Journal of Cancer Therapy
Vol.2 No.2(2011), Article ID:5474,8 pages DOI:10.4236/jct.2011.22016
DNA-Repair ERCC1 Gene Polymorphisms in Epithelial Ovarian Cancer and Relation to Platinum Resistance and Survival
![]()
1Department of Oncology, Vejle Hospital, Vejle, Denmark;
2Institute of Regional Health Services Research, University of Southern Denmark, Odense C, Denmark;
3Pathology, Vejle Hospital, Vejle, Denmark.
Email: Karina.Dahl.Steffensen@slb.regionsyddanmark.dk
Received March 3rd, 2011; revised April 20th, 2011; accepted April 30th, 2011.
Keywords: Drug Resistance, Ovarian Cancer, Polymorphisms, ERCC1, DNA Repair, Predictive Marker
ABSTRACT
Objectives: Excision repair cross-complementation group 1 (ERCC1) is a key DNA repair gene in the nucleotide excision repair pathway which is activated in the repair of intraand interstrand DNA crosslink caused by platinum-based treatment. Two single nucleotide polymorphisms (SNPs) of the ERCC1 gene, codon 118 C/T and C8092A, have been reported to be functional, but the influence on platinum resistance and survival is not yet clear. The primary aim of the present study was to investigate whether the two SNPs were associated with resistance to standard combination carboplatin and paclitaxel chemotherapy and the potential prognostic impact in newly diagnosed ovarian cancer patients. Methods: Serum samples from 202 patients with newly diagnosed ovarian cancer were assessed for ERCC1 SNP genotyping using real time PCR. All patients were treated with first line carboplatin/paclitaxel chemotherapy. Results: There were no correlation between the ERCC1 118 C/T and C8092A genotypes and platinum resistance (P = 0.79 and P = 0.36, respectively). Furthermore, the results showed no association to progression free survival (P = 0.18 and P = 0.16, respectively) or overall survival (P = 0.89 and P = 0.78, respectively) for the two SNPs. Conclusions: The ERCC1 118 C/T and C8092A polymorphisms did not have significant influence on clinical outcome defined as platinum resistance, PFS and OS.
1. Introduction
Differences in chemotherapy response and patient survival may be related to inter individual genetic polymorphisms in patient’s genes since they can change the expression or the function of enzymes related to the metabolism of the chemotherapeutic drug offered to the patient.
Ovarian cancer is considered a chemo sensitive tumor as 70% - 85% of patients with advanced ovarian cancer respond to standard combination taxane/platinum-based treatment following primary surgical debulking [1]. Despite this apparent efficacy of treatment, the majority of these patients will relapse within a few years and if not already present, ultimately chemotherapy resistance will occur. Especially, the development of tumor resistance to platinum compounds is a major clinical problem in the treatment of ovarian cancer. Although the molecular mechanisms of platinum resistance are complex and multifactorial, DNA repair is essential to clinical drug resistance [2-4].
Excision repair cross-complementation group 1 (ERCC1) is a key DNA repair gene in the nucleotide excision repair pathway (NER) [5-7]. This important pathway is activated in the repair of intraand inter-strand DNA crosslink caused by platinum-based treatment. Excision of the formed DNA adducts is carried out by nucleotide excision repair proteins [8] that recognize the DNA damage and excise the cytotoxic platinum-DNA adducts from the injured DNA strand.
ERCC1 gene and protein expression have been found to be inversely correlated with response to platinumbased chemotherapy in ovarian cancer patients [9-11].
Furthermore, preclinical studies have also suggested that the expression levels of ERCC1 mRNA are related to platinum resistance. In ovarian cancer cell lines a 3-fold higher expression of ERCC1 mRNA was correlated with cisplatin resistance [12].
Single nucleotide polymorphisms (SNPs) in the ERCC1 gene may affect the function of the encoding gene. The ERCC1 gene, on chromosome 19q13.2 - q13.3, encodes a protein of 297 amino acids. Two common polymorphisms of the ERCC1 gene, 118 C/T (rs11615) and C8092A (rs3212986), have been reported [13-15]. The single nucleotide polymorphism (SNP) at codon 118 (position 19007/also synonymous with T19007C) causes a C > T change that codes for the same amino acid, asparagine, and it has been proposed to impair ERCC1 translation and reduce ERCC1 protein expression in cells, and thereby, effect the response to platinum based chemotherapy [15-17]. The C8092A polymorphism, located in position 8092 of the 3’-untranslated region of the gene consisting of a C > A change, may be involved in translational repression of ERCC1 mRNA [18] or affect ERCC1 mRNA stability resulting in impaired DNA repair capacity and has also been associated with the risk of adultonset glioma [19].
