R. Kitz et al. / Open Journal of Pediatrics, 2011, 1, 21-26 25
eral-fold increased risk for sinusitis, asthma, pneumonia,
and bronchiectasis [12]. Others found a high incidence
of GER in asthmatic pediatric populations [13,14]. Val-
ues of esophageal pH (epH) are the highest in a sub-
group of infants with chronic respiratory disorders un-
dergoing 24-hour pH-monitoring [15]. Studies dealing
with the impact of epHM on respiratory diseases should
reflect these theories and normal values of acid exposure
are of great importance. This is even more important,
since overestimation of GER as a cause of asthma
symptoms may lead to nonjustified therapy of GER as
asthma treatment [16].
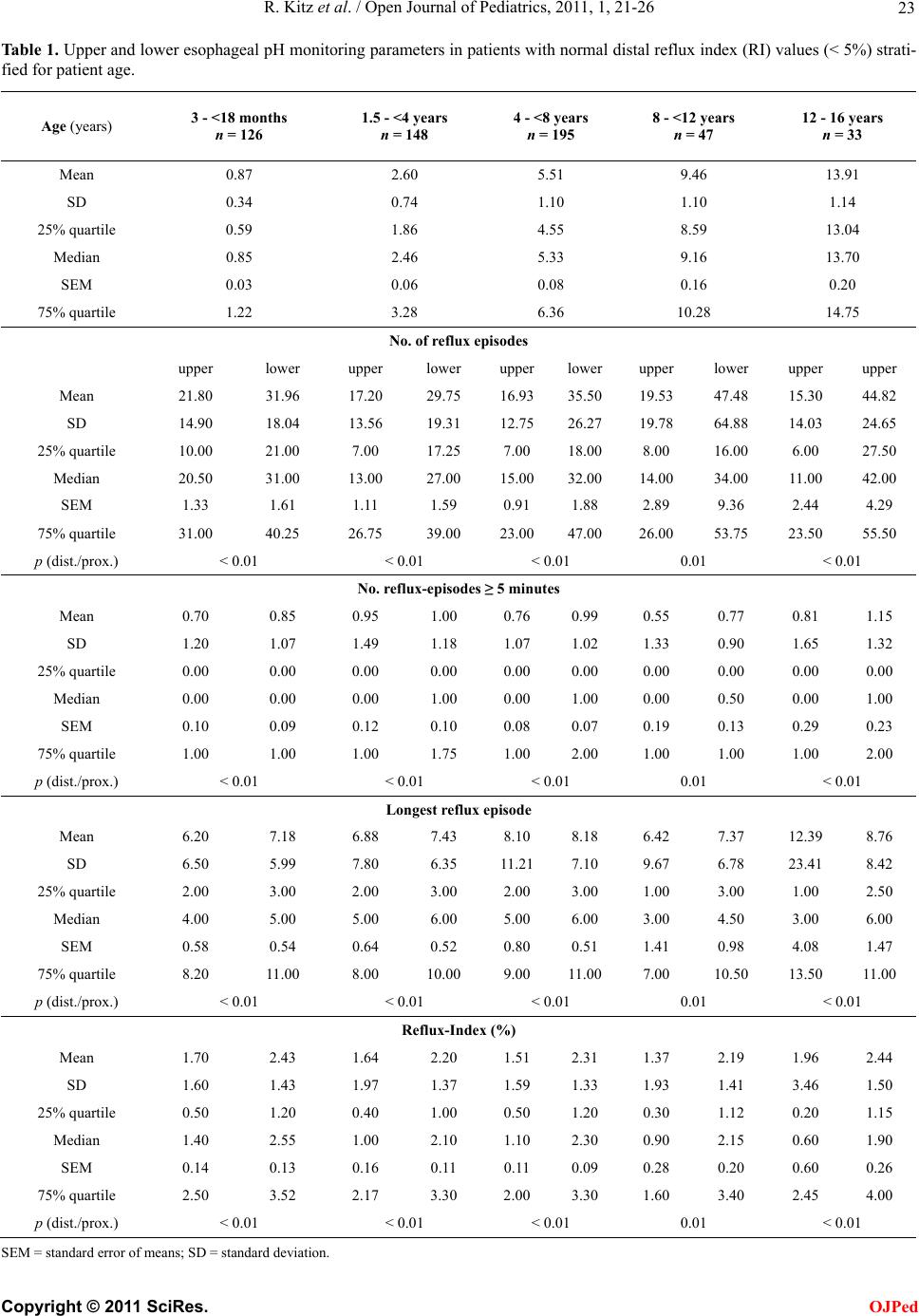
Reference values are mandatory to distinguish be-
tween physiological and pathologic reflux activity. De-
tecting the reflux in the upper esop hagus may be of spe-
cial interest in children with extraesophageal disorders.
