R. A., Marosszeky, J. E, Crooks, J., Baguley, I. J., & Gurka, J.
A. (1999). Interaction of posttraumatic stress disorder and chronic
pain following traumatic brain injury. Journal of Head Trauma Re-
habilitation, 14, 588-594. doi:10.1097/00001199-199912000-00007
Clark, M. R., & Treisman, G. J. (1991). Pain and depression—An Inter-
disciplinary patient-centered therapy. Advances in Psychosomatic
Medicine, 25, 78-88.
Davidson, J. T., Stein, D. J., Shalev, A. J., & Yehuda, R. (2004). Post-
traumatic stress disorder: Acquisition, recognition, course, and
treatment. Journal of Neuropsychiatry and Clinical Neurosciences,
16, 135-147. doi:10.1176/appi.neuropsych.16.2.135
Defrin, R., Ginzburg, K., Solomon, Z., Polad, E., Bloch, M., Govezen-
sky, M., & Schreiber, S. (2008). Quantitative testing of pain percep-
tion in subjects with PTSD—Implications for the mechanism of the
coexistence between PTSD and chronic pain. Pain, 138, 450-459.
doi:10.1016/j.pain.2008.05.006
Diatchenko, L., Slade, G. D., Nackley, A. G., Bhalang, K., Sigurdsson,
A., Belfer, I., Goldman, D., Xu, K., Shabalina, S. A., Shagin, D.,
Max, M. B., Makarov, S. S., & Maixner, W. (2005). Genetic basis
for individual variations in pain perception and the development of a
chronic pain condition. Human Molecular Genetics, 14, 135-143.
doi:10.1093/hmg/ddi013
Fedoroff, I. C., Taylor, S., Asmundson, G. J. G., & Koch, W., J. (2000).
Cognitive factors in traumatic stress reactions: Predicting PTSD
symptoms from anxiety sensitivity and beliefs about harmful events.
Behavioural and Cognitive Psych oth era py, 28, 5-15.
Geuze, E., Westenberg, H. G., Jochims, A., De Kloet, C. S., Bohus, M.,
Vermetten, E., & Schmahl, C. (2007). Altered pain processing in vet-
erans with posttraumatic stress disorder. Archives of General Psy-
chiatry, 64, 76-85. doi:10.1001/archpsyc.64.1.76
Harris, I. A., Young, J. M., Rae, H., Jalaludin, B. B., & Solomon, M. J.
(2007). Factors associated with back pain after physical injury: A
survey of consecutive major trauma patients. Spine, 32, 1561-1565.
doi:10.1097/BRS.0b013e318067dce8
Keefe, F. J., Rumble, M. E., Scipio, C. D., Giordano, L. A., & Perri, L.
M. (2004). Psychological aspects of persistent pain: Current state of
the science—Invited comentary. The Journal of Pain, 5, 195-211.
doi:10.1016/j.jpain.2004.02.576
Kessler, R. C., Zhao, S., Katz, S. J. (1999). Past-year use of outpatient
services for psychiatric problems in the National Co-Morbidity Sur-
vey. American Journal of Ps yc hi at r y, 156, 115-123.
Lanius, R. A., Williamson, P. C., Hopper, J., Densmore, M., Boksman,
K., Gupta, M. A., Neufeld, R. W., Gati, J. S., & Menon, R. S. (2003).
Recall of emotional states in posttraumatic stress disorder: An fMRI
investigation. Biol o g i c a l Psychiatry, 53, 204-210.
doi:10.1016/S0006-3223(02)01466-X
Leo, R. J. (2005). Chronic pain and comobid depression. Current
Treatment Options in Neurology, 7 , 403-412.
doi:10.1007/s11940-005-0032-0
Maruta, T., Swanson, D. W., & Swenson, W. M. (1976). Pain as a
psychiatric symptom: Comparison between low back pain and de-
pression. Psychosom, 17, 123-127.
McWilliams, L. A., Cox, B. J., Enns, M. W. (2003) Mood and anxiety
disorders associated with chronic pain: An examination in a nation-
ally representative sample. Pain, 106, 127-133.
doi:10.1016/S0304-3959(03)00301-4
Melzack, R., & Casey, K. (1968). The skin senses (pp. 423-439).
Springfield, IL: Charles C. Thomas.