The primary aim of the present study was to investigate whether the two gene polymorphisms, ERCC1 118 C/T and C8092A were associated with resistance to standard combination carboplatin and paclitaxel chemotherapy and furthermore, to evaluate the potential prognostic impact in newly diagnosed ovarian cancer patients.
2. Materials and Methods
2.1. Ethics Statement
Patients received both oral and written information at the respective departments of clinical oncology before they signed an informed consent prior to collection of biological material. The study was conducted according to the principles expressed in the Declaration of Helsinki. The Danish Biomedical Research Ethics Committee and the Danish Data Protection Agency approved the study.
2.2. Study Population
Two hundred and two newly diagnosed ovarian cancer patients, stage I-IV, were included from four different Danish hospitals. The patients had histological confirmed epithelial ovarian cancer and all tumor specimens underwent central pathology revision.
The majority of the patients underwent primary debulking surgery while minor parts (N = 38, 18.8 %) were treated with neoadjuvant chemotherapy. They all received first line combination chemotherapy with carboplatin (AUC5) and paclitaxel (175 mg/m²). Treatment was administered every 3 weeks for at least four cycles.
Platinum sensitivity was defined as time to recurrence > 6 months after completion of first line platinum-based chemotherapy and platinum-resistance as recurrence ≤ 6 months after completion of first line platinum-based chemotherapy or progression during the first line platinum-based chemotherapy.
Recurrence of disease was evaluated as according to the Gynecologic Cancer Inter Group (GCIG) CA125 criteria’s [20,21] defined as an elevation of CA125 of at least twice the nadir value (and above upper normal level) or to twice the upper normal level (in patients that achieved normalization of CA125 during first line treatment) and radiological confirmation of tumor.
As a part of this translational research protocol the patients provided peripheral blood samples for translational research at baseline and at each chemotherapy treatment cycle (day 1).
2.3. ERCC1 Genotyping
DNA was extracted and purified from white blood cells recovered from the whole blood samples using the Maxwell® 16 Blood DNA Purification Kit (Cat. # AS1010, Maxwell Promega, Madison, WI 53711, USA).
The ERCC1 codon 118 C/T and C8092A polymorphisms were detected by polymerase chain reactions (PCR) using the 7900HT real-time PCR system (Applied Biosystems, CA 94404, USA. www.appliedbiosystems.com).
PCR reactions were set up in 10 μl reaction volume including 2 μl DNA and 8 μl TaqMan® Universal PCR Master Mix. TaqMan® validated SNP genotyping assay c__2532959_1_ for the ERCC1 codon 118 polymorphism (rs11615) and assay c__2532948_10 for the C8092A (rs3212986) polymorphisms were used.
After PCR amplification an endpoint plate read was performed and the final products were analyzed by the SDS (Sequence Detection Systems) software.
For quality controls known genomic DNA controls were included together with NTC (No Template Control).
2.4. Statistical Analysis
All clinical data and follow data were prospectively collected as part of a translational study protocol and the data were entered into case report forms. The correlation between ERCC1 polymorphisms and clinicopathological parameters was assessed by chi-square statistics and the same applied to the association between ERCC1 polymorphisms and response/resistance to chemotherapy.
The haplotypes were estimated using the Bayesian algorithm in the PHASE program version 2.1.1 [22,23], which is available at http://stephenslab.uchicago.edu/soft ware.html.
Progression free survival (PFS) was defined as the time from date of diagnosis (date of primary surgery/ biopsy) until disease recurrence or death, whichever came first. Overall survival (OS) was defined as the time from date of diagnosis until death regardless of cause. Univariate overall survival analysis was performed using the Kaplan-Meier method and log-rank statistics for comparison of survival curves. Multivariate progression-free and overall survival analysis was performed by the Cox regression model. The parameters entered in the Cox analysis were FIGO stage, grade, residual disease status, histology, age groups and the two SNPs as categorical variables. For the multivariate analysis, histology was divided into serous and non-serous, FIGO stages were divided into stage I/II vs. III/IV and grade into grade 1 vs. grade 2/3/not graded due to too many parameters (according to the number of events) in multivariate analyses if not merged into fewer groups.
Statistical significance was defined as a probability level, p < 0.05.
Statistical analyses were performed with the Number Cruncher Statistical System (NCSS) software (version 2007, Kaysville, Utah, www.ncss.com).
3. Results
3.1. Patients and Allele Frequencies
Genotyping for the two ERCC1 polymorphisms were obtained for all 202 patients.
The frequencies of the different gene polymorphism are shown in Table 1 along with the patient’s characteristics. Concerning ERCC1 C8092A only ten patients (5%) harbored the more uncommon AA polymorphic homozygotic genotype. According to the NCBI database, the C8092A genotype is found in approximately 5% in the European population. This is in consistence with our findings.
