T. Ashraf-Ganjoei et al. / Open Journal of Obstetrics and Gynecology 1 (2011) 109-112
112
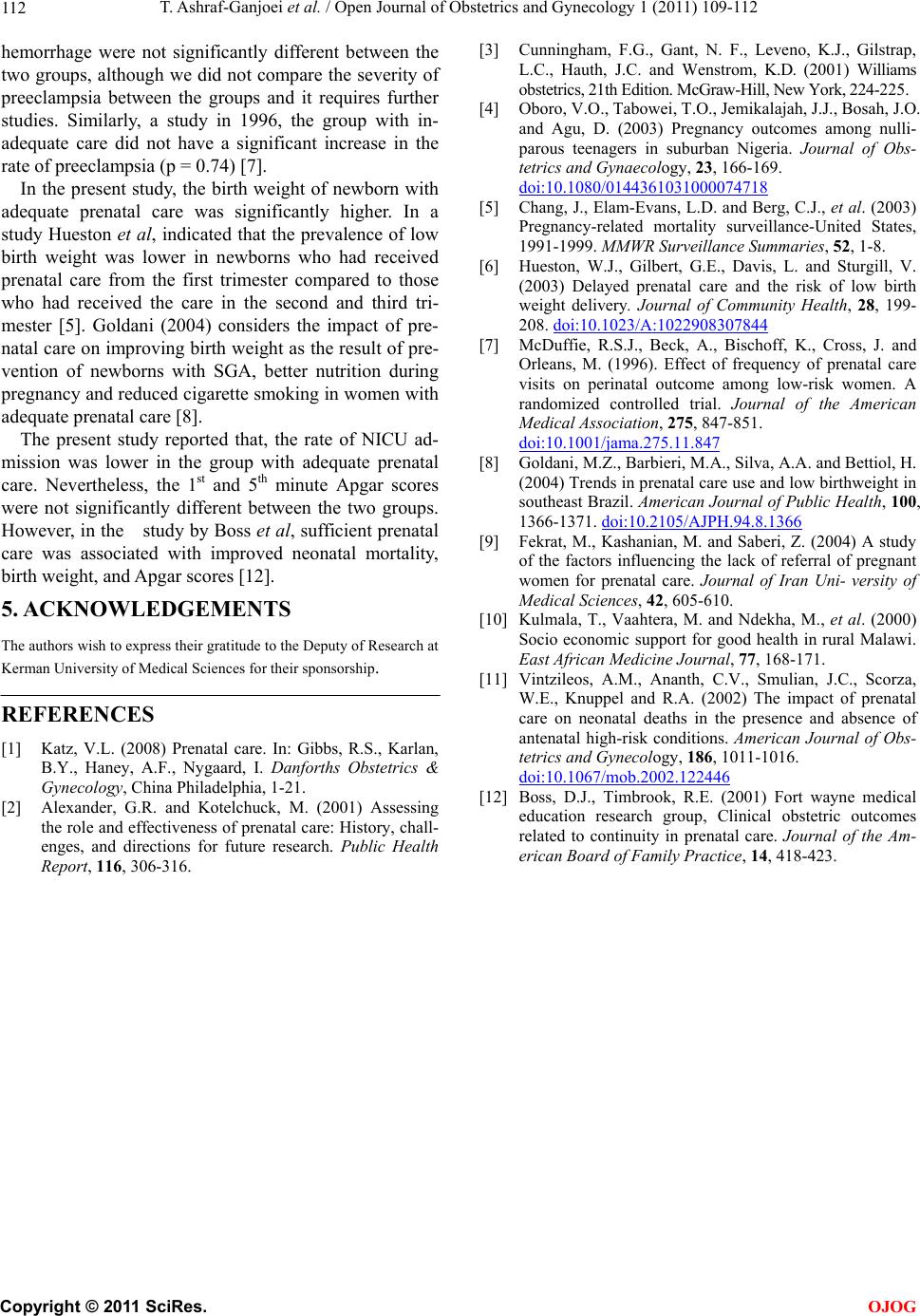
hemorrhage were not significantly different between the
two groups, although we did not compare the severity of
preeclampsia between the groups and it requires further
studies. Similarly, a study in 1996, the group with in-
adequate care did not have a significant increase in the
rate of preeclampsia (p = 0.74) [7].
