Open Journal of Rheumatology and Autoimmune Diseases
Vol.4 No.3(2014), Article ID:49241,6 pages
DOI:10.4236/ojra.2014.43026
Profile of Secondary Bone Cancer in Lomé (Togo)
Owonayo Oniankitan, Kodjo Kakpovi, Messanvi Kpoti, Prénam Houzou, Eyram Fianyo, Viwalé E. S. Koffi-Tessio, Komi C. Tagbor, Moustafa Mijiyawa
Rheumatology Department, University Teaching Hospital of Lomé, Lomé, Togo
Email: Owonayo@yahoo.com
Copyright © 2014 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 25 June 2014; revised 25 July 2014; accepted 25 August 2014
ABSTRACT
Objectives: To determine the epidemiological, clinical and paraclinical profile of bone metastases cancer. Patients and Methods: It was a retrospective study performed on a series of cases, admitted in Rheumatology department of the University Teaching Hospital of Lomé, Togo from October 1989 to December 2008. The diagnosis of bone metastasis was made because of the existence of inflammatory bone pain, or pathological fracture, or bone swelling and a bone condensing or mixed or osteolytic radiological image. The anatomopathological evidence was made after biopsy of the bone lesion or primary cancer. 2018 patients were hospitalized in rheumatology, and among them 77 had documented bone metastasis. Results: There were 53 men (68.8%) and 24 women (31.2%) with a sex ratio of 2.2. The mean age was 56.6 ± 12.6 years, ranging from 21 to 82 years. The primary cancer most frequently found was that of the prostate, representing 57.1% of bone metastasis and breast in 15.6%. The main manifestations of patients with bone metastases were inflammatory bone pain (76.6%) and alteration of general condition (75.3%). The spine was the main area of pain (64.9%). The metastasis was bone condensing in 48.1% of cases, osteolytic in 40.3% and mixed in 11.6%. The average survival was 22 months. Conclusion: The clinical and radiological presentation remains classic. Cancer of the prostate and breast are the main neoplasia responsible for bone metastasis in our series. The diagnosis of the primary tumor is often made at the stage of metastasis in black Africa.
Keywords:Bone Cancer, Metastasis, Prostate, Black Africa

1. Introduction
Malignant bone tumors are severe and frequent diseases in the West and in the Africa. They are dominated by multiple myeloma and bone metastases [1] -[3] . Secondary bone cancer is the most common bone tumor [1] -[3] , making of the bone the third site of metastasis of cancer after lung and liver. Its discovery constitutes the revealing mode of primary cancer in one case over five. Bone metastases of broncho-pulmonary cancers and breast cancers are more common in the West [1] -[4] . In Africa, prostate, breast and liver cancers are most often responsible for bone metastases [5] -[12] . In Africa in general, the diagnosis is not always easy and care remains poor due to lack of technological and financial resources and above all the still very limited access to appropriate health care facilities. Despite its frequency and severity, secondary bone cancer remains poorly documented in Togo as in other countries in Sub-Saharan Africa [3] [12] . The purpose of this study was to determine the epidemiological, clinical and paraclinical profile of bone metastases cancer in a rheumatologic service in Lomé.
2. Patients and Methods
This study was retrospectively performed on a series of cases admitted in the Department of Rheumatology, University Hospital Sylvanus Olympio, Lomé, Togo’s capital between January 1990 and December 2008. The series included all patients diagnosed with bone metastasis of any cancer. Most of these patients were diagnosed with the cancer after being admitted in the Rheumatology ward for inflammatory bone pain. The demographic, clinical, and paraclinical data of patients were collected from their records. The diagnosis of bone metastasis was based essentially on the clinical picture (inflammatory bone pain and alteration of the general condition) and radiological features (mainly bone condensing, osteolysis). A bone biopsy or a biopsy of the primary tumor as made to confirm the malignancy only when the diagnosis was uncertain. The cases where the primary tumor was not found were excused from this study. The anemia corresponded to a hemoglobin concentration lower than 10 g/dl. A plasma creatinine greater than 12 mg/l was considered renal insufficiency. Serum calcium greater than 110 mg/l was considered hypercalcemia. Erythrocyte sedimentation rate greater than 20 mm in the first hour was considered accelerated. The combination of fatigue, anorexia, weight loss and pallor or the presence of at least three of these symptoms was considered impaired general condition. A weight loss greater than 10% was considered massive and a weight loss below 10% was considered moderate. A serum PSA level inferior to 4 ng/ml was considered normal. No patient received bone scan or magnetic resonance imaging (MRI) due to the absence of scintigraphy and MRI in Togo at the time of the study. The statistical analysis of results was performed using SPSS version 17.