The observed number of each genotype was compared with that expected for a population in Hardy-Weinberg equilibrium and the investigated population showed no differences from this distribution (p = 0.99 for ERCC1 118 C/T and p = 0.90 for ERCC1 C8092A, χ²).
Linkage disequilibrium between the two polymorphic loci was observed (D = –0.148 and r2 = 0.54). The patient cohort was mainly composed of advanced stage patients with high grade serous tumors which are the most common presentation of epithelial ovarian cancer at diagnosis.
Six cycles of chemotherapy treatment were administered to 85% of the patients and 98% received at least three cycles. Thirteen patients received more than six cycles due to an expectation of a further tumor response with prolonged treatment up to a maximum of nine cycles.
One patient received only one cycle. This patient died two days after the first cycle of carboplatin and paclitaxel. The subsequent autopsy revealed that the patient died due to a lobar pneumonia and acute hemorrhagic gastritis.
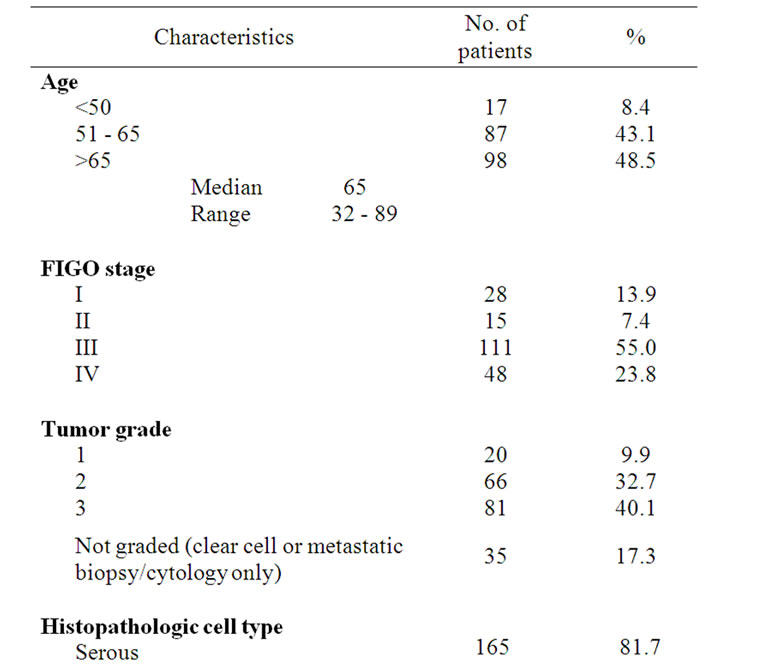
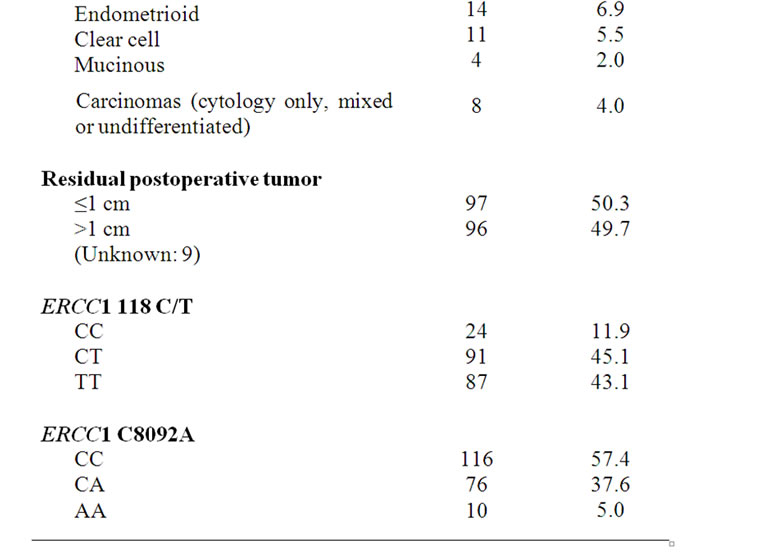
Table 1. Patient characteristics.
There were no correlation between SNPs and any of the classical clinicopathological variables (data not shown).
3.2. Association between ERCC1 SNPs and Platinum Resistance
The clinical response to the combination platinumpaclitaxel chemotherapy was assessed for all patients by the end of every third cycle. CA125 was measured at each cycle. The majority of the patients (157/202, (78%)) had measurable disease at baseline, prior to the first cycle of combination chemotherapy by modified GCIG CA125 criteria’s [20,21] and/or by Response Evaluation Criteria In Solid Tumors (RECIST) criteria’s.
After completion of the first line chemotherapy 59% of the patients with measurable disease had complete response and 32% had partial response. Only 13 patients (8%) did not respond to the first line treatment.
