 Open Journal of Stomatology, 2011, 1, 75-83 doi:10.4236/ojst.2011.13013 Published Online September 2011 (http://www.SciRP.org/journal/OJST/ OJST ). Published Online September 2011 in SciRes. http://www.scirp.org/journal/OJST Cephalometric norms for a sample of Emirates adults Huda M. Abu-Tayyem1*, Amna H. Alshamsi2, Sayed Hafez1, Eman Mohie ElDin1 1Faculty of Oral and Dental Medicine, Cairo University, Cairo, Egypt; 2Ministry of Health, Sharjah, United Arab Emirates. Email: *huda_ma@hotmail.com Received 23 May 2011; revised 21 July 2011; accepted 3 August 2011. ABSTRACT Introduction: European-American norms are still used in the orthodontic treatment of Emirates pa- tients despite the different ethnic backgrounds of the Emirates. The purpose of this study was to formulate cephalometric norms for lateral cephalometric mea- surements of Emirates adults and to study gender differences. Methods: Lateral cephalometric radio- graphs of 176 Emirates adults, 91 males and 85 fe- males, were selected according to the following crite- ria; an age range between 19 to 25 years, esthetically pleasing and harmonious faces with balanced and acceptable profiles and occlusions, normal skeletal and dental relationship, all permanent teeth present, and no history of orthodontic treatment or facial trauma. The mean values and standard deviations of 91 angular and 21 linear cephalometric variables were calculated using the Dolphin version 10.5 soft- ware package. The resulting norms for Emirates male and female groups were compared using a stu- dent t-test. Results: Several statistically significant gender differences were noticeable. Skeletally, Emir- ates males showed significantly greater (p < 0.001) total, anterior, and posterior cranial base lengths as well as longer facial heights, greater SGn-FH (˚), ANS Xi PM (˚), and FH/MP (˚) angles than females. In addition, Emirates males had significantly greater (p < 0.001) Co-A (mm), Co-Gn (mm), and significantly greater (p < 0.05) Pog-N vert (mm) than females. Dentally, Emirates males had significantly greater (p < 0.05) UI-SN (˚) and U1-NA (˚), U1-NA (mm), and L1-NB (mm) (p < 0.001) than females. For soft tissue measurements there were significant gender differ- ences (p < 0.001) for all angular and linear measure- ments except for lower lip to E-plane and nose prominence measurements which have no significant gender difference. Emirates males revealed greater measurements than females except for soft tissue con- vexity, Z-angle, and both upper and lower lips pro- trusion which were significantly greater in Emir- ates females. Conclusions: The use of specific ce- phalometric standards for Emirates adults, sepa- rate for gender, seems to be justified. It is appro- priate to put these cephalometric norms into daily orthodontic practice when Emirates adults are be- ing treated. Keywords: Emirates Norms; Cephalometric; Norms 1. INTRODUCTION Since its introduction in 1931 by Broadbent [1] and Hofrath [2] in the United States and Germany, respec- tively, radiographic cephalometry has become one of the most important tools of clinical and orthodontic research [3]. Cephalometric norms provide useful guidelines to orthodontists in their diagnosis and evaluation of ortho- dontic treatment outcomes. Moreover their importance exists to investigate the average values, shapes and variations among any population [4]. Harmonious facial esthetics and optimal functional occlusion have long been recognized as the most impor- tant goals of orthodontic treatment. Orthodontic treat- ment is best when the facial and cephalometric charac- teristics of the ethnic background of patients are consid- ered [4,5]. The orthodontic literature contains many studies involving cephalometric and profile standards of Caucasian and European-American [5-15], African- American [16-24], Japanese [25-29], Chinese [30-33], Polish [34], Filipinos [35], Mexican-Americans [36], Korean [37,38], Turkish populations [39-42], Indians [43], Brazilians [44], and Puerto Rican Americans [45], but little published data for Arabs [46-58] and non for Emirates in specific. This information is considered as a critical base which should be used for studying growth, diagnosis, treatment planning and prognosis of such population. Hajighadimi et al. [46] studied craniofacial character- istics of 67 Iranian children (35 females with and 32  H. M. Abu-Tayyem et al. / Open Journal of Stomatology 1 (2011) 75-83 76 males) using Tweed and Steiner analyses. They reported that Iranians have a more convex soft tissue profile compared with Tweed’s and Steiner’s standards; whereas Iranian males had more procumbent dentitions than the female one. Bishara et al. [49] established cephalometric standards for Egyptian adolescent males and females and compared them with a matched Iowa adolescent sample. There was a great similarity in the overall facial mor- phology between the Egyptian and Iowan populations. Hamdan and Rock [51] evaluated the cephalometric features of a Jordanian population as compared with the Eastman standards and found different skeletal and den- tal cephalometric features for the Jordanians. Shalhoub et al. [52] evaluated lateral cephalometric radiographs of 48 adult Saudis with normal facial proportions, com- pared them with a North American sample, and estab- lished a set of cephalometric norms for Saudi adults liv- ing in Riyadh. Sarhan and Nashashibi [53] compared cephalometric radiographs of Saudi males (10 - 14 years old) with a similar British sample. They found slightly more prognathic Saudi