Health
Vol. 4 No. 2 (2012) , Article ID: 17486 , 6 pages DOI:10.4236/health.2012.42014
Quality of life, elderly and physical activity
![]()
1Biosciences of Human Motricity Laboratory, Labimh/Unirio, Rio de Janeiro, Brazil; *Corresponding Author: karlos.pernambuco@hotmail.com
2Latin American Development Group for Maturity (GDLAM), Rio de Janeiro, Brazil
3Postgraduate Program in Nursing and Biosciences, Universidade Federal do Estado do Rio de Janeiro, Rio de Janeiro, Brazil
4Universidade Trás os Montes e Alto Douro, Vila Real, Portugal
Received 27 October 2011; revised 18 December 2011; accepted 26 December 2011
Keywords: Quality of Life; Aged; Motor Activity; Exercise
ABSTRACT
The concept of quality of life is multiple concerns as a cultural, social and environmental individuality. The aim of this study was to verify the levels of quality of life in elderly practitioners of physical activity comparing a active group with a control group The sample consisted of 159 physically independent and apparently healthy individuals of either sex, with mean age of 66.61 ± 4.73 years. Active group obtained mean 14.32 ± 0.763 in whoqol’s scores for levels of quality of life, the Control group (CG) obtained mean 13.31 ± 0.94 and p-value 0.05. The ANOVA with repeated samples showed higher values for active group when compared with control group after intervention, the significant level was p < 0.05. It must be recognized that not every aspect of human life is reduced to the practice of physical activity; however, it is an important instrument that generates well-being in this age group.
1. INTRODUCTION
The concept of quality of life (QoL) is very broad and dynamic. One can find diverse definitions for this term in the literature, but all of them take cultural, social and environmental individuality into consideration. According to the World Health Organization, it is the perception of the individuals’ position in life, expectations, standards and concerns [1,2].
It is conceptualized as a generic, multidimensional parameter, describing an individual’s subjective perception of his/her physical and psychological health, as well as his/her social functioning and environmental and general life status. It’s measurements have typically included a series of life domains: physical, emotional, social, environmental, and material [3]. Those who evaluate their QoL synthesize their experiences and perceptions.
Emotional maturity will also favor social relationships, beyond the mere satisfaction of conviviality, encouraging volunteer actions and demonstrating that besides serving one’s own well-being, one must serve the community as well. Feelings other than sexual satisfaction must be shared with one’s partner, including exchanges of affection and friendship [4].
Several studies have been developed to examine the importance of health quality in old age. Many of them have emphasized the importance of physical activity or mobility as a way of improving organic conditions and slowing physical degeneration [5].
Evidences show the beneficial effect of an active lifestyle [6], mainly if physical and functional autonomy can be maintained throughout aging: that minimizes degeneration improving health and QoL. The concept of QoL is quite complex including a variety of aspects [7,8].
The reduced physiological capacity evident with ageing may affect the ability to perform many tasks, potentially affecting quality of life. Previous research has clearly demonstrated the reduced capacity of the respiratory system with ageing and described the effect that habitual physical activity has upon this decline [9].
It has been shown that physical activity produces increased range of motion, strength muscle and functional autonomy levels [10,11].
The physiological process of aging is marked by a decrease in motor skills, reduced strength, flexibility, speed and VO2max, hindering daily activities and maintenance of a healthy lifestyle [12,13].
The aim of this study is to compare the levels of quality of life in old adults sedentary and practitioners of physical activity.
2. MATERIALS AND METHODS
The sample consisted of 159 physically independent and apparently healthy individuals of either sex, with mean age of 66.61 ± 4.73 years, body mass index was calculated from weight and height measurements was 27.23 ± 3.46 [1,14]. All participants were retired, only ten were male and five participants return to work. The times on schooling were mean eleven years. There was only one subject who didn’t knew read or write.
Priority was given to group that participated in physiccal activity programs. The subjects were randomly distributed by simple raffle into two groups. The group that participated in physical activity programs had 125 subjects, practicing resistive training for 16 weeks. These groups were denominated active group [2,15]. The second group who called control group (CG with 34 subjects).
The criterion were, the participants had to be 60 years of age or greater and be capable of performing physical activity. Those with osteoarticular alterations, cardiopathy, vascular diseases, diabetes, arterial hypertension all this diseases without medical control and any alteration that prevented practice of physical exercises were assigned to control group.