It appears from Table 2(a) that there were no correlation between the SNP genotypes and response to chemother apy. However, it should be noticed that only a very limited number of patients (N = 13) progressed or had stable disease during first line treatment making any statistical correlation between response rates and ERCC1 SNPs dubious.
At the time of analysis, recurrence data at 6 months follow up were available for 155 patients and 56 patients has progressed within 6 months of completion of chemotherapy.
As shown in Table 2(b) the SNP genotypes did not significantly correlate with platinum resistance defined as recurrence within 6 months of completed therapy.
3.3. Association between ERCC1 SNPs and Survival
Progression free and overall survival curves were estimated by the Kaplan-Meier method and the KaplanMeier survival curves are shown in Figure 1.
The Kaplan-Meier survival plots showed no statistically significant relationship between SNP genotypes and progression-free or overall survival.
For ERCC 118 C/T the Kaplan Meier estimate of median PFS for patients with ERCC1 118 C/C, C/T and T/T were 11.3, 19.3 and 13.9 months, respectively while the median PFS of patients with ERCC1 C8092A C/C, C/A and A/A were 14.1, 19.6 and 9.5 months respectively.
Patients with the ERCC1 118 CC and the ERCC1 8092 AA genotype graphically appeared to have a poor progression free survival, but these group were rather small (N = 24 and N = 10) and there were no statistically significant differences.
The Kaplan Meier estimate of median OS for patients with ERCC1 118 C/T, were 37.5 months for C/C, 39.6 months for C/T and 42.9 months for the T/T genotype, (p = 0.89). The median OS of patients with ERCC1 C8092A C/C, C/A and A/A were 42.9, 40.7 and 35.7 months, respectively (p = 0.78).
Furthermore, multivariate analysis showed no independent influence of the two SNPs on PFS or OS (Table 3).
3.4. Haplotype Analysis
Haplotype analysis was conducted to evaluate the combined effect of the two polymorphisms of the ERCC1 gene, 118 C/T and C8092A on platinum resistance, PFS and OS. The four possible haplotypes in this cohort of ovarian cancer patients were CC (11.4%), CA (22.9%), TC (64.8%), and TA (0.9%).
No significant associations were found between haplotypes and platinum-resistance, e.g. 35% patients carrying the TC haplotype were platinum-resistant compared to 47 % among patients not carrying the TC haplotype, p = 0.42, Fisher’s exact test (data not shown).
For patients carrying at least one allele with the TC haplotype (87.6% of the patients) an increased progression-free survival (p = 0.04) was found compared with patients not harboring the TC haplotype (data not shown). This increased PFS did not translate into a better overall survival for patients with the TC haplotype (p = 0.9, data not shown).
Multivariate analysis did not showed improved PFS (HR 0.57 [0.31-1.03, 95% CI], p = 0.06) or OS (HR 0.75 [0.37 - 1.51, 95% CI], p = 0.42) for the TC haplotype (data not shown).