3. Results
Of the 2018 rheumatic patients admitted in 19 years, 77 (3.8%) had bone metastases. The mean age at admission of those 77 patients (53 men, 68.8% and 24 women, 31.2%) was 56.6 ± 12.6 years with extremes of 21 and 82 years and the age group most affected was between 46 and 65 years (35 cases, 45.4%). The mean disease duration was 17.3 ± 13.4 months. The mean duration of hospitalization was 39.10 ± 40.20 days and the median was 25 days. The primary cancer most frequently found was that of the prostate, representing 57.1% of bone metastasis and breast in 15.6% (Table 1).

Table 1. Demographics data of the 77 patients with metastases according to the primary tumor.
*m ± SD: Mean ± Standard Deviation; F/M: Female/Male.
Primary cancer was seen in 23 patients (29.9%) before metastasis and it was revealing in the remaining 54 (77.1%). The mean time between the diagnosis of primary cancer and the development of metastasis was 4.4 ±3.5 years in 29.9% of the cases. The onset of the disease was insidious in 65 patients (84.4%) and in 12 others sudden (15.6%). Inflammatory bone pain (59 cases, 76.6%), alteration of the general condition (58 cases; 75.3%) and spinal cord compression (34 cases; 44.1%) were the main manifestations in our patients (Table 2).
The alteration of the general condition was reflected mainly by a massive weight loss in 48 cases (62.3%) and a moderate weight loss in the remaining 29 patients (37.7%). The mean body mass index was 20.8 ± 3.5 kg/m2, with a range from 14.69 to 31.14 kg/m2. Only 14% of our patients had a BMI greater than 25 kg/m2. All patients suffered from bone pain and the spine was the main site of pain (50 cases, 64.9%) with a clear preference for the lumbar segment (48 cases, 62.3%). The other sites of spinal pain were thoracic segment (13 cases, 16.9%) and cervical segment (8 cases, 10.4%). Most other affected sites were the long bones (14 cases, 18.2%), the pelvis (9 cases, 11.7%) and the ribs (8 cases, 10.4%). An affection of more than one region was revealed in 16 cases (20.8%). In X-ray, it was essentially bone condensing (37 cases, 48.1%), bone lysis (31 cases, 40.3%) and vertebral compression (23 cases, 29.9%) (Table 3).
Of the 37 patients with bone condensing, 35 had a prostate cancer (94.6%) and 2 patients a breast cancer (5.4%). The locations were mostly the spine (46 cases, 59.72%) (Figure 1), followed by the pelvis (25 cases, 32.5%).