faces, more protruded incisors and lower gonial and saddle angles as compared with the British sample. Al-Jasser [54] described the craniofacial characteris- tics of 87 Saudi students with acceptable profiles and occlusions and compared them with Steiner's Euro- pean-American standards. It was concluded that Saudis have different craniofacial features when compared with Steiner norms. Al-Jame et al. [55] studied lateral cepha- lograms of 162 Kuwaitis (82 males and 80 females of mean age 13.27 ± 0.42 years and 13.21 ± 0.43 years, respectively), with normal occlusion to establish lateral cephalometric hard tissue norms and to compare them with the published norms. They found that the average subject in the sample had a steeper mandibular plane, a more convex profile with a tendency for reduced chin protrusion, and a more protrusive dentition than the norms of the common analysis systems. Hassan [56] evaluated 70 lateral cephalometric radiographs of Saudis (32 females and 38 males; aged 18 - 28 years) with ac- ceptable profiles and occlusions living in the western region of Saudi Arabia and compared them with Euro- pean-American norms. He found that Saudis tended to have an increased ANB angle because of retrognathic mandibles and bimaxillary protrusion as compared with European-Americans. Hashim and AlBarakati [57] eva- luated cephalometric radiographs of 56 Saudi adults (30 males and 26 females) with pleasant and balanced facial profiles. The Saudi females had a greater angle of total facial convexity and soft tissue facial plane angle and a shorter lower lip than the males. Their results revealed significant differences in most of the soft tissue variables when comparing Saudis with Caucasian Americans as well as in other ethnic groups. Al-Gunaid et al. [58] studied 50 adult Yemeni men (with a mean age was 23.1 years) with normal occlusion and esthetically pleasing profile and compared them with cephalometric standards of normal North American white people according to Legan-Burstone and Holdaway analyses. They con- cluded that soft-tissue facial profiles of white Yemenis and Americans are different in certain respects and these racial differences must be considered during diagnosis and treatment planning. From this review, it can be concluded that there are differences in dentofacial relationships between various ethnic and racial groups. Therefore, it is important to develop standards for various populations. Accordingly, the present study was concerned with an ethnic group for which little cephalometric information was available, the Emirates adults. The purpose of this study was to for- mulate cephalometric norms for the Emirates adults with acceptable facial profile and occlusion and to study gender differences. 2. MATERIAL AND METHODS This study was carried out on a total sample of 176 Emirates adults (91 males and 85 females) selected from individuals who attended the Emirates health centers, high schools and colleges according to the following criteria: natural born ethnic Emirates with Emirates grandparents, ranged in age from 19 to 25 years old, balanced and acceptable facial profiles, normal skeletal Class I with well aligned upper and lower dental arches, permanent dentition stage (the third molars may or may not be present), no history of previous orthodontic or prosthodontic treatment , no history of maxillofacial or plastic surgery, no congenital facial anomalies, and no history of systemic diseases or chronic illness that may affect the normal dentofacial growth. Initially, a clinical examination was made to deter- mine the status of the occlusion, and those subjects who were judged to have a normal occlusion were selected. The procedure of selecting subjects started with filling personal information by the subject. Then three examin- ers, including two orthodontists and one postgraduate orthodontic student, examined overjet, overbite, crowd- ing, and spacing condition of the teeth. Two hundred subjects met these criteria in the preliminary examina- tion and were asked to report to the Department of Or- thodontics, Sharjah Dental Center, Ministry of Health, Sharjah, United Arab Emirates for a more detailed ex- amination. Of these 200 subjects, 24 chose not to par- ticipate in the study. A closer examination of the subjects indicated that 15 had different types of malocclusion, and another 9 were either older or younger than the age C opyright © 2011 SciRes. OJST 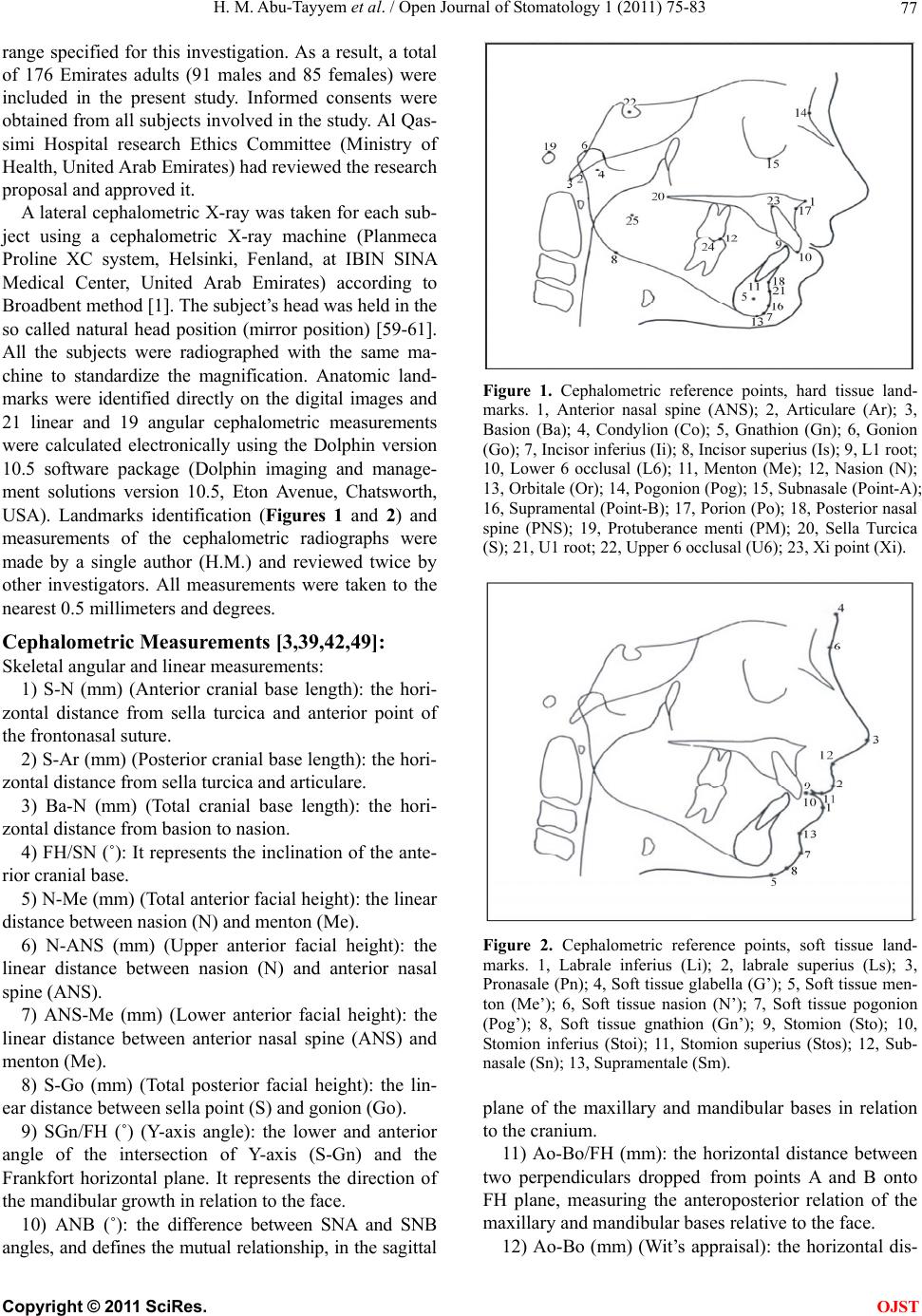 H. M. Abu-Tayyem et al. / Open Journal of Stomatology 1 (2011) 75-83 77 range specified for this investigation. As a result, a total of 176 Emirates adults (91 males and 85 females) were included in the present study. Informed consents were obtained from all subjects involved in the study. Al Qas- simi Hospital research Ethics Committee (Ministry of Health, United Arab Emirates) had reviewed the research proposal and approved it. A lateral cephalometric X-ray was taken for each sub- ject using a cephalometric X-ray machine (Planmeca Proline XC system, Helsinki, Fenland, at IBIN SINA Medical Center, United Arab Emirates) according to Broadbent method [1]. The subject’s head was held in the so called natural head position (mirror position) [59-61]. All the subjects were radiographed with the same ma- chine to standardize the magnification. Anatomic land- marks were identified directly on the digital images and 21 linear and 19 angular cephalometric measurements were calculated electronically using the Dolphin version 10.5 software package (Dolphin imaging and manage- ment solutions version 10.5, Eton Avenue, Chatsworth, USA). Landmarks identification (Figures 1 and 2) and measurements of the cephalometric radiographs were made by a single author (H.M.) and reviewed twice by other investigators. All measurements were taken to the nearest 0.5 millimeters and degrees. Cephalometric Measurements [3,39,42,49]: Skeletal angular and linear measurements: 1) S-N (mm) (Anterior cranial base length): the hori- zontal distance from sella turcica and anterior point of the frontonasal suture. 