Table 2 (a). Correlation between and ERCC1 SNPs and response (N = 157 patients with measurable disease).

Table 2 (b). Correlation between and ERCC1 SNPs and platinum resistance (N = 155 with follow up > 6 months).
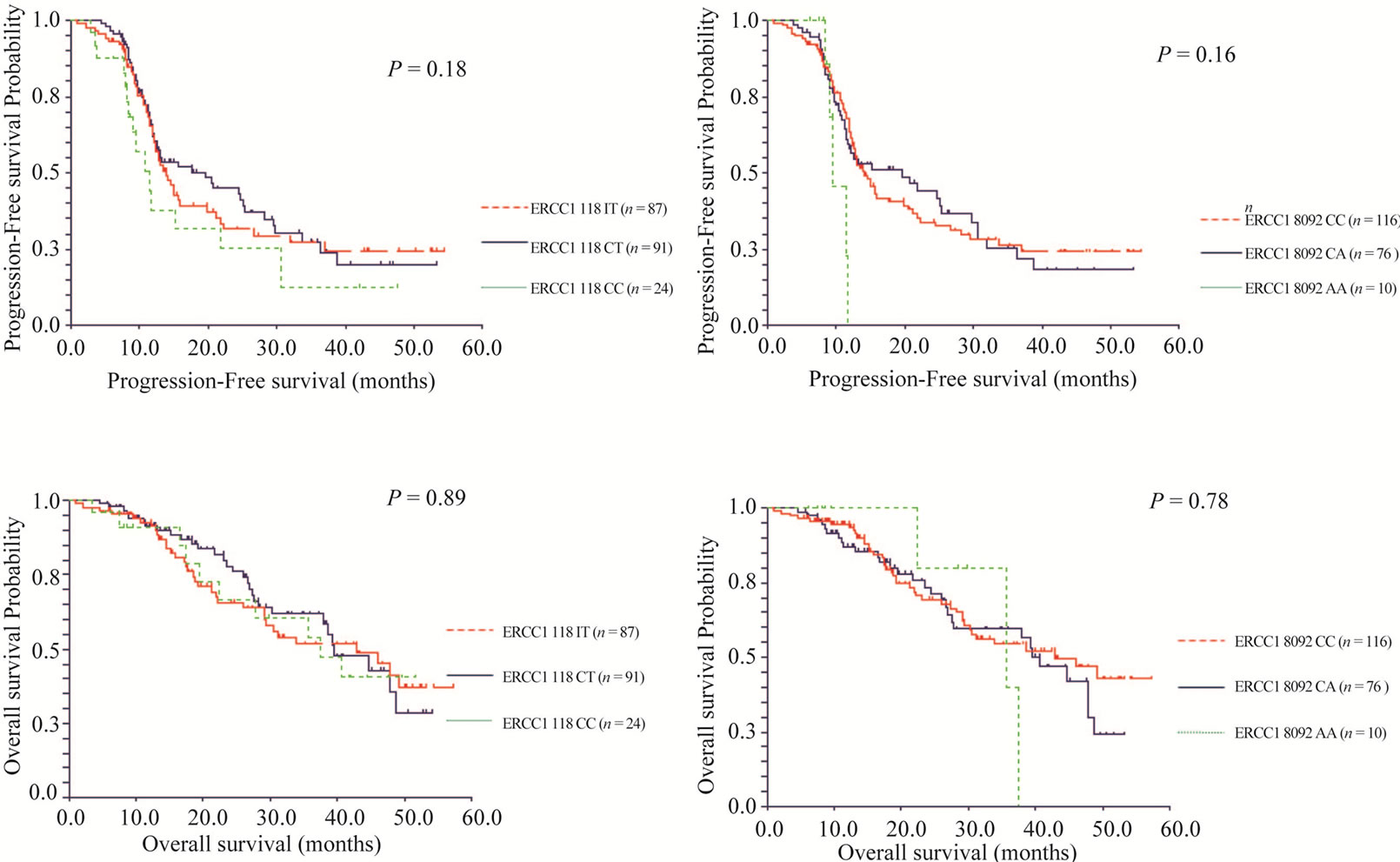
Figure 1. Kaplan-Meier estimates of PFS and OS for patients with the ERCC1 118 C/T and ERCC1 C8092A genotypes.


Table 3. Multivariate analysis (COX).
4. Discussion
Inter individual variation in chemotherapy response is a major factor in ovarian cancer.
Identifying parameters with influence on this variability may allow individualized and more effective treatments offered to patients. Single nucleotide polymorphisms may contribute to inter individual variability in DNA repair capacity and therefore predict outcome for platinum based chemotherapy. Polymorphisms in the ERCC1 gene have been implicated in response to platinum-based chemotherapy in several tumor types [13,24, 25], but data on ovarian cancer are still limited and contradictory.
The role of the two ERCC1 polymorphisms in the survival of ovarian cancer patients have been evaluated in a few other ovarian cancer studies with conflicting results. ERCC1 118 C/T polymorphism was investigated in a study by Smith et al. [26] who showed that the C/C genotype was associated with an impaired PFS (HR = 1.95, p = 0.051) and OS (HR = 2.01, p = 0.033). However, this was only shown in the subgroup of patients treated with platinum without paclitaxel, but not in the group treated with combination paclitaxel/platinum suggesting that the influence of the ERCC1 118 C/C genotype was minimized by the addition of a taxane which targets microtubules rather than DNA.
In the presented study the ERCC1 118 C/T polymorphism did not seem to be associated with clinical outcome, since we were not able to detect a significant correlation to platinum resistance or to PFS/OS. In agreement with the current study, three other studies in ovarian cancer were similarly not able to detect any influence of the ERCC1 118 C/T polymorphism on PFS or OS [27-29].
Another study by Kang et al. [30] demonstrated that platinum resistance was less frequently observed in patients with the C/T and T/T genotype (p = 0.018) and the same findings has been presented in a previous work by our group [10] investigating ERCC 118 C/T polymorphism in another ovarian cancer cohort showing that the T/T genotype had significantly better CA125 response (P = 0.045) in first line treatment although neither of these two studies showed any correlation to OS. The same applied to the present study in which no correlation with SNPs and OS was found. Interestingly, the former study by our group was performed on ovarian cancer patients treated with carboplatin and cyclophosphamide and supports to some extend the work by Smith et al. [26] described previously in which the ERCC1 118 polymorphism only seemed to have clinical impact in patients not treated with a taxane.