Anemia was found in 39 patients with a mean hemoglobin level of 7.8 g/dl. Erythrocyte sedimentation rate was elevated in 72 patients. Sedimentation rate mean was 83.3 ± 32.7 mm in the first hour with a range from 10 mm to 147 mm. The prostate specific antigen mean was 301.87 ± 738.23 ng/ml with a range from 35 ng/ml to
 (a)
(a)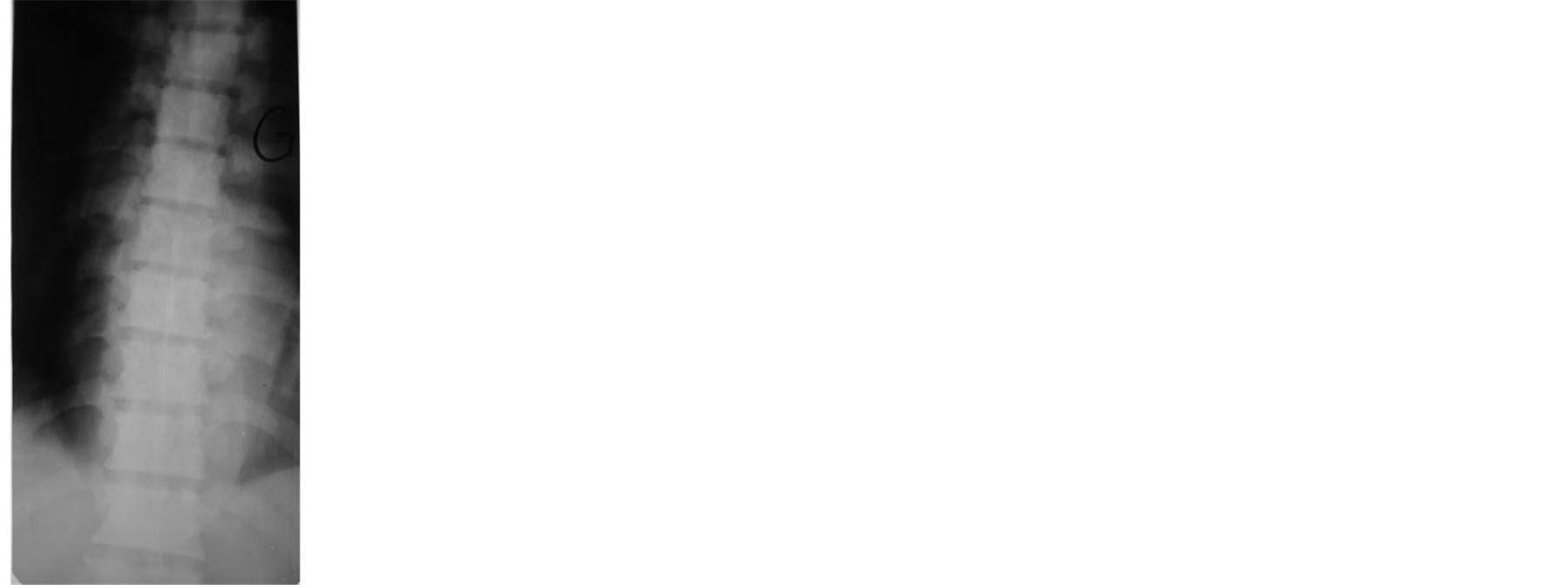 (b)
(b)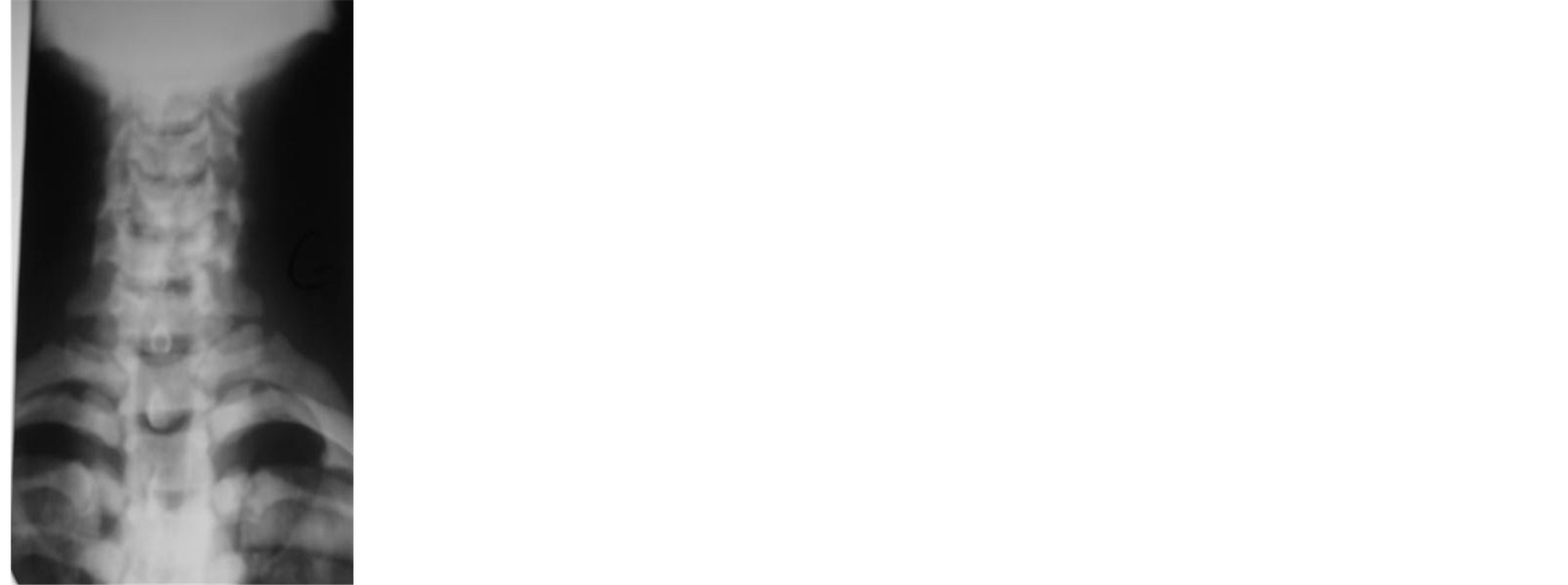 (c)
(c)
Figure 1. Spine bone condensing in 64 years patient with cancer of prostate: (a) = Lumbar spine; (b) = Thoracic spine; (c) = Cervical spine.
Table 2.Distribution of the 77 patients according to the circumstances of discovery of bone metastasis.
*Mixed bone pain = Pain with some features of inflammatory pain and mechanical pain.
Table 3. Distribution of the 77 patients according to the result of the X-ray of the painful bone segment.
5000 ng/ml and the median was 105 ng/ml. Creatinine was high in five patients with a range from 20 mg/l to 45 mg/l. Hypercalcemia was observed in 11 (14.3%) of the 77 patients with a range from 121 mg/l to 135 mg/l. A severe anemia caused the death of seven patients with prostate bone metastasis (9.1%) during hospitalization. The average survival was 22 months.
4. Discussion