2) S-Ar (mm) (Posterior cranial base length): the hori- zontal distance from sella turcica and articulare. 3) Ba-N (mm) (Total cranial base length): the hori- zontal distance from basion to nasion. 4) FH/SN (˚): It represents the inclination of the ante- rior cranial base. 5) N-Me (mm) (Total anterior facial height): the linear distance between nasion (N) and menton (Me). 6) N-ANS (mm) (Upper anterior facial height): the linear distance between nasion (N) and anterior nasal spine (ANS). 7) ANS-Me (mm) (Lower anterior facial height): the linear distance between anterior nasal spine (ANS) and menton (Me). 8) S-Go (mm) (Total posterior facial height): the lin- ear distance between sella point (S) and gonion (Go). 9) SGn/FH (˚) (Y-axis angle): the lower and anterior angle of the intersection of Y-axis (S-Gn) and the Frankfort horizontal plane. It represents the direction of the mandibular growth in relation to the face. 10) ANB (˚): the difference between SNA and SNB angles, and defines the mutual relationship, in the sagittal Figure 1. Cephalometric reference points, hard tissue land- marks. 1, Anterior nasal spine (ANS); 2, Articulare (Ar); 3, Basion (Ba); 4, Condylion (Co); 5, Gnathion (Gn); 6, Gonion (Go); 7, Incisor inferius (Ii); 8, Incisor superius (Is); 9, L1 root; 10, Lower 6 occlusal (L6); 11, Menton (Me); 12, Nasion (N); 13, Orbitale (Or); 14, Pogonion (Pog); 15, Subnasale (Point-A); 16, Supramental (Point-B); 17, Porion (Po); 18, Posterior nasal spine (PNS); 19, Protuberance menti (PM); 20, Sella Turcica (S); 21, U1 root; 22, Upper 6 occlusal (U6); 23, Xi point (Xi). Figure 2. Cephalometric reference points, soft tissue land- marks. 1, Labrale inferius (Li); 2, labrale superius (Ls); 3, Pronasale (Pn); 4, Soft tissue glabella (G’); 5, Soft tissue men- ton (Me’); 6, Soft tissue nasion (N’); 7, Soft tissue pogonion (Pog’); 8, Soft tissue gnathion (Gn’); 9, Stomion (Sto); 10, Stomion inferius (Stoi); 11, Stomion superius (Stos); 12, Sub- nasale (Sn); 13, Supramentale (Sm). plane of the maxillary and mandibular bases in relation to the cranium. 11) Ao-Bo/FH (mm): the horizontal distance between two perpendiculars dropped from points A and B onto FH plane, measuring the anteroposterior relation of the maxillary and mandibular bases relative to the face. 12) Ao-Bo (mm) (Wit’s appraisal): the horizontal dis- C opyright © 2011 SciRes. OJST  H. M. Abu-Tayyem et al. / Open Journal of Stomatology 1 (2011) 75-83 78 tance between perpendicular lines from point A and B onto the functional occlusal plane, measuring the anter- oposterior relation of the maxillary and mandibular bases relative to the functional occlusal plane. 13) FH/MP (˚) (Frankfort mandibular plane angle): the angle formed between Frankfort horizontal plane and mandibular plane. 14) PP/SN (˚) (Palatal plane angle): the angle formed between anterior cranial base (S-N) and palatal plane (PP). It represents the cant of the maxillary plane in rela- tion to anterior cranial base. 15) MP/SN (˚): the angle formed between the man- dibular plane (Go-Gn) and the anterior cranial base (SN line). It represents the inclination of the mandibular base to the cranium. 16) ANS Xi PM (˚) (Lower face height): this is the angular measurement formed by the intersection of a line from anterior nasal spine to the center of the ramus and the corpus axis. It represents the vertical jaw relation i.e. the depth of the bite. 17) SNA (˚): anteroposterior position of the maxilla (apical base) relative to the anterior cranial base. 18) Co-A (mm): the horizontal distance between condylion and point-A. It represents the effective maxil- lary length. 19) SNB (˚): measuring the anteroposterior position of the mandibular base in relation to the cranium. 20) Pog-Nv (mm): the linear distance between the point Pog and a vertical line drawn from nasion perpen- dicular onto the FH plane. It represents the anteroposte- rior position of the mandibular chin in relation to the face. 21) Co-Gn (mm): the horizontal distance between condylion and point gnathion. It represents the effective mandibular length. Dental angular and linear measurements: 22) U1/L1 (˚) (Inter-incisal angle): the angle between long axes of the upper and lower central incisors. 23) U1/SN (˚): the angle formed between the long axis of upper central incisor and the anterior cranial base. It represents the degree of the inclination of upper incisors relative to the cranium. 