While older studies propose the 95th percentile as the
cut-off value [17], more recent publications favor the
SEM as range of normal values [3]. Our study provides
both limits in order to give a solid base for data interpre-
tation. In order to avoid an over-treatment, we recom-
mend the conserv ative approach of taking valu es beyond
the 75th interquartile range as an indication for an anti-
acid treatment.
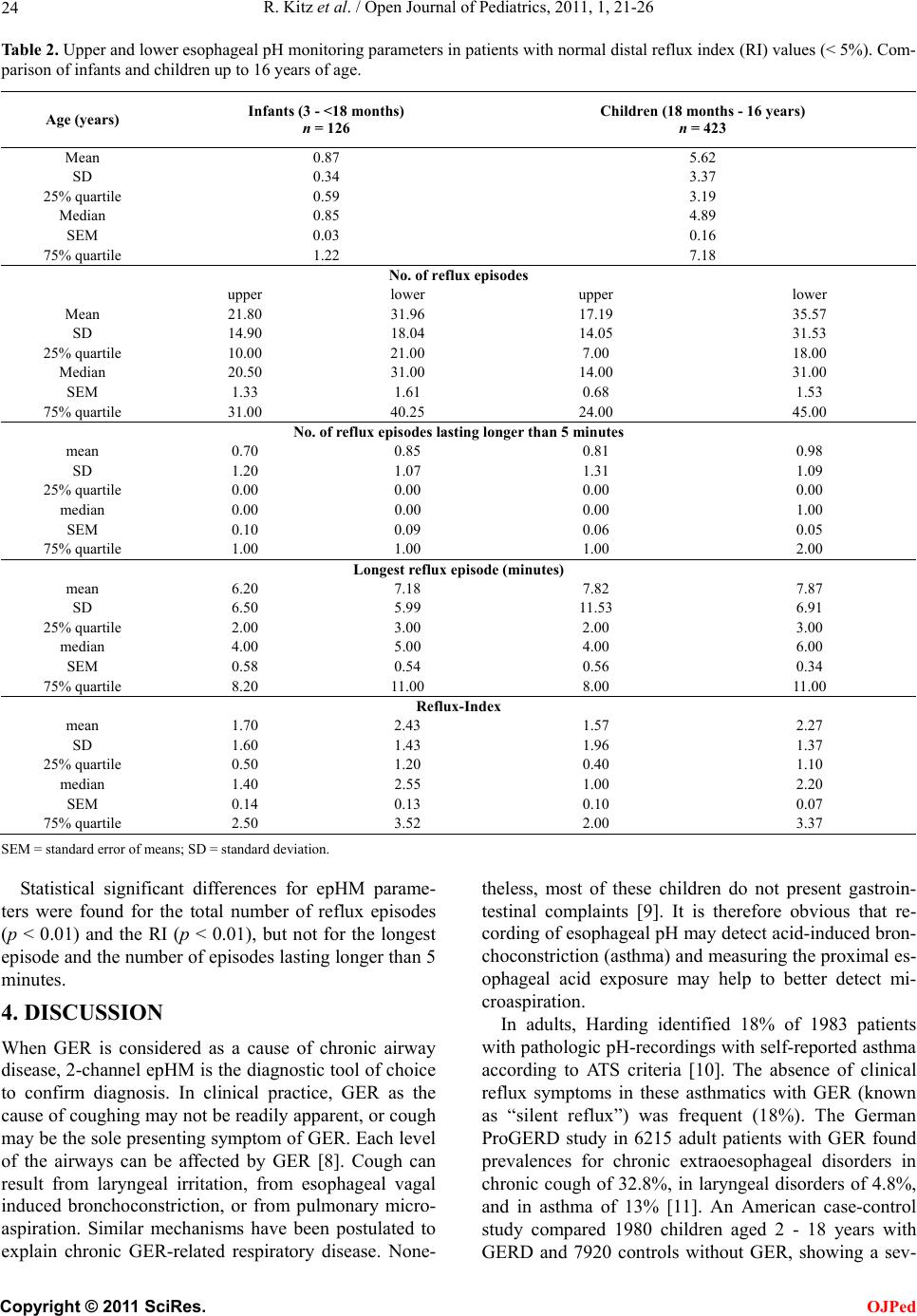
Bagucka et al. [3] published normal data for the upper
esophagus in children initially referred for exclusion of
suspected GER. According to ESPGHAN-recommenda-
tions, they stratified their study group depending on the
RI in the lower esophagus. While their values encom-
passed infants younger than 17 months of age, we now
extended the age range up to 16 year-old adolescents.