In this study, 3.8% of patients suffering from bone metastases on 2018 patients admitted in 19 years. Male dominance remains classic as described by many authors [8] [10] -[12] . It seems to be explained by the frequency of prostate cancer, a cancer of easy diagnosis in our professional context. The same is true for the mean age of onset at 56 years, at least in Africa [11] -[13] . The appearance of metastasis seems later in western series as shown by Houze et al. [14] and Vandecandelaere et al. [15] who reported an mean age of 77 and 63 years respectively. The mean time before consultation for bone metastasis remains long, 17 months in our series and 22 months in the series of Ntsiba et al. from Congo [12] . Medical wandering of patients before specialist consultation is the main cause [9] [16] , as well as the lack of effective means of investigation for early diagnosis. This long period before consultation suggests a predominant mode of revelation of bone metastasis by bone complications, neurological or metabolic.
The mode of clinical revelation remains dominated by inflammatory bone pain, joining results from Ntsiba et al. in Congo [12] , Belaksir et al. in Morocco [11] and Kagohashi et al. in Japan [17] . It is present in 76.6% of patients in our series, of variable intensity ranging from simple discomfort to excruciating pain, debilitating, rebellious to the usual analgesics. hypercalcemia is most often asymptomatic and is not a current mode of revelation in our study as in the study of Ntsiba et al. [12] . This seems surprising given the pejorative nature of the existence of hypercalcemia during bone metastasis [11] [12] .