24) U1/NA (˚): the angle formed between the long axis of upper central incisor and the NA line. It repre- sents the degree of the inclination of upper incisors rela- tive to the anterior limit of the maxillary base. 25) U1-NA (mm): the linear perpendicular distance from the incisal tip of the most protruded upper central incisor and the N-A line. It represents the degree of the protrusion of upper incisors relative to the anterior limit of the maxillary base. 26) L1-NB (mm): the linear perpendicular distance from the incisal tip of the most protruded lower central incisor and the N-B line. It represents the degree of the protrusion of lower incisors relative to the anterior limit of the mandibular base. 27) L1/NB (˚): the angle between long axis of lower central incisor and NB line. It represents the degree of the inclination of lower incisors relative to the mandibular base. 28) L1/MP (˚): the angle between long axis of lower central incisor and the mandibular plane. It represents the degree of the inclination of lower incisors relative to the mandibular base. Soft tissue angular and linear measurements: 29) H-angle: the angle between soft tissue labrale supe- rious, soft tissue nasion and Pog’. It represents the promi- nence of the upper lip in relation to N’pog’ line. 30) Z-angle: the angle between soft tissue labrale supe- rious, pogonion (profile line) and Frankfort horizontal plane. It represents the amount of lip protrusion. 31) N’SnPog’ (˚) (soft tissue profile): It represents the degree of soft tissue convexity regardless the nose promi- nence. 32) N’PnPog’ (˚) (soft tissue convexity): It represents the degree of soft tissue convexity including the nose. 33) PnN’Sn (˚) (Nasal prominence): It represents the degree the nasal prominence. 34) Sn-Stos (mm) (length of upper lip): the length of the upper lip measured between subnasale and stomion superius. 35) Stoi-Sm (mm) (length of lower lip): the length of the lower lip measured between stomion and mentolabial sulcus. 36) Ls-E line (mm): The horizontal distance between labrale superious and esthetic line. It represents the rela- tive protrusion of the upper lip to the esthetic line. 37) Li-E line (mm): The horizontal distance between labrale inferius and esthetic line. It represents the relative protrusion of the lower lip to the esthetic line. 38) Pog-Pog’ (mm) (thickness of the soft tissue chin): the horizontal distance between the hard and soft tissue pogonion. 39) Ls-SnPog’ (mm) (upper lip protrusion): The hori- zontal distance between the most anterior point of the upper lip and subnasale soft tissue pogonion line. It represents the relative protrusion or retrusion of the upper lip to the SnPog’ line. 40) Li-SnPog’ (mm) (lower lip protrusion): The hori- zontal distance between the most anterior point of the lower lip and subnasale soft tissue pogonion line. It represents the relative protrusion or retrusion of the lower lip to the SnPog’ line. 3. RESULTS Means and standard deviations of cephalometric meas- urements for Emirates adults are shown in Table 1. A C opyright © 2011 SciRes. OJST 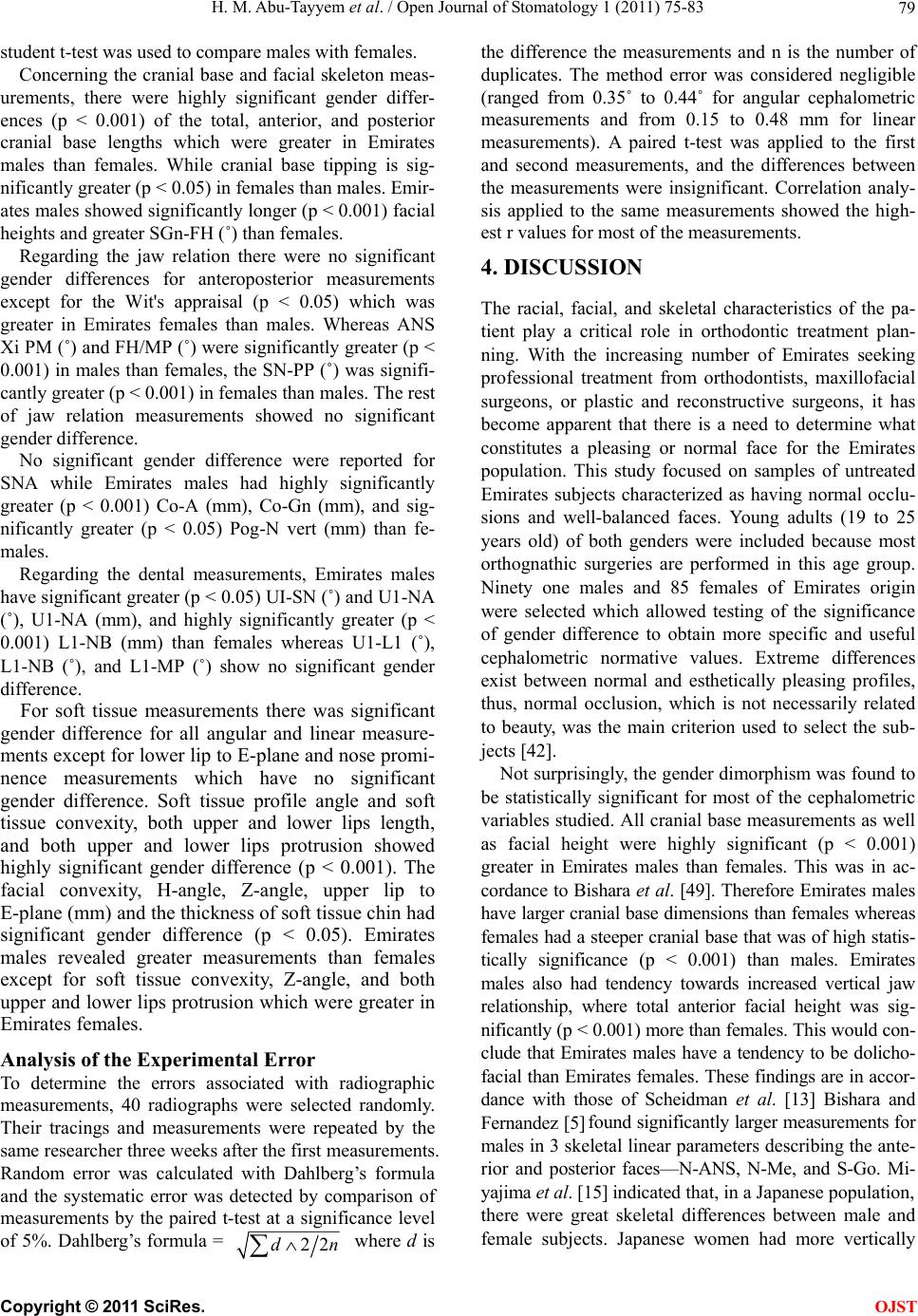 H. M. Abu-Tayyem et al. / Open Journal of Stomatology 1 (2011) 75-83 Copyright © 2011 SciRes. 79 student t-test was used to compare males with females. Concerning the cranial base and facial skeleton meas- urements, there were highly significant gender differ- ences (p < 0.001) of the total, anterior, and posterior cranial base lengths which were greater in Emirates males than females. While cranial base tipping is sig- nificantly greater (p < 0.05) in females than males. Emir- ates males showed significantly longer (p < 0.001) facial heights and greater SGn-FH (˚) than females. Regarding the jaw relation there were no significant gender differences for anteroposterior measurements except for the Wit's appraisal (p < 0.05) which was greater in Emirates females than males. Whereas ANS Xi PM (˚) and FH/MP (˚) were significantly greater (p < 0.001) in males than females, the SN-PP (˚) was signifi- cantly greater (p < 0.001) in females than males. The rest of jaw relation measurements showed no significant gender difference. OJST No significant gender difference were reported for SNA while Emirates males had highly significantly greater (p < 0.001) Co-A (mm), Co-Gn (mm), and sig- nificantly greater (p < 0.05) Pog-N vert (mm) than fe- males. Regarding the dental measurements, Emirates males have significant greater (p < 0.05) UI-SN (˚) and U1-NA (˚), U1-NA (mm), and highly significantly greater (p < 0.001) L1-NB (mm) than females whereas U1-L1 (˚), L1-NB (˚), and L1-MP (˚) show no significant gender difference. For soft tissue measurements there was significant gender difference for all angular and linear measure- ments except for lower lip to E-plane and nose promi- nence measurements which have no significant gender difference. Soft tissue profile angle and soft tissue convexity, both upper and lower lips length, and both upper and lower lips protrusion showed highly significant gender difference (p < 0.001). The facial convexity, H-angle, Z-angle, upper lip to E-plane (mm) and the thickness of soft tissue chin had significant gender difference (p < 0.05). Emirates males revealed greater measurements than females except for soft tissue convexity, Z-angle, and both upper and lower lips protrusion which were greater in Emirates females. Analysis of the Experimental Error To determine the errors associated with radiographic measurements, 40 radiographs were selected randomly. Their tracings and measurements were repeated by the same researcher three weeks after the first measurements. Random error was calculated with Dahlberg’s formula and the systematic error was detected by comparison of measurements by the paired t-test at a significance level of 5%. Dahlberg’s formula = 22d n where d is the difference the measurements and n is the number of duplicates. The method error was considered negligible (ranged from 0.35˚ to 0.44˚ for angular cephalometric measurements and from 0.15 to 0.48 mm for linear measurements). A paired t-test was applied to the first and second measurements, and the differences between the measurements were insignificant. Correlation analy- sis applied to the same measurements showed the high- est r values for most of the measurements. 