All participants signed an informed consent form corresponding research in human beings [14]. All procedures were according to the Helsink declaration of 1975 and were approved by the institutional Ethic Committee under number 24/2011;
For the physical evaluation, the participants were asked to wear bathing suits (swimsuit and trunks) to obtain body measurements such as height and body mass index (BMI). To evaluate body mass, a certified (precision of 100 g) Filizola scale was used. Height was measured using an INMETRO certified stadiometer (precision of 1 mm) [3,15].
The groups responded to WHOQOL-100 [1] questionnaires were for the most part self-administered; however the researchers assisted some individuals with low visual acuity or low levels of scholarity.
For statistical procedures were used Predictive Analytics Software (PASW) Statistics 18 for Windows and mean, standard deviation. To verify sample normality and homogeneity were used Shapir-Wilk and Levene test. The ANOVA with repeated measures on group factors (ST, DFL and CG) and time (pre e pos-test) to compare inner and inter groups, followed by post hoc of Tukey to identify differences. The study assumed level p < 0.05 for statistical significance.
3. RESULTS
The characteristics of the sample showed (Table 1) that active group had many systemic diseases, bmi was 27.45 ± 4.40 who signalized over weight, there was a participant who return work and women compound major of participants (99 women and 26 men).
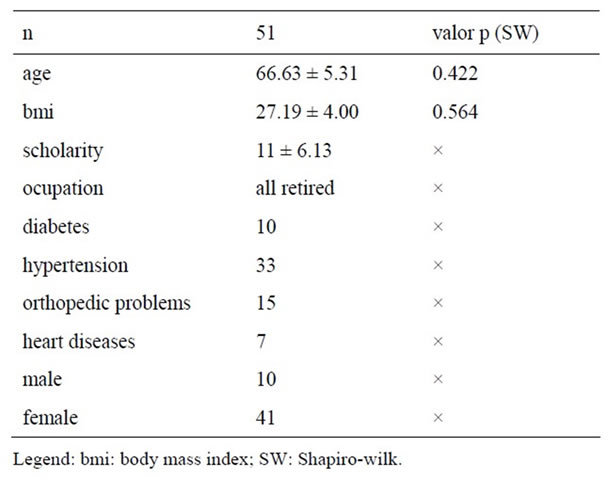
Table 1. Sample caracteristics.
On Figure 1 the results will be showed separated by domains. After 16 week the control group (CG) gets the levels of quality of life softly better but not with signifycative difference (p < 0.05). On domain 1 had mean diminish. When observed overall column the standard deviation get smaller.
The results obtained by active group were better after 16 weeks on QOL levels, showing that practice of physical activity promoted modifications on perceptions with life. This corroborate with Huang’s (2006) studies when he says that WHOQOL instruments measure a broad range of perception with life.
When analyzing the domains separately, it can be observed that, although the group was active, apparently healthy and obtained the general level of satisfaction for quality of life, Dom1 (which verifies pain and discomfort, energy and fatigue, sleep and rest) reach level significative higher (p < 0.05) after intervention and when it compared with control group difference was significative positive (p < 0.000) for active group [2].
Similar results were found for Dom 2 (psychology) when it compared with control group (CG) after intervention, the difference was significative positive (p < 0.000) for AG, it capacities for relief depression and reinforce mental activities.
The same occurred with Dom 3 (0.04) (related to mobility, activities of daily living; dependence on medicinal substances and medical aids; and work capacity), when make inner comparisons (0.04) and when it made intra groups, the results where positive for AG (0.006).
The physical activity promotes relations among peoples, make those persons closer each other and Dom 4 (personal relationships, social support and sexual activity) results demonstrated, when it compared with CG, difference was significative positive, once more for AG (0.07).
To observe spirituality, Dom 6 yielded results above 16.95, demonstrating a high level of belief in religious

* = p < 0.05 Active group pré × pos test; # = p < 0.05 Active pos × Control pós test.
Figure 1. Results pos test: active group × control group.
practices, all participants on both group integrates church activities.
And finally the QoL index, called overall, show AG significative advantage when it reached values on intra groups comparisons (p = 0.012) that demonstrated physical interventions promotes subjective perceptions on QoL.