When comparing the data, we found consistencies in the
total number of reflux episodes and the absence of epi-
sodes lasting longer than five minutes. Discrepancies
were found for the RI (0.5% vs 1.2%) in the present
study. These findings could be explained by the different
mean ages of the groups < 1.5 years. Bagucka et al.
studied infants as young as 0.5 months old, whereas in
our study no child was younger than 3 months. Their
median age was 3.0 months, whereas our children had a
median age of 10.2 months. Taking into account the
more buffered stomach content of milk-fed children, less
amount of reflux can be detected by measuring only
pH-condition [18]. In other words: the longer the pH in
the stomach is below 4, the more reflux episodes can be
detected in the esophagus. More precisely, simultane-
ously performed intraluminal impedance measurement
of the esophagus can detect bolus movements, thus
broadening our diagnostic spectrum as to detect nonacid
reflux activity in the future [19,20].
Problems in the application of reference values may
occur due to the type of recording device and electrodes.
At present, mostly antimony electrodes are used. They
are less accurate than glass electrodes, however, they
provide multi-channel recording on different levels in
the esophagus and are easier to handle as well as to place
into the esophagus.
5. CONCLUSIONS
The present study prov ides reference values of proximal
esophageal pH-monitoring from infancy to adolescence.
The inter-quartile ranges appear as suitable threshold
levels when anti-acid treatment for the control of re-
flux-associated airway disease is considered.
REFERENCES
[1] Rudolph, C.D., Mazur, L.J., Liptak, G.S., Baker, R.D.,
Boyle, J.T., et al. (2001) Guidelines for evaluation and
treatment of gastroesophageal reflux in infants and chil-
dren: recommendations of the North American Society
for Pediatric Gastroenterology and Nutrition. Journal of
Pediatric Gastroenterology and Nutrition, 32, S1-S31.
doi:10.1097/00005176-200100002-00001
[2] Khoshoo, V., Le, T., Haydel, R.M., Landry, L. and Nelson,
C. (2003) Role of gastroesophageal reflux in older children
with persistent asthma. Chest, 123, 1008-1013.
doi:10.1378/chest.123.4.1008
[3] Bagucka, B., Badriul, H., Vandemaele, K., Troch, E. and
Vandenplas, Y. (2000) Normal ranges of continuous pH-
monitoring in the proximal esophagus. Journal of Pedi-
atric Gastroenterology and Nutrition, 31, 244-247.
doi:10.1097/00005176-200009000-00008
[4] Sondheimer, J.M. and Haase, G.M. (1988) Simultaneous
pH-recordings from multiple sites in children with and
without distal gastroesophageal reflux. Journal of Pedi-
atric Gastroenterology and Nutrition, 7, 46-51.
[5] Gustafsson, P. and Tibbling, L. (1988) 24-hour oeso-
phageal two-level pH-monitoring in healthy children and
adolescents. Scandinavian Journal of Gastroenterology,
23, 91-94.
[6] ESPGHAN—Working Group of the European Society of
Pediatric Gastroenterology, Hepatology and Nutrition
(1992) A standardized protocol for the methodology of
esophageal pH-monitoring and interpretation of data for
the diagnosis of gastroesophageal reflux. Journal of Pe-
diatric Gastroenterology and Nutrition, 14, 467-471.
[7] Ahrens, P., Haas, S. and Kitz, R. (2003) Standardization
and optimization of 2-channel pH-monitoring in children
with gastroesophageal reflux-associated pulmonary dis-
ease. Monatsschrift Kinderheilkunde, 151, 1298-1305.
doi:10.1007/s00112-003-0843-6
[8] Dobhan, R. and Castell, D.O. (1993) Normal and abnormal
proximal esopha geal acid exposure: Results of am bulatory
dual-probe pH-monitoring. The American Journal of Gas-
troenterology, 88, 25-29.
[9] Gorenstein, A., Levine, A., Boaz, M., Mandelberg, A.
and Serour, F. (2003) Severity of acid gastroesophageal
reflux assessed by pH metry: Is it associated with respi-
ratory disease? Pediatric Pulmonology, 36, 330-334.
doi:10.1002/ppul.10361
[10] Harding, S.M., Guzzo, M.R. and Richter, J.E. (1999)
24-h Esophageal pH-Testing in Asthmatics. Chest, 115,
C
opyright © 2011 SciRes. OJPed