4. DISCUSSION The racial, facial, and skeletal characteristics of the pa- tient play a critical role in orthodontic treatment plan- ning. With the increasing number of Emirates seeking professional treatment from orthodontists, maxillofacial surgeons, or plastic and reconstructive surgeons, it has become apparent that there is a need to determine what constitutes a pleasing or normal face for the Emirates population. This study focused on samples of untreated Emirates subjects characterized as having normal occlu- sions and well-balanced faces. Young adults (19 to 25 years old) of both genders were included because most orthognathic surgeries are performed in this age group. Ninety one males and 85 females of Emirates origin were selected which allowed testing of the significance of gender difference to obtain more specific and useful cephalometric normative values. Extreme differences exist between normal and esthetically pleasing profiles, thus, normal occlusion, which is not necessarily related to beauty, was the main criterion used to select the sub- jects [42]. Not surprisingly, the gender dimorphism was found to be statistically significant for most of the cephalometric variables studied. All cranial base measurements as well as facial height were highly significant (p < 0.001) greater in Emirates males than females. This was in ac- cordance to Bishara et al. [49]. Therefore Emirates males have larger cranial base dimensions than females whereas females had a steeper cranial base that was of high statis- tically significance (p < 0.001) than males. Emirates males also had tendency towards increased vertical jaw relationship, where total anterior facial height was sig- nificantly (p < 0.001) more than females. This would con- clude that Emirates males have a tendency to be dolicho- facial than Emirates females. These findings are in accor- dance with those of Scheidman et al. [13] Bishara and Fernandez [5] found significantly larger measurements for males in 3 skeletal linear parameters describing the ante- rior and posterior faces—N-ANS, N-Me, and S-Go. Mi- yajima et al. [15] indicated that, in a Japanese population, there were great skeletal differences between male and female subjects. Japanese women had more vertically  H. M. Abu-Tayyem et al. / Open Journal of Stomatology 1 (2011) 75-83 80 Table 1. Comparison between cephalometric measurements of Emirates males and females. Emirates males (n = 91) Emirates females (n = 85) Variables Mean SD Mean SD t-test P-value Skeletal Ba-N (mm) 88.95 3.51 71.54 1.60 4.94 <0.001** S-N (mm) 45.56 4.08 36.95 1.77 4.38 <0.001** S-Ar (mm) 135.35 5.57 112.17 3.89 3.88 <0.001** FH-SN (˚) 6.48 3.73 8.56 2.03 –3.56 <0.001** N-Me (mm) 164.25 5.55 131.93 8.95 4.55 <0.001** N-ANS (mm) 64.29 9.22 55.02 5.54 3.51 <0.001** ANS-Me(mm) 87.07 3.63 68.44 8.69 4.83 <0.001** S-Go (mm) 100.48 3.23 80.18 2.58 4.71 <0.001** SGn-FH (˚) 60.03 4.67 57.54 4.23 3.69 <0.001** ANB (˚) 2.03 1.65 1.82 1.53 0.85 >0.05 Ao-Bo /FH (mm) 5.44 1.39 4.26 2.47 1.21 >0.05 Ao-Bo (mm) –0.47 2.46 –1.31 2.66 2.21 <0.05* FH/MP (˚) 25.44 4.54 23.17 6.01 2.38 <0.05* MP-SN (°) 31.95 6.47 31.71 6.11 0.26 >0.05 SN-PP (˚) 5.77 3.77 7.87 3.17 –4 <0.001** ANS Xi PM (˚) 45.36 3.90 42.61 4.75 4.18 <0.001** SNA (˚) 81.40 2.82 81.14 3.09 0.59 >0.05 Co-A (mm) 112.28 4.14 94.12 4.84 3.58 <0.001** SNB (˚) 80.52 2.27 79.75 3.57 1.71 >0.05 Pog-N vert (mm) –4.23 1.57 –1.95 3.34 –2.16 <0.05* Co-Gn (mm) 156.03 5.84 128.10 5.02 4.10 <0.001** Dental U1-L1 (˚) 120.01 9.38 121.08 6.87 –0.52 >0.05 UI-SN (˚) 111.49 6.80 108.63 6.31 2.89 <0.05* U1-NA (˚) 29.20 1.09 26.55 5.86 2.11 <0.05* U1-NA (mm) 7.64 2.43 6.05 2.23 2.71 <0.05* L1-NB (˚) 29.82 5.39 28.58 5.09 1.57 >0.05 L1-NB (mm) 8.47 2.74 5.87 2.91 3.73 <0.001** L1-MP (˚) 96.73 5.46 96.66 7.40 0.07 >0.05 Soft tissue H-Angle 14.56 4.46 12.98 3.84 2.51 <0.05* Z-Angle 74.08 8.99 78 7.89 –3.06 <0.05* N’SnPog’ (˚) 156.91 6.92 133.79 5.51 3.81 <0.001** N’PnPog’ (˚) 127.48 4.78 136.85 8.03 –4.64 <0.001** PnN’Sn (˚) 19.99 2.22 20.73 6.29 –1.01 >0.05 Sn-Stos (mm) 27.09 1.53 16.79 2.35 5.92 <0.001** Stoi-Sm (mm) 25 2.49 21 5.86 6.56 <0.001** Ls-E line (mm) –5.88 3.56 –1.80 4.03 –2.60 <0.05* Li-E line (mm) –2.23 4.41 –1.32 4.42 –1.36 >0.05 Pog-Pog’ (mm) 14.50 7.12 11.48 7.24 2.79 <0.05* Ls-SnPog’ (mm) 3.47 2.20 12.01 2.66 –3.96 <0.001** Li-SnPog’ (mm) 3.72 2.68 11.74 2.16 –3.80 <0.001** p = Probability level, not significant. = p > 0.05, * significant = p ≤ 0.05, ** significant = p ≤ 0.01, *** highly significant = p ≤ 0.001. * Student t-test. oriented facial axis angles, greater mandibular plane angles, and smaller midfacial lengths, and they were more protrusive relative to the nasion perpendicular. Regarding facial growth pattern, the Y-axis with FH plane angle was significantly greater (p < 0.001) in males. Therefore, Emirates males have more tendency to vertical growth pattern (backward mandibular rotation) than Emirates females as further evidenced by the sig- nificant (p < 0.05) increase of FMA and the high sig- nificant (p < 0.001) increase of ANS Xi PM angle. These findings are agreed with those of Park et al. [37] and Bishara et al. [49]. Accordingly, the results again explain the tendency of Emirates males to be more dolichofacial than females. C opyright © 2011 SciRes. OJST  H. M. Abu-Tayyem et al. / Open Journal of Stomatology 1 (2011) 75-83 81 No significant difference