With respect to the C8092A polymorphism, we did not find any influence of C8092A polymorphism to clinical outcome. In agreement with the results presented, a very large trial [27] including 914 ovarian cancer patients did not either show any correlation of C8092A polymorphism to PFS or OS.
Nevertheless, this is in contrast with two other studies on ovarian cancer that both showed significantly longer PFS and OS in patients with the C/C genotype. One study [29] with 233 patients showed 68.6 months median survival in patients with the C/C genotype compared to 51.6 months for patients with the C/A + A/A genotypes (p = 0.047, p = 0.018 in multivariate analysis). The second study [28] did not show any correlation with response but reported a HR of 1.94 (p = 0.03) for the C/A + A/A for worse OS compared to the C/C genotype. The conflicting results also apply to other tumor types. Two studies in non-small cell lung cancer patients also reported worse survival for the A/C + A/A genotypes [24, 25]. A third non-small cell lung cancer study [31] has in discrepancy with these results shown significantly association of the 8092 A allele with longer OS in univariate and multivariate analysis.
Noteworthy, our study supports several other studies [24,29,31] suggesting that the ERCC1 118 C/T and C8092A SNPs may be in linkage disequilibrium.
The selection of one single locus as having sufficient phenotypic effect to impact on clinical outcome may be an oversimplification. There are many different pathways involved in DNA repair and even within the NER pathway several proteins are involved in the repair process although the ERCC1 protein is one of the key enzymes in this pathway.
The SNPs may not have any impact of the protein level. In the present study (data not presented, the ERCC1 protein data has been previously presented elsewhere [11]), as well as in another recently published study in non-small cell lung cancer [25], no correlation between ERCC1 SNP genotypes and ERCC1 protein expression were found. Beside changes in the encoding protein sequence, multiple other mechanisms such as gene regulation (e.g. polymorphisms in the promoter region or promoter methylation), mRNA processing (e.g. splicing, mRNA modification and turnover) and translation (e.g. microRNA induced inhibition of translation) can cause phenotypic changes.
5. Conclusions
The ERCC1 118 C/T and C8092A polymorphisms were not found to have significant influence on clinical outcome defined as platinum resistance, PFS and OS and were therefore not effective tools in selecting patients most likely to benefit to platinum-based chemotherapy.
6. Acknowledgements
We thank laboratory technologist’s Lone Frischknecht and Tina Brandt Christensen for their skilled work with the PCR analysis for ERCC1 SNP genotyping.
We also thank our collaborators at Aalborg University Hospital (Anni Grove, Bente Lund, Kirsten Lambæk, Janni Møldrup and Henrik Krarup), Herning Hospital (Nina Keldsen and Grethe Christensen) and Odense University Hospital (Mansoor Raza Mirza, Susanne Larsen and Troels Bergmann) for their kind contribution with patient material.
REFERENCES
- J. T. Thigpen, “Chemotherapy for Advanced Ovarian Cancer: Overview of Randomized Trials,” Seminars in Oncology, Vol. 27, No. 3, June 2000, pp. 11-16.
- C. A. Rabik and M. E. Dolan, “Molecular Mechanisms of Resistance and Toxicity Associated with Platinating Agents,” Cancer Treatment Reviews, Vol. 33, No. 4, February 2007, pp. 9-23. doi:10.1016/j.ctrv.2006.09.006
- R. P. Perez, “Cellular and Molecular Determinants of Cisplatin Resistance,” European Journal of Cancer, Vol. 34, No. 10, September 1998, pp. 1535-1542. doi:10.1016/S0959-8049(98)00227-5
- I. Díaz-Padilla and A. Poveda, “DNA Repair-Based Mechanisms of Platinum Resistance in Epithelial Ovarian Cancer: From Bench to Bedside,” Clinical Ovarian Cancer, Vol. 3, No. 1, May 2010, pp. 29-35. doi:10.3816/COC.2010.n.005
- M. Dabholkar, L. Bradshaw, R. J. Parker, I. Gill, F. Bostick-Bruton, F. M. Muggia, et al., “Cisplatin-DNA Damage and Repair in Peripheral Blood Leukocytes in Vivo and in Vitro,” Environmental Health Perspectives, Vol. 98, November 1992, pp. 53-59. doi:10.1289/ehp.929853
- E. Reed, “Platinum-DNA Adduct, Nucleotide Excision Repair and Platinum Based Anti-Cancer Chemotherapy,” Cancer Treatment Reviews, Vol. 24, No. 5, October 1998, pp. 331-344. doi:10.1016/S0305-7372(98)90056-1
- S. De, I, P. J. McHugh, P. H. Clingen and J. A. Hartley, “Defining the Roles of Nucleotide Excision Repair and Recombination in the Repair of DNA Interstrand Cross-Links in Mammalian Cells,” Molecular and Cellular Biology, Vol. 20, No. 21, November 2000, pp. 7980- 7990.