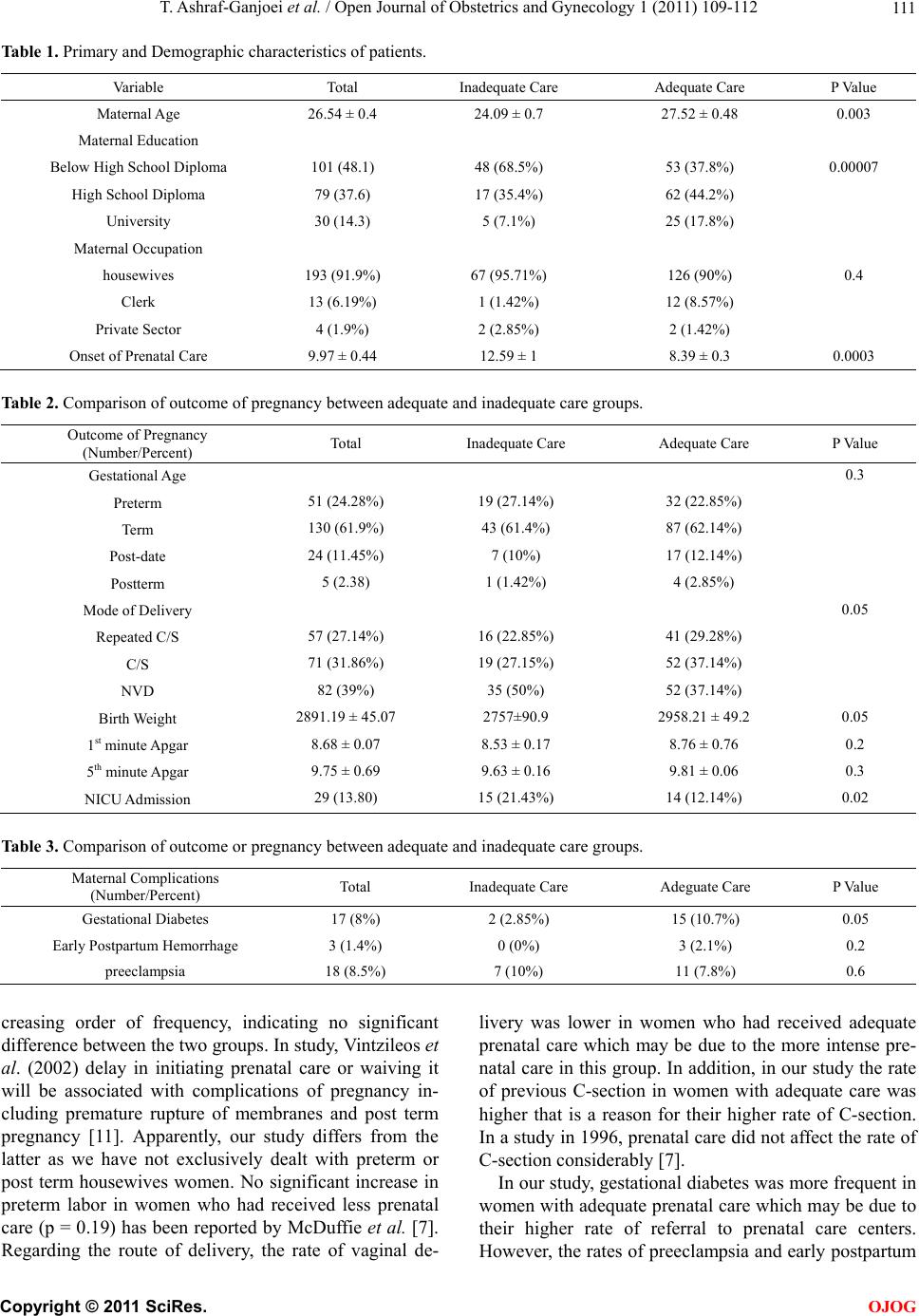
In the present study, the birth weight of newborn with
adequate prenatal care was significantly higher. In a
study Hueston et al, indicated that the prevalence of low
birth weight was lower in newborns who had received
prenatal care from the first trimester compared to those
who had received the care in the second and third tri-
mester [5]. Goldani (2004) considers the impact of pre-
natal care on improving birth weight as the result of pre-
vention of newborns with SGA, better nutrition during
pregnancy and reduced cigarette smoking in women with
adequate prenatal care [8].
