S. Lassaad et al. / Open Journal of Pediatrics, 2011, 1, 34-36
Copyright © 2011 SciRes.
36
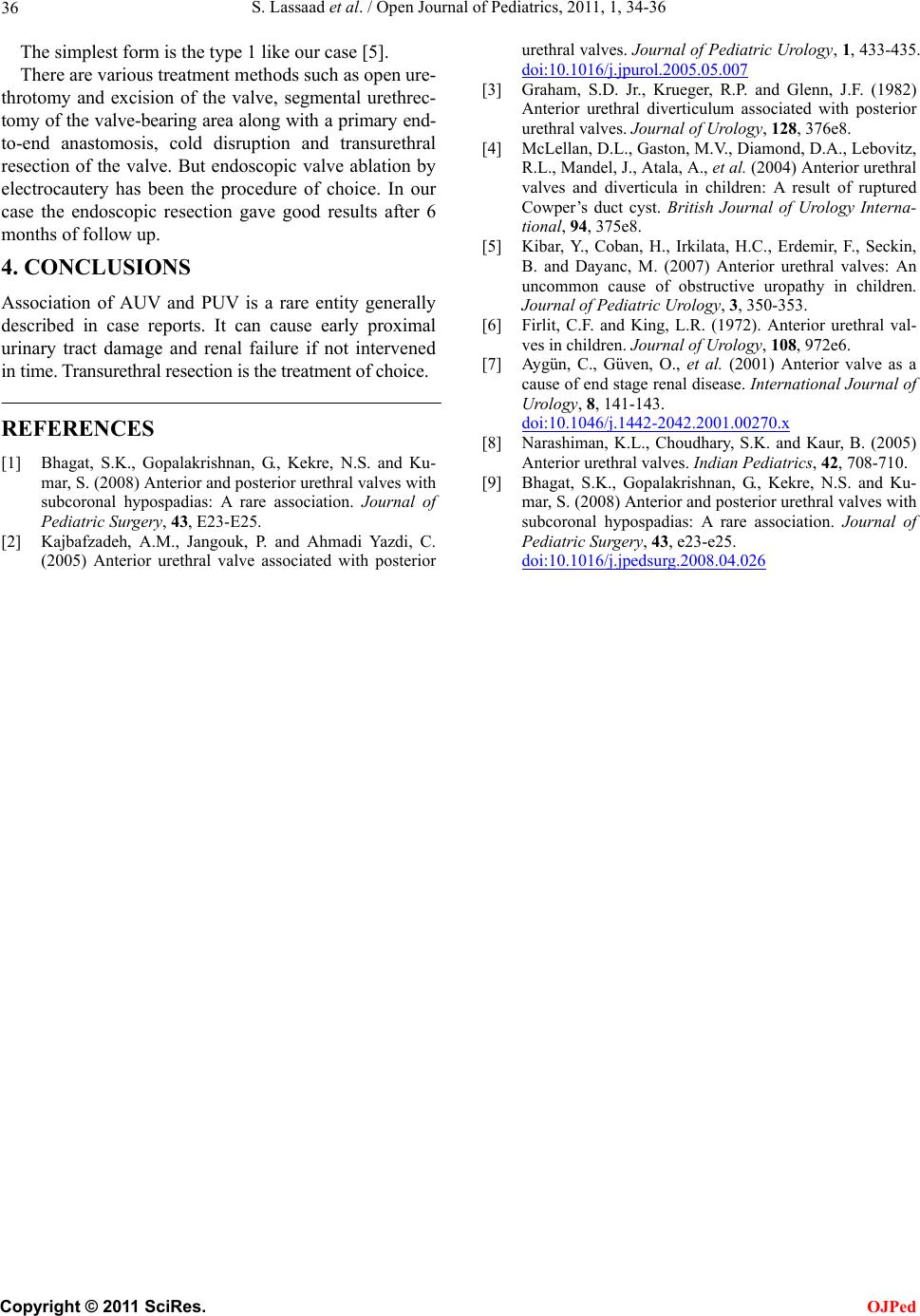
The simplest form is the type 1 like our case [5].
There are various treatment methods such as open ure-
throtomy and excision of the valve, segmental urethrec-
tomy of the valve-bearing area along with a primary end-
to-end anastomosis, cold disruption and transurethral
resection of the valve. But endoscopic valve ablation by
electrocautery has been the procedure of choice. In our
case the endoscopic resection gave good results after 6
months of follow up.
OJPed
4. CONCLUSIONS
Association of AUV and PUV is a rare entity generally
described in case reports. It can cause early proximal
urinary tract damage and renal failure if not intervened
in time. Transurethral resection is the treatment of choice.
REFERENCES
[1] Bhagat, S.K., Gopalakrishnan, G., Kekre, N.S. and Ku-
mar, S. (2008) Anterior and posterior urethral valves with
subcoronal hypospadias: A rare association. Journal of
Pediatric Surgery, 43, E23-E25.
[2] Kajbafzadeh, A.M., Jangouk, P. and Ahmadi Yazdi, C.
(2005) Anterior urethral valve associated with posterior
urethral valves. Journal of Pediatric Urology, 1, 433-435.
doi:10.1016/j.jpurol.2005.05.007
[3] Graham, S.D. Jr., Krueger, R.P. and Glenn, J.F. (1982)
Anterior urethral diverticulum associated with posterior
urethral valves. Journal of Urology, 128, 376e8.
[4] McLellan, D.L., Gaston, M.V., Diamond, D.A., Lebovitz,
R.L., Mandel, J. , Atal a, A., et al. (2004) Anterior urethral
valves and diverticula in children: A result of ruptured
Cowper’s duct cyst. British Journal of Urology Interna-
tional, 94, 375e8.
[5] Kibar, Y., Coban, H., Irkilata, H.C., Erdemir, F., Seckin,
B. and Dayanc, M. (2007) Anterior urethral valves: An
uncommon cause of obstructive uropathy in children.
Journal of Pediatric Urology, 3, 350-353.
[6] Firlit, C.F. and King, L.R. (1972). Anterior urethral val-
ves in children. Journal of Urology, 108, 972e6.
[7] Aygün, C., Güven, O., et al. (2001) Anterior valve as a
cause of end stage renal disease. International Journal of
Urology, 8, 141-143.
doi:10.1046/j.1442-2042.2001.00270.x
[8] Narashiman, K.L., Choudhary, S.K. and Kaur, B. (2005)
Anterior urethral valves. Indian Pediatrics, 42, 708-710.
[9] Bhagat, S.K., Gopalakrishnan, G., Kekre, N.S. and Ku-
mar, S. (2008) Anterior and posterior urethral valves with
subcoronal hypospadias: A rare association. Journal of
Pediatric Surgery, 43, e23-e25.
doi:10.1016/j.jpedsurg.2008.04.026