Simultaneous measurements of self-reported and objective measures of physical functioning should add a more integrated view for evaluation of therapeutic effectiveness, since the overall correlation was poor between objective and subjective scores among individuals [15]
4. DISCUSSION
This study score provides scores on QoL measured by the WHOQOL—100 on sample of the population who participated on county program on inner city of Rio de Janeiro state [3].
In a study performed by Samano et al. [16], a multivariate analysis showed that prayer and belief in alternative/complementary medicines significantly correlated with a better quality of life on functional and symptom scales. These results corroborate with this study because the members of active group were actively participants of many churches and the levels of dominium who refers spirituality get higher on pos test.
A study promoted by Aberg et al. [17], to improve to understanding of factors is perceived by elderly people as important for their life satisfaction, during and after rehabilitation. Three themes emerged as important for life satisfaction activity, independence and adaptation. Activity and independence were considered significant better for life satisfaction on active group. These findings reinforce the results of other studies showing that actives elderly had higher mobility and physical independence [4,5].
On study made by Figueira et al. [18] who compared quality of life among Brazilians and Indians elderly, they conclude that knowing the concepts of the researched population and searching for the perception of their needing it is possible to develop strategies to know how the old aged perceive their aging. The proper concerning of asking the old aged what they consider important on determining their quality of life makes it possible to help them produce themselves, in this new phase of their lives as old aged, to transcend their aging dilemmas. As our group, the level of relationship discretely higher showing that social activities are important to see another experiences and learn with other.
To reinforce the impact of physical exercise on the quality of life was concluded with the studies carried out by Kuan et al. [19], where he investigated the relation of quality of life levels in institutionalized elderly patients (in this study a reduce format was used—WHOQOL BREF). It was possible to verify that physical activity had a strong impact on the physical health domain and consequently on the quality of life levels of this group. This result demonstrated that immobility were important component to interfere on happiness, some relates of members of active group were on direction that physical activities became their lives more happy and arranged to daily activities.
When the instrument WHOQOL was compared with other instruments, researchers and clinicians should carefully define their research questions related to patient-reported outcomes before selecting which instrument to use [20].
Hagell and Westergren [21] deemed necessary to consider, ratings of perceived importance of various areas of life are probably best used separately from satisfaction ratings. The level of education and understood of questions may be a bias to study, this were perceived on subjects with low schooling.
On randomized controlled trial investigated the effects of upperand lower-limb aerobic exercise training on disease-specific functional status and generic health-related quality of life (QOL) in patients with intermittent claudicating using another instrument the Medical Outcomes Study Short Form version 2 (SF-36v2) and European Quality of Life Visual Analog Scale (EQ-VAS) for health-related QOL observed after 24 to 72 weeks of follow-up, more consistent changes in generic healthrelated QOL domains were apparent in the lower-limb. Those find agree with results of this study on getting best results on physical domain. Although in our study the active group reach best result in 12 to 16 weeks [22].
Another study used adapted Tai chi program to verify the effects of targeted exercise programs on health-related quality of life compared with usual care based on the ability to perform activities of daily living (ADL) and the Neuropsychiatric Inventory scores in geriatric institutionalized persons with 65 years old above after 12 month. The components of Activity Daily Living, eg, ability to walk, continence, and nutrition, were maintained better in the intervention groups than in the control group and conclude that adapted exercise programs can slow down the decline in health-related quality of life among heterogeneous, institutionalized elderly persons [23-28]. To be active with anything is important for elderly, in this study the members of AG made domestic activities besides exercises programs.
The subject of AG were oriented by physician to look for physical activities to get health and better levels of QoL in order to get systemic parameters better. It was observed in the study was to evaluate the impact of complex ambulatory education on quality of life, exercise capacity and B-type natriuretic peptide (BNP) level in chronic stable heart failure patients. The data were evaluated before and 2 months after the patient education: quality of life (evaluated by the Minnesota questionnaire), peak exercise oxygen consumption (VO2) and BNP level. He concluded that patient education with the emphasis on adherence, self-care management and physical training has a reliable positive impact on the quality of life, exercise capacity and plasma levels of B-type natriuretic peptide in the population of stable moderate HF patients [29].