Prostate cancer (44 cases, 57.1%) is the first responsible for bone metastases cancer followed by breast cancer (12 cases, 15.6%). These results converge with those obtained by Ntsiba et al. in the Congo who noted on two different studies a frequency of 3.5% and 2.2% metastases associated with prostate cancers before those from cancers of the breast [8] [12] . Our results were consistent with those of the Côte d’Ivoire from two different studies. It was the study of Kouakou who found prostate cancer followed by the hepatic carcinoma, cancer of the kidney, thyroid, lungs, breasts and anus [18] . Daboiko et al. have found a clear dominance of bone metastases cancer of the prostate always in the Cocody CHU [19] . The results of our study were comparable to those obtained in Cameroon by Bahebeck et al. who found the cancer of the prostate gland, followed by cancer breast, the hepatic carcinoma and cancer of the thyroid gland [5] .
All these results suggest a higher incidence of prostate cancer in the black compared to the white race [15] . In Tunis, Belhaj et al. found on 60 cases of bone metastases, 25 cases of breast cancer and 8 cases of oto-rhino-laryngologic cancer [20] . In Lille, Vandecandelaere et al. indicated a predominance of broncho-pulmonary cancers compared to prostate and breast cancers [15] . Still, these data confirm the high incidence of prostate cancer within the black compared to white. At the end of our study on 77 collected cases, no cases of bone metastasis from thyroid cancer had been objectified, which was not very opposed to the results obtained by Hindié et al. who found in Paris on 961 patients with thyroid cancer and who received a total thyroidectomy, only 16 cases (1.6%) of bone metastasis [21] .
In X-rays, the presentation of bone metastasis remains classic, condensing, osteolytic or mixed. The predominance of bone condensing images is correlated with the frequency of bone metastasis of prostate cancer, first osteophilic responsible for such images [8] [22] [23] . However it does not appear to be the only responsible in our series and in the series of Ntsiba et al, since 5.4% and 6.2% respectively of condensing images were present in breast cancer.
5. Conclusion
The clinical and radiological presentation of bone metastasis remains classic. Pain is the main revealing symptom. Prostate cancer and breast cancer are mainly responsible for bone metastasis in our series. The diagnosis of the primary tumor is often made at the stage of metastasis in black Africa.
Conflict of Interest
No conflict of interest.
References
- Jemal, A., Tiwari, R.C., Murray, T., Samuels, A., Ward, E., Feuer, E.J. and Thun, M.J. (2004) Cancer Statistics 2004. CA: A Cancer Journal for Clinicians, 54, 8-29. http://dx.doi.org/10.3322/canjclin.54.1.8
- Virk, M.S. and Lieberman, J.R. (2007) Tumor Metastasis to Bone. Arthritis Research and Therapy, 9, 10.
- Li, K.K., Sinclair, E., Pope, J., et al. (2008) A Multidisciplinary Bone Metastases Clinic at Toronto Sunnybrook Regional Cancer Centre. A Review of the Experience from 1999 to 2005. Journal of Pain Research, 1, 43-48.
- Gremaud, M., Delouche, D., Monnerat, C., et al. (2006) Treatment of Bone Metastases with Bisphosphonates. Revue Médicale Suisse A, 2, 1861-1866.
- Bahebeck, J., Atangana, R., Eyenga, V., et al. (2003) Bones Tumors in Cameroon: Incidence, Demography and Histopathology. International orthopaedics, 27, 315-317. http://dx.doi.org/10.1007/s00264-003-0480-7
- Sarma, N.H., Al-fituri, O., Visweswara, R.N., et al. (1994) Primary Bone Tumor in Eastern Libya, a 10 Year Study. The Central African journal of medicine, 40, 148-151.
- Abdulkareem, F.B., Evesan, S.U., Akinde, O.R., et al. (2007) Pathological Studies of Bone Tumors at the National Orthopaedic Hospital, Lagos, Nigeria. Western African Journal of Medicine, 26, 306-311.
- Bileckot, R., Miakoundoba, R.C. and Nkoua-Mbon, J.B. (2008) Two Brazzaville Series of Bone Metastases. Carcinol Prat Afrique, 8, 57-60.