was found between males and females regarding the angular and linear measure- ments of the anteroposterior jaw relationship. These findings are agreed with those of Park et al. [37]. Whereas, Wits appraisal was significantly greater (p < 0.05) in males which could be attributed to the steeper maxilla in females as evidenced by SN-PP (˚), rather than discrepancy between upper and lower jaws. Maxil- lary and mandibular anteroposterior positions was sl- ightly more in males but of no significance but the chin position was significantly (p < 0.05) more retruded in males (Pog-Nv mm). Thus, regarding skeletal facial convexity, Emirates males have more convex profiles than females, due to retruded chin, rather than retrog- nathic mandible or prognathic maxilla. These findings are also disagreed with those of Park et al. [37] and Scheidman et al. [11]. Moreover, maxillary and man- dibular sagittal lengths were highly significantly (p < 0.001) longer in Emirates male than females. These findings disagreed with those of Scheidman et al. [11]. This increase in size of jaws in males is coincident with their larger skeletal features of skull than Emirates fe- males. Concerning dental measurements, Emirates males showed significantly (p < 0.05) more proclined upper and lower incisors than females as indicated by the rela- tionship of the maxillary and mandibular incisors to the SN, MP, NA, and NB lines. So, Normal angulation of incisors should be taken into consideration, when incisor retraction is planned in orthodontic treatment of Emir- ates adults. In their study, Swlerenga et al. [36] found that Mexican American males and females have greater mandibular incisor proclination than black American or white chil- dren, and that maxillary incisor inclination of Mexican American women is more retroclined than that of black or white women. Miyajima et al. [25] found mandibular dentoalveolar protrusion in the Japanese men compared with European-American adults. No statistically sig- nificant gender dimorphism was found in the dental measurements of both Anatolian Turkish [42] and Japa- nese adults [25]. Most probably the soft tissue follows hard tissue structures, but could also consolidate them. Regarding soft tissue measurements, Emirates males had signifi- cantly greater (p < 0.001) soft tissue profile angle (N’Sn’Pog’) than females whereas females had more (p < 0.05) soft tissue convexity (N’Pn Pog’) than males. In spite of retruded bony chin, the soft tissue chin (Pog’) was more protruded in males than females, ranging from significant to highly significant. Emirates females had slightly more prominent noses than males, but of no sig- nificance. Accordingly, considering soft tissue profile, females had more convex facial profiles than males, while skeletally males had more convex profiles than females. Upper and lower lip lengths were significantly (p < 0.001) increased in males than females. These find- ings are in accordance with those of Hashim and AlBa- rakati [57] and Scheidman et al. [11]. This was attributed to the greater facial height in males and more to the in- creased lower facial height. The soft tissue of lip fol- lowed the hard tissue of upper and lower jaws. Also re- garding the lip appearance, upper and lower lips were more protrusive in Emirates males than females. This was assured by significant (p < 0.05) increase of H-an- gles, and decreased Z angle in Emirates males. These findings are disagreed with those of Eraby et al. [39]. The lip protrusion followed the difference in protrusion of upper and lower incisors. But on using the E-plane as reference for analyzing lip protrusion, the lips appeared more retrusive in Emirates males. This could be contrib- uted more to soft tissue chin protrusion in males, rather than the actual lips’ procumbency. Along with the clinical examination and other patient records, knowledge of normative cephalometric values of normal samples from different ethnic groups can be helpful for planning orthodontic or orthognatic surgery. However, these normal data should not be used as a template. Orthodontic and orthognathic treatment should always be planned according to each patient’s needs and desires. From the previous findings it is recommended to use the lateral cephalometric norms of the present study as a reference for orthodontic diagnosis and treatment planning of Emirates adults, separate for gender. 5. CONCLUSIONS Emirates adults have distinct cephalometric features, which should be used as a reference in treating Emirates orthodontic patients. Skeletally, Emirates adult males showed longer total, anterior, and posterior cranial base lengths, indicating larger cranial base; longer facial heights, greater vertical jaw relation (more tendency to be dolichocephalic),and longer midfacial and mandibular lengths than females. Dentally, Emirates adult males demonstrated more proclined upper and lower incisors than females. Considering soft tissue profile, Emirates females had more convex facial profiles than males, while skeletally males had more convex profiles than females. Emirates males had greater upper and lower lip lengths and soft tissue profile angle due to a greater soft tissue chin thickness, whereas females had a greater soft tissue profile convexity due to greater nasal prominence. The results of the present study support the view that the norms of specific population should be used as ref- erence for successful orthodontic treatment and not ap- C opyright © 2011 SciRes. OJST  H. M. Abu-Tayyem et al. / Open Journal of