These results suggest that, although the participants reported improvements in the physical health domain, the instrument used to check quality of life levels was not able to identify or perceive the benefits derived by the activities proposed for the active elderly. It can also be observed that the programs did not result in any perception change among the elderly, lead to the adoption of healthy habits or identify barriers that impeded the adoption of these new habits.
5. CONCLUSIONS
Physical quality gains in fitness are related to improved quality of life, autonomy and independence, enabling the elderly to engage in daily living and work activities. The results obtained by the group studied did not attain the minimum quality of life satisfaction levels when assessed separately, suggesting that the instrument did not succeed in verifying these qualities.
The aspects of quality of life is composed by different subjects and can observed separated, on the other hand, it is known that quality of life levels are influenced by overall environment. It must be recognized that not every aspect of human life is reduced to the practice of physiccal activity; however, it is an important instrument that generates functional autonomy and well-being in this age group.
These concepts of quality of life are reported in individuals exhibiting satisfactory levels of independence or functional autonomy. It is hoped that human beings can be independent in their daily activities and autonomous in their decisions, thus living longer and happier lives.
![]()
![]()
REFERENCES
- WHOQOL Group (1998) The World Health Organization Quality of Life Assesment (WHOQOL): Development and general psychometric properties. Social Science & Medicine, 46, 1569-1585. doi:10.1016/S0277-9536(98)00009-4
- Figueira, H.A., Figueira, O.A., Figueira, A.A., et al. (2010) Elderly quality of life impacted by traditional Chinese medicine techniques. Clinical Interventions in Aging, 5, 301-305. doi:10.2147/CIA.S10615
- Dykstra P. (2009) Older adult loneliness: Myths and realities. European Journal of Ageing, 6, 91-100. doi:10.1007/s10433-009-0110-3
- Fleck, M.P.A., Chachamovisch, E. and Trentini, C.M. (2003) Projeto WHOQOL-OLD: Método e resultados de grupos focais no Brasil. Revista de Saúde Pública, 37, 793-799. doi:10.1590/S0034-89102003000600016
- Siqueira Rodrigues, B.G., Cader, S.A., et al. (2010) Pilates method in personal autonomy, static balance and quality of life of elderly females. Journal of Bodywork and Movement Therapies, 14, 195-202. doi:10.1016/j.jbmt.2009.12.005
- Freitas, C.M.S.M., Santiago, M.S., Viana, A.T., Leao, A.C. and Freyre, C. (2007) Aspectos motivacionais que influenciam a adesao e manutencao de idosos a programas de exercıcios fısicos. Revista Brasileira de Cineantropometria & Desempenho Humano, 9, 92-100 (in Portuguese).
- Figueira, H., Figueira, J., Mello, D. and Dantas, E. (2008) Quality of life throughout aging. Acta Medica Lituanica, 15, 169-172.
- Fraga, M.J., Cader, S.A., Ferreira, M.A., Giani, T.S. and Dantas, E.H.M. (2011) Aerobic resistance, functional autonomy and quality of life (QoL) of elderly women impacted by a recreation and walking program. Archives of Gerontology and Geriatrics, 52, e40-e43. doi:10.1016/j.archger.2010.04.021
- Watsford, M.L., Murphy, A.J. and Pine, M.J. (2007) The effects of ageing on respiratory muscle function and performance in older adults. Journal of Science and Medicine in Sport, 10, 36-44. doi:10.1016/j.jsams.2006.05.002
- Vale, R.G.S., Oliveira, R.D., Pernambuco, C.S., Meneses, Y.P.S.F., Novaes, J.S. and Andrade, A.F.D. (2009) Effects of muscle strength and aerobic training on basal serum levels of IGF-1 and cortisol in elderly women. Archives of Gerontology and Geriatrics, 49, 343-347. doi:10.1016/j.archger.2008.11.011
- Tainaka, K., Takizawa, T., Katamoto, S. and Aoki, J. (2009) Six-year prospective study of physical fitness and incidence of disability among community-dwelling Japanese elderly women. Geriatrics & Gerontology International, 9, 21-28. doi:10.1111/j.1447-0594.2008.00492.x
- Souza Santos, C.A., Cader, S.A., Dantas, E.H.M. and Moreira, M.H.R. (2010) Physical fitness of post-menopausal women submitted to a physical activities programme. Biomedical Human Kinetics, 2, 93-96. doi:10.2478/v10101-010-0023-9
- ACSM, American College of Sports Medicine (1998) Position stand. Exercise and physical activity for older adults. Medicine & Science in Sports & Exercise, 30, 992-1008. doi:10.1097/00005768-199806000-00033
- BRASIL. Ministério da Saúde (1996) Resolução 196/96. O Plenário do Conselho Nacional de Saúde resolve aprovar diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. Em 10 de outubro de.