- Ly, M., Ly, A., Rodrigues, M., et al. (2010) Cancer in Africa, a New Health Challenge. Examples of Mali and Mali Onco Association. Bull Cancer, 97, 965.
- Gombe-Mbalawa, C. and Ibara, G. (2011) Report Functioning Cancer Registry of Brazzaville from January 1st to December 31st 2010. Cancer Registry of Brazzaville, 2011.
- Belaksir, L., Seknaji, N., Touimy, M., Janani, S., et al. (2010) Bone Metastases: Experience of Rheumatology CHU Ibn Rushd at Casa. Revue du Rhumatisme, 77, A131-A325.
- Ntsiba, H., N’soundhat, N.E.L., Ndounga, E. and Ondzal, A.E. (2013) Profile of Secondary Bone Cancer in Brazzaville. Open Journal of Rheumatology and Autoimmune Diseases, 3, 251-254. http://dx.doi.org/10.4236/ojra.2013.34039
- Seknaji, N., Touimy, M., Belksir, L., et al. (2010) Contribution of Bone Biopsy in Search of Primary Cancer of Bone Metastases. Revue Du Rhumatisme, 77, A131-A325.
- Houze, P., Ranaivosoar, R., Prost, A.C., et al. (1995) Bone Metastases of Prostate Cancer: Contribution of Specific Determination of Bone Alkaline Phosphatase. Immuno-Analyse & Biologie Specialisee, 10, 27-33.
- Vandecandelaere, M., Filipo, R.M., Cortet, B., Catanzariti, L., Duquesnoy, B. and Delcambre, B. (2004) Bone Metastases Revealing: A Comparative Study in 30-Years Intervals. Revue Du Rhumatisme, 71, 390-396. http://dx.doi.org/10.1016/S1169-8330(03)00304-1
- Gombe-Mbalawa, C., Diouf, D., Mbon, J.B.N., et al. (2013) Arrival of Cancer Patients in Advanced Stages: Attempted Identification of Responsibility. Bull Cancer, 100, 167-171.
- Vandecandelaere, M., Flipo, R.M., Cortet, B., Catanzariti, L., Duquesnoy, B., Delcambre, B. (2004) Bone Metastasis Revealing Primary Tumor. Comparison of Two Series Separated by 30 Years. Joint Bone Spine, 71, 224-229. http://dx.doi.org/10.1016/S1297-319X(03)00123-4
- Kouakoué, N. (1994) Bone Metastasis in Ivory Coast Hospital. Rhumatologie (Aix-les-Bains) A, 46, 243-245.
- Daboiko, J.C., Eti, E., Dollo, Y.I., Ouali, B., Ouattara, B. and Kouakou, N.M. (2004) Inflammatory Rheumatic Diseases at Cocody University Medical Center (Abidjan) from March 1998 to March 2000. Joint, Bone, Spine, 71, 598-599.
- Belhaj, R., Boussen, H., Ghanem, A., Essafer, S., Harzallah, L., Ayed, F.B., et al. (2002) Bioclinical Correlations in Bony Metastases. Results of a Prospective Study. 60 Cases. La Tunisie médicale, 80, 691-695.
- Hindié, E., Zanotti-Fregonara, P., Keller, I., Duron, F., Devaux, J.Y., Calzada-Nocaudie, M., et al. (2007) Bone Metastases of Differentiated Thyroid Cancer: Impact of Early 131I-Based Detection on Outcome. Endocrine Related Cancer, 14, 799-807. http://dx.doi.org/10.1677/ERC-07-0120
- Proust, C., Proust, J. and Maubon, A. (2006) Imaging Bone Metastases. Nuclear Medicine. Functional and Metabolic Imaging, 30, 149-154.
- Belaksir, L., Touimy, M., Janani, S., et al. (2010) Revealing Bone Metastasis of Prostate Cancer. Revue Du Rhumatisme, 77, A131-A325.