Stomatology 1 (2011) 75-83 82 plied to different populations. REFERENCES [1] Broadbent, B.H. (1931) A new X-ray technique and its application to orthodontia. Angle Orthodontist, 1, 45-66. [2] Hofrath, H. (1931) Die bedeutung der roentgenfern der kiefer anomalien. Fortschr Orthodontic, 1, 232-248. [3] Athanasiou, A. (1997) Orthodontic cephalometry. Mosby- Wolfe, London. [4] Bishara, S.E., Jacobsen, J.R., Hession, T.J. and Treder, J.E. (1998) Soft tissue profile changes from 5 to 45 years of age. American Journal of Orthodontics & Dentofacial Orthopedics, 114, 698-706. doi:10.1016/S0889-5406(98)70203-3 [5] Bishara, S.E. and Fernandez, A.G. (1985) Cephalometric comparisons of the dentofacial relationships of two ado- lescent populations from Iowa and Northern Mexico. American Journal of Orthodontics, 88, 314-322. doi:10.1016/0002-9416(85)90131-9 [6] Downs, W.B. (1956) Analysis of the dentofacial profile. Angle Orthodontist, 26, 191-212. [7] Downs, W.B. (1948) Variation in facial relationships: Their significance in the treatment and prognosis. Ameri- can Journal of Orthodontics, 34, 812-840. [8] Riedel, R.A. (1952) The relation of maxillary structures to cranium in malocclusion and in normal occlusion. An- gle Orthodontist, 22, 142-145. [9] Steiner, C.C. (1953) Cephalometrics for you and me. American Journal of Orthodontics, 39, 729-755. doi:10.1016/0002-9416(53)90082-7 [10] Bishara, S.E. (1981) Longitudinal cephalometric stan- dards from 5 years of age to adulthood. American Jour- nal of Orthodontics 1981, 79, 35-44. [11] Scheideman, G.B., Bell, W.H., Legan, H.L., Finn, R.A. and Reisch, J.S. (1980) Cephalometric analysis of dento- facial normals. American Journal of Orthodontics, 78, 404-420. [12] Argyropoulos, E. and Sassouni, V. (1989) Comparison of the dentofacial patterns for native Greek and Ameri- can-Caucasian adolescents. American Journal of Ortho- dontics & Dentofacial Orthopedics, 95, 238-249. [13] Franchi, L., Baccetti, T. and McNamara, J.A. Jr. (1998) Cephalometric floating norms for North American adults. Angle Orthodontist, 68, 497-502. [14] Farkas, L.G., Tompson, B., Phillips, J.H., Katic, M.J. and Cornfoot, M.L. (1999) Comparison of anthropometric and cephalometric measurements of the adult face. Jour- nal of Craniofacial Surgery, 10, 18-25. [15] Huang, W.J., Taylor, R.W. and Dasanayake, A.P. (1998) Determining cephalometric norms for Caucasians and African Americans in Birmingham. Angle Orthodontist, 68, 503-512. [16] Drummond, R.A. (1968) A determination of cephalomet- ric norms for the Negro race. American Journal of Or- thodontics, 54, 670-682. doi:10.1016/0002-9416(68)90018-3 [17] Fonseca, R.J. and Klein, W.D. (1978) A cephalometric evaluation of American Negro women. American Jour- nal of Orthodontics, 73, 152-160. doi:10.1016/0002-9416(78)90185-9 [18] Cotton, W.N., Takano, W.S. and Wong, W. (1951) The Downs analysis applied to three other ethnic groups. An- gle Orthodontist, 21, 213-220. [19] Richardson, E.R. (1980) Racial differences in dimen- sional traits of the human face. Angle Orthodontist, 50, 301-311. [20] Kapila, S. (1989) Selected cephalometric angular norms in Kikuyu children. Angle Orthodontist, 59, 139-144. [21] Jacobson, A. (1978) The craniofacial skeletal pattern of the South African Negro. American Journal of Ortho- dontics, 73, 681-691. doi:10.1016/0002-9416(78)90229-4 [22] Bacon, W., Girardin, P. and Turlot, J.C. (1983) A com- parison of cephalometric norms for the African Bantu and a Caucasoid population. European Journal of Or- thodontics, 5, 233-240. [23] Anderson, A.A., Anderson, A.C., Hornbuckle, A.C. and Hornbukle, K. (2000) Biological derivation of a range of cephalometric norms for children of African American descent (after Steiner). American Journal of Orthodon- tics & Dentofacial Orthopedics, 118, 90-100. [24] Bailey, K.L. and Taylor, R.W. (1998) Mesh diagram cephalometric norms for Americans of African descent. American Journal of Orthodontics & Dentofacial Or- thopedics, 114, 218-223. [25] Miyajima, K., McNamara, J.A. Jr, Kimura, T., Murata, S. and Iizuka, T. (1996) Craniofacial structure of Japanese and European-American adults with normal occlusions and well-balanced faces. American Journal of Orthodon- tics & Dentofacial Orthopedics, 110, 431-438. [26] Engel, G. and Spolter, B.M. (1981) Cephalometric and visual norms for a Japanese population. American Jour- nal of Orthodontics, 80, 48-60. [27] Kondo, S., Wakatsuki, E. and Shibagaki, H. (1999) A somatometric study of the head and face in Japanese adolescents. Okajimas Folia Anatomica Japonica, 76, 179-185. [28] Alcalde, R.E., Jinno, T., Pogrel, M.A. and Matsumura, T. (1998) Cephalometric norms in Japanese adults. Journal of Oral and Maxillofacial Surgery, 56, 129-134. [29] Ioi, H., Nakata, S., Nakasima, A. and Counts, A.L. (2007) Comparison of cephalometric norms between Japanese and Caucasian adults in antero-posterior and vertical di- mension. European Journal of Orthodontics, 29, 493-499. doi:10.1093/ejo/cjm059 [30] Yen, P.K.J. (1973) The facial configuration in a sample of Chinese males. Angle Orthodontist, 43, 301-304. [31] Cooke, M.S. and Wei, S.H.Y. (1988) Cephalometric “standards” for the southern Chinese. European Journal of Orthodontics, 10, 264-272. [32] Lew, K.K., Ho, K.K., Keng, S.B. and Ho, K.H. (1992) Soft tissue cephalometric norms in Chinese adults with esthetic facial profiles. Journal of Oral and Maxillofacial Surgery, 50, 1184-1190. doi:10.1016/0278-2391(92)90151-O [33] Wu, J., Hagg, U. and Rabie, A.B. (2007) Chinese norms of McNamara’s cephalometric analysis. Angle Orthodon- tist, 77, 12-20. doi:10.2319/021606-62R.1 [34] Obloj, B., Fudalej, P. and Dudkiewicz, Z. (2008) Cepha- lometric standards for Polish 10-year-olds with normal occlusion. Angle Orthodontist, 78, 262-269. doi:10.2319/011207-14.1 C opyright © 2011 SciRes. OJST  H. M. Abu-Tayyem et al. / Open Journal of Stomatology 1 (2011) 75-83 Copyright © 2011 SciRes. 