The present study reported that, the rate of NICU ad-
mission was lower in the group with adequate prenatal
care. Nevertheless, the 1st and 5th minute Apgar scores
were not significantly different between the two groups.
However, in the study by Boss et al, sufficient prenatal
care was associated with improved neonatal mortality,
birth weight, and Apgar scores [12].
5. ACKNOWLEDGEMENTS
The authors wish to express their gratitude to the Deputy of Research at
Kerman University of Medical Sciences for their sponsorship.
REFERENCES
[1] Katz, V.L. (2008) Prenatal care. In: Gibbs, R.S., Karlan,
B.Y., Haney, A.F., Nygaard, I. Danforths Obstetrics &
Gynecology, China Philadelphia, 1-21.
[2] Alexander, G.R. and Kotelchuck, M. (2001) Assessing
the role and effectiveness of prenatal care: History, chall-
enges, and directions for future research. Public Health
Report, 116, 306-316.
[3] Cunningham, F.G., Gant, N. F., Leveno, K.J., Gilstrap,
L.C., Hauth, J.C. and Wenstrom, K.D. (2001) Williams
obstetrics, 21th Edition. McGraw-Hill, New York, 224-225.
[4] Oboro, V.O., Tabowei, T.O., Jemikalajah, J.J., Bosah, J.O.
and Agu, D. (2003) Pregnancy outcomes among nulli-
parous teenagers in suburban Nigeria. Journal of Obs-
tetrics and Gynaecology, 23, 166-169.
doi:10.1080/0144361031000074718
[5] Chang, J., Elam-Evans, L.D. and Berg, C.J., et al. (2003)
Pregnancy-related mortality surveillance-United States,
1991-1999. MMWR Surveillance Summaries, 52, 1-8.
[6] Hueston, W.J., Gilbert, G.E., Davis, L. and Sturgill, V.
(2003) Delayed prenatal care and the risk of low birth
weight delivery. Journal of Community Health, 28, 199-
208. doi:10.1023/A:1022908307844
[7] McDuffie, R.S.J., Beck, A., Bischoff, K., Cross, J. and
Orleans, M. (1996). Effect of frequency of prenatal care
visits on perinatal outcome among low-risk women. A
randomized controlled trial. Journal of the American
Medical Association, 275, 847-851.
doi:10.1001/jama.275.11.847
[8] Goldani, M.Z., Barbieri, M.A., Silva, A.A. and Bettiol, H.
(2004) Trends in prenatal care use and low birthweight in
southeast Brazil. American Journal of Public Health, 100,
1366-1371. doi:10.2105/AJPH.94.8.1366
[9] Fekrat, M., Kashanian, M. and Saberi, Z. (2004) A study
of the factors influencing the lack of referral of pregnant
women for prenatal care. Journal of Iran Uni- versity of
Medical Sciences, 42, 605-610.
[10] Kulmala, T., Vaahtera, M. and Ndekha, M., et al. (2000)
Socio economic support for good health in rural Malawi.
East African Medicine Journal, 77, 168-171.
[11] Vintzileos, A.M., Ananth, C.V., Smulian, J.C., Scorza,
W.E., Knuppel and R.A. (2002) The impact of prenatal
care on neonatal deaths in the presence and absence of
antenatal high-risk conditions. American Journal of Obs-
tetrics and Gynecology, 186, 1011-1016.
doi:10.1067/mob.2002.122446
[12] Boss, D.J., Timbrook, R.E. (2001) Fort wayne medical
education research grouph, Clinical obstetric outcomes
related to continuity in prenatal care. Journal of the Am-
erican Board of Family Practice, 14, 418-423.
C
opyright © 2011 SciRes. OJOG