- Q. Li, J. J. Yu, C. Mu, M. K. Yunmbam, D. Slavsky, C. L. Cross, et al., “Association between the Level of ERCC-1 Expression and the Repair of Cisplatin-Induced DNA Damage in Human Ovarian Cancer Cells,” Anticancer Research, Vol. 20, No. 2A, March 2000, pp. 645-652.
- M. Dabholkar, F. Bostick-Bruton, C. Weber, V. A. Bohr, C. Egwuagu and E. Reed, “ERCC1 and ERCC2 Expression in Malignant Tissues from Ovarian Cancer Patients,” Journal of the National Cancer Institute, Vol. 84, No. 19, October 1992, pp. 1512-1517. doi:10.1093/jnci/84.19.1512
- K. D. Steffensen, M. Waldstrom, U. Jeppesen, I. Brandslund and A. Jakobsen, “Prediction of Response to Chemotherapy by ERCC1 Immunohistochemistry and ERCC1 Polymorphism in Ovarian Cancer,” International Journal of Gynecological Cancer, Vol. 18, No. 4, October 2007, pp. 702- 710.
- K. D. Steffensen, M. Waldstrom and A. Jakobsen, “The Relationship of Platinum Resistance and ERCC1 Protein Expression in Epithelial Ovarian Cancer,” International Journal of Gynecological Cancer, Vol. 19, No. 5, July 2009, pp. 820-825. doi:10.1111/IGC.0b013e3181a12e09
- K. V. Ferry, T. C. Hamilton and S. W. Johnson, “Increased Nucleotide Excision Repair in Cisplatin-Resistant Ovarian Cancer Cells: Role of ERCC1-XPF,” Biochemical Pharmacology, Vol. 60, No. 9, November 2000, pp. 1305-1313. doi:10.1016/S0006-2952(00)00441-X
- D. J. Park, W. Zhang, J. Stoehlmacher, D. Tsao-Wei, S. Groshen, J. Gil, et al., “ERCC1 Gene Polymorphism as a Predictor for Clinical Outcome in Advanced Colorectal Cancer Patients Treated with Platinum-Based Chemotherapy,” Clinical Advances in Hematology and Oncology, Vol. 1, No. 3, March 2003, pp. 162-166.
- M. R. Shen, I. M. Jones and H. Mohrenweiser, “Nonconservative Amino Acid Substitution Variants Exist at Polymorphic Frequency in DNA Repair Genes in Healthy Humans,” Cancer Research, Vol. 58, No. 4, February 1998, pp. 604-608.
- J. J. Yu, C. Mu, K. B. Lee, A. Okamoto, E. L. Reed, F. Bostick-Bruton, et al., “A Nucleotide Polymorphism in ERCC1 in Human Ovarian Cancer Cell Lines and Tumor Tissues,” Mutation Research, Vol. 382, No. 1-2, September 1997, pp. 13-20.
- J. S. Ryu, Y. C. Hong, H. S. Han, J. E. Lee, S. Kim, Y. M. Park, et al., “Association between Polymorphisms of ERCC1 and XPD and Survival in Non-Small-Cell Lung Cancer Patients Treated with Cisplatin Combination Chemotherapy,” Lung Cancer, Vol. 44, No. 3, June 2004, pp. 311-316. doi:10.1016/j.lungcan.2003.11.019
- J. J. Yu, K. B. Lee, C. Mu, Q. Li, T. V. Abernathy, F. Bostick-Bruton, et al., “Comparison of Two Human Ovarian Carcinoma Cell Lines (A2780/CP70 and MCAS) that are Equally Resistant to Platinum, but Differ at Codon 118 of the ERCC1 Gene,” International Journal of Oncology, Vol. 16, No. 3, March 2000, pp. 555-560.
- C. J. McGurk, M. Cummings, B. Koberle, J. A. Hartley, R. T. Oliver and J. R. Masters, “Regulation of DNA Repair Gene Expression in Human Cancer Cell Lines,” Journal of Cellular Biochemistry, Vol. 97, No. 5, April 2006, pp. 1121-1136. doi:10.1002/jcb.20711
- P. Chen, J. Wiencke, K. Aldape, A. Kesler-Diaz, R. Miike, K. Kelsey, et al., “Association of an ERCC1 Polymorphism with Adult-Onset Glioma,” Cancer Epidemiology, Biomarkers & Prevention, Vol. 9, No. 8, August 2000, pp. 843-847.