83 OJST [35] Moldez, M.A., Sato, K., Sugawara, J. and Mitani, H. (2006) Linear and angular Filipino cephalometric norms according to age and gender. Ang le Orthodontist, 76, 800- 805. [36] Swierenga, D., Oesterle, L.G. and Messersmith, M.L. (1994) Cephalometric values for adult Mexican Ameri- cans. American Journal of Orthodontics & Dentofacial Orthopedics, 106, 146-155. doi:10.1016/S0889-5406(94)70032-X [37] Park, I., Bowman, D. and Klapper, L. (1989) Cepha- lometric study of Korean adults. American Journal of Orthodontics & Dentofacial Orthopedics, 96, 54-59. doi:10.1016/0889-5406(89)90229-1 [38] Hwang, H.S., Kim, W.S. and McNamara, J.A. Jr. (2002) Ethnic differences in the soft tissue profile of Korean and European-American adults with normal occlusions and well-balanced faces. Angle Orthodontist, 72, 72-80. [39] Erbay, E.F., Canikliog˘lu, C.M. and Erbay, S.K. (2002) Soft tissue profile in Anatolian Turkish adults: Part I. Evaluating of horizontal lip position using different soft tissue analyses. American Journal of Orthodontics & Dentofacial Orthopedics, 121, 57-64. doi:10.1067/mod.2002.119780 [40] Erbay, E.F. and Canikliog˘lu, C.M. (2002) Soft tissue profile in Anatolian Turkish adults: Part II. Comparison of different soft tissue analyses in the evaluation of beauty. American Journal of Orthodontics & Dentofacial Orthopedics, 121, 65-72. doi:10.1067/mod.2002.119573 [41] Basciftci, F.A., Uysal, T. and Buyukerkmen, A. (2003) Determination of Holdaway soft tissue norms in Anato- lian Turkish adults. American Journal of Orthodontics & Dentofacial Orthopedics, 123, 395-400. doi:10.1067/mod.2003.139 [42] Basciftci, F.A., Uysal, T. and Buyukerkmen, A. (2004) Craniofacial structure of Anatolian Turkish adults with normal occlusions and well-balanced faces. American Journal of Orthodontics & Dentofacial Orthopedics, 125, 366-372. doi:10.1016/j.ajodo.2003.04.004 [43] Nanda, R. and Nanda, R.S. (1969) Cephalometric study of the dentofacial complex of North Indians. Angle Or- thodontist, 39, 22-28. [44] Cerci, V., Martins, J.E. and de Oliveira, M.A. (1993) Cephalometric standards for white Brazilians. The Inter- national Journal of Adult Orthodontics & Orthogathic Surgery, 8, 287-292. [45] Evanko, A.M., Freeman, K. and Cisneros, G.J. (1997) Mesh diagram analysis: Developing a norm for Puerto Rican Americans. Angle Orthodontist, 67, 381-388. [46] Hajighadimi, M., Dougherty, H.L. and Garakani, F. (1981) Cephalometric evaluation of Iranian children and its comparison with Tweed’s and Steiner’s standards. American Journal of Orthodontics, 79, 192-197. doi:10.1016/0002-9416(81)90317-1 [47] Loutfy, M.S., Ponitz, P. and Harris, J.E. (1971) Cepha- lometric standards for normal Egyptian face. Egyptian Dental Journal, 17, 91-100. [48] Shehata, F.I. (1982) Bimaxillary prognathism in the Nu- bian people of Egypt. Angle Orthodontist, 52, 19-25. [49] Bishara, S.E., Abdalla, E.M. and Hoppens, B.J. (1990) Cephalometric comparisons of dentofacial parameters be- tween Egyptian and North American adolescents. Ameri- can Journal of Orthodontics & Dentofacial Orthopedics, 97, 413-421. [50] Mouakeh, M. (2001) Cephalometric evaluation of cra- niofacial pattern of Syrian children with Class III maloc- clusion. American Journal of Orthodontics & Dentofa- cial Orthopedics, 119, 640-649. [51] Hamdan, A.M. and Rock, W.P. (2001) Cephalometric norms in an Arabic population. Journal of Orthodontics, 28, 297-300. [52] Shalhoub, S.Y., Sarhan, O.A. and Shaikh, H.S. (1987) Adult cephalometric norms for Saudi Arabians with a comparison of values for Saudi and North American Caucasians. British Journal of Orthodontics, 14, 273-279. [53] Sarhan, O.A. and Nashashibi, I.A. (1988) A comparative study between two randomly selected samples from which to derive standards for craniofacial measurements. Jour- nal of Oral Rehabilitation, 15, 251-255. [54] Al-Jasser, N.M. (2000) Cephalometric evaluation of craniofacial variations in normal Saudi population ac- cording to Steiner analysis. Saudi Medical Journal, 21, 746-750. [55] Al-Jame, B., Artun, J., Al-Azemi, R., Behbehani, F. and Buhamra, S. (2006) Lateral cephalometric norms for ado- lescent Kuwaitis: Hard tissue measurements. Medical Principles and Practice, 15, 91-97. doi:10.1159/000090910 [56] Hassan, A.H. (2006) Cephalometric norms for Saudi adults living in the western region of Saudi Arabia. Angle Orthodontist, 76, 109-113. [57] Hashim, H.A. and AlBarakati, S.F. (2003) Cephalometric soft tissue profile analysis between two different ethnic groups: A comparative study. Journal of Contemporary Dental Practice, 2, 60-73. [58] Al-Gunaid, T., Yamada, K., Yamaki, M. and Saito, I. (2007) Soft-tissue cephalometric norms in Yemeni men. American Journal of Orthodontics & Dentofacial Or- thopedics, 132, e7-e14. [59] Molhave, A. (1958) Sitting and standing posture in man. Ugeskr Laeger, 120, 1516-1518. [60] Solow, B. and Tallgren, A. (1971) Natural head position in standing subjects. Acta Odontologica Scandinavica, 29, 591-607. [61] Siersbaek-Nielsen, S. and Solow, B. (1982) Intra- and interexaminer variability in head posture recorded by dental auxiliaries. American Journal of Orthodontics, 82, 50-57.
|