Näring, G. W., Van Lankveld, W., & Geenen, R. (2007). Somatoform
dissociation and traumatic experiences in patients with rheumatoid
arthritis and fibromyalgia. Clinical and Experimental Rheumatology,
25, 872-877.
Nemeroff, C. B., Bremner, J. D., Foa, E. B., Mayberg, H. S., North, C.
S., & Stein, M. B. (2006). Posttraumatic stress disorder: A state-of-
the-science review. Journal of Psychiatric Research, 4 0, 1-21.
doi:10.1016/j.jpsychires.2005.07.005
Otis, J. D., Keane, T. M., & Kerns, R. D. (2003). An examination of the
relationship between chronic pain and post-traumatic stress disorder.
Jorunal of Rehabili tation Research and Development, 40, 397-406.
doi:10.1682/JRRD.2003.09.0397
Peterlin, B. L., Tietjen, G., Meng, S., Lidicker, J., & Bigal, M. (2008).
Post-traumatic stress disorder in episodic and chronic migraine. Pain
in the Head, 48, 517-522. doi:10.1111/j.1526-4610.2008.00917.x
Roth, R. S., Geisser, M. E., Bates, R. J. (2008). The relation of
post-traumatic stress symptoms to depression and pain in patients
with accident-related chronic pain. Pain, 9, 588-596.
doi:10.1016/j.jpain.2008.01.333
Salomons, T. V., Osterman, J. E., Gagliese, L., & Katz, J. (2001). Pain
flashbacks in posttraumatic stress disorder. Clinical Journal of Pain,
8, 231-234.
Schmahl, C., Meinzer, M., Zeuch, A., Fichter, M., Cebulla, M., Klein-
dienst, N., Ludascher P., Steil, R., & Bohus, M. (2008). Pain sensi-
tivity is reduced in borderline personality disorder, but not in post-
traumatic stress disorder and bulimia nervosa. World Journal of Bio-
logical Psychiatry, 29, 1-8. doi:10.1080/15622970701849952
Shalev, A. Y., Orr, S. P, & Peri, T. (1992). Physiological responses to
loud tones of Israeli post-traumatic stress disorder patients. Archives
of General Psychiatry, 49, 870-875.
Sharp, T. J., & Harvey, A. G. (2001). Chronic pain and posttraumatic
stress disorder: Mutual maintenance? Clinical Psychology Review,
21, 857-877. doi:10.1016/S0272-7358(00)00071-4
Shin, L. M., Wright, C. I., Cannistraro, P. A., Wedig, M. M., McMullin,
K., Martis, B., Macklin, M. L., Lasko, N. B., Cavanagh, S. R.,
Krangel, T. S., Orr, S. P., Pitman, R. K., Whalen, P. J., & Rauch, S.
L. (2005). A functional magnetic resonance imaging study of amyg-
dala and medial prefrontal cortex responses to overtly presented
fearful faces in posttraumatic stress disorder. Archives of General
Psychiatry, 62, 273-281. doi:10.1001/archpsyc.62.3.273
Stein, M. B., McQuaid, J. R., & Pedrelli, P. (2000). Post-traumatic
stress disorder in the primary care medical setting. General Hospital
Psychiatry, 22, 261-269. doi:10.1016/S0163-8343(00)00080-3
Symreng, I., & Fishman, S. M. (2004). Anxiety and pain. Pain Clinical
Updates, 12, 12-13.
Taylor, S., Fedoroff, I., Koch, W. J., Thordarson, D. S., Fecteau, G., &
Nicki, R. M. (2001). Posttraumatic stress disorder arising after road
traffic collisions: Patterns of response to cognitive-behavior therapy.
Journal of Consulting and Clinical Psychology, 69, 541-551.
doi:10.1037/0022-006X.69.3.541
Wallace, J., & Panch, G. (2001). Pain clinic, a new role for psychiatrists.
Psychiatric Bulletin, 25, 473-474. doi:10.1192/pb.25.12.473
Yehuda, R., Schmeidler, J., Wainberg, M., Binder-Brynes, K., & Du-
vdevani, T. (1998). Vulnerability to posttraumatic stress disorder in
adult offspring of Holocaust survivors. American Journal of Psy-
chiatry, 155, 1163-1171.