- G. J. Rustin, “Use of CA-125 to Assess Response to New Agents in Ovarian Cancer Trials,” Journal of Clinical Oncology, Vol. 21, No. 10, May 2003, pp. 187-193. doi:10.1200/JCO.2003.01.223
- G. J. Rustin, M. Quinn, T. Thigpen, B. A. du, E. Pujade-Lauraine, A. Jakobsen, et al., “Re: New Guidelines to Evaluate the Response to Treatment in Solid Tumors (Ovarian Cancer),” Journal of the National Cancer Institute, Vol. 96, No. 6, March 2004, pp. 487-488. doi:10.1093/jnci/djh081
- M. Stephens, N. J. Smith and P. Donnelly, “A New Statistical Method for Haplotype Reconstruction from Population data,” The American Journal of Human Genetics, Vol. 68, No. 4, April 2001, pp. 978-989. doi:10.1086/319501
- M. Stephens and P. Scheet, “Accounting for Decay of Linkage Disequilibrium in Haplotype Inference and Missing-Data Imputation,” The American Journal of Human Genetics, Vol. 76, No. 3, March 2005, pp. 449-462. doi:10.1086/428594
- W. Zhou, S. Gurubhagavatula, G. Liu, S. Park, D. S. Neuberg, J. C. Wain, et al., “Excision Repair Cross-Complementation Group 1 Polymorphism Predicts Overall Survival in Advanced Non-Small Cell Lung Cancer Patients Treated with Platinum-Based Chemotherapy,” Clinical Cancer Research, Vol. 10, No. 15, August 2004, pp. 4939-4943. doi:10.1158/1078-0432.CCR-04-0247
- T. Takenaka, T. Yano, C. Kiyohara, N. Miura, H. Kouso, T. Ohba et al., “Effects of Excision Repair Cross-Complementation Group 1 (ERCC1) Single Nucleotide Polymorphisms on the Prognosis of Non-Small Cell Lung Cancer Patients,” Lung Cancer, Vol. 57, No. 1, April 2010, pp. 101-107.
- S. Smith, D. Su, Rigault de la Longrais IA, P. Schwartz, M. Puopolo, T. J. Rutherford, et al., “ERCC1 Genotype and Phenotype in Epithelial Ovarian Cancer Identify Patients Likely to Benefit from Paclitaxel Treatment in Addition to Platinum-Based Therapy,” Journal of Clinical Oncology, Vol. 25, No. 33, November 2007, pp. 5172- 5179. doi:10.1200/JCO.2007.11.8547
- S. Marsh, J. Paul, C. R. King, G. Gifford, H. L. McLeod and R. Brown, “Pharmacogenetic Assessment of Toxicity and Outcome after Platinum Plus Taxane Chemotherapy in Ovarian Cancer: The Scottish Randomised Trial in Ovarian Cancer,” Journal of Clinical Oncology, Vol. 25, No. 29, October 2007, pp. 4528-4535. doi:10.1200/JCO.2006.10.4752
- H. S. Kim, M. K. Kim, H. H. Chung, J. W. Kim, N. H. Park, Y. S. Song, et al., “Genetic Polymorphisms Affecting Clinical Outcomes in Epithelial Ovarian Cancer Patients Treated with Taxanes and Platinum Compounds: A Korean Population-Based Study,” Gynecologic Oncology, Vol. 113, No. 2, May 2009, pp. 264-269. doi:10.1016/j.ygyno.2009.01.002
- T. C. Krivak, K. M. Darcy, C. Tian, D. Armstrong, B. E. Baysal, H. Gallion, et al., “Relationship between ERCC1 Polymorphisms, Disease Progression, and Survival in the Gynecologic Oncology Group Phase III Trial of Intraperitoneal Versus Intravenous Cisplatin and Paclitaxel for Stage III Epithelial Ovarian Cancer,” Journal of Clinical Oncology, Vol. 26, No. 21, July 2008, pp. 3598-3606. doi:10.1200/JCO.2008.16.1323
- S. Kang, W. Ju, J. W. Kim, N. H. Park, Y. S. Song, S. C. Kim, et al., “Association between Excision Repair Cross-complementation Group 1 Polymorphism and Clinical Outcome of Platinum-Based Chemotherapy in Patients with Epithelial Ovarian Cancer,” Experimental and Molecular Medicine, Vol. 38, No. 3, June 2006, pp. 320-324.
- A. Kalikaki, M. Kanaki, H. Vassalou, J. Souglakos, A. Voutsina, V. Georgoulias, et al., “DNA Repair Gene Polymorphisms Predict Favorable Clinical Outcome in Advanced Non-Small-Cell Lung Cancer,” Clinical Lung Cancer, Vol. 10, No. 2, March 2009, pp. 118-123. doi:10.3816/CLC.2009.n.015