- Lindholm, E., Brevinge, H., Bergh, C.-H., Körner, U. and Lundholm, K. (2003) Relationships between self-reported health related quality of life and measures of standardized exercise capacity and metabolic efficiency in a middle-aged and aged healthy population. Quality of Life Research, 12, 575-582. doi:10.1023/A:1025034919526
- Samano, E.S.T., Goldenstein, P.T., et al. (2004) Rezar se correlaciona com uma melhor qualidade de vida: Resultados de um estudo sobre o uso de medicina alternativa/complementar por um grupo de pacientes oncológicos brasileiros. Sao Paulo Medicine Journal, 122.
- Aberg, A.C., Sidenvall, B., Hepworth, M., O’Reilly, K. and Lithell, H. (2005) On loss of activity and independence, adaptation improves life satisfaction in old age—A qualitative study of patients perceptions. Quality of Life Research, 14, 1111-1125.
- Fleck, M.P.A., Leal, O.F., Louzada, S., Xavier, M., Chachamovich, E., et al. (1999) Desenvolvimento da versão em português do instrumento de avaliação de qualidade de vida da OMS (WHOQOL-100). Revista Brasileira de Psiquiatria, 1, 536-542.
- Figueira, H.A., Figueira, J.A., Bezerra, J.C., Dantas, E.H.M. (2009) Old aged quality of life: Brazil-India a cross-cultural perspective. Indian Journal of Gerontology, 23, 66-78.
- Kuan-Lang, L., Rong-Jye, T., Bing-Long, W. Hong-Shen, L., Amidon, R.L. and Senyeong, K. (2005) Health-related quality of life and health utility for the institutional elderly in Taiwan. Quality of Life Research, 14, 1169-1180. doi:10.1007/s11136-004-3061-3
- Huang, I-C., Wu, A.W. and Frangakis, C. (2006) Do the SF-36 and WHOQOL-BREF measure the same constructs? Evidence from the Taiwan population. Quality of Life Research, 15, 15-24. doi:10.1007/s11136-005-8486-9
- Hagell, P. and Westergren, A. (2006) The significance of importance: An evaluation of Ferrans and powers’ quality of life index. Quality of Life Research, 15, 867-876. doi:10.1007/s11136-005-5467-y
- Saxton, J.M., Zwierska, I., et al. (2011) Upper-versus lower-limb aerobic exercise training on health-related quality of life in patients with symptomatic peripheral arterial disease. Journal of Vascular Surgery, 53, 1265- 1273.
- Hopman, W.M., Berger, C., et al. (2007) The association between body mass index and health-related quality of life: data from CaMos, a stratified population study. Quality of Life Research, 16, 1595-1603. doi:10.1007/s11136-007-9273-6
- Magarelli, P.C., Cridennda, D.K. and Cohen, M. (2009) Changes in serum cortisol and prolactin associated with acupuncture during controlled ovarian hyperstimulation in women undergoing in vitro fertilization-embryo transfer treatment. Fertility and Sterility, 92, 1870-1879. doi:10.1016/j.fertnstert.2008.10.067
- Cruz, L.N., Polanczyk, C.A., Camey, S.A., Hoffmann, J.F. and Fleck, M.P. (2011) Quality of life in Brazil: Normative values for the Whoqol-bref in a southern general population sample. Quality of Life Research, 20, 1123- 1129.
- Beuttenmüller, L., Cader, S.A., Macena, R.H.M., Araujo, N.S., Nunes, É.F.C. and Dantas, E.H.M. (2010) Muscle contraction of the pelvic floor and quality of life of women with stress urinary incontinence who underwent kinesitherapy. Physiotherapy, 18, 35-41. doi:10.2478/v10109-010-0052-5
- Daniel, F., Vale, R., Giani, T., Bacellar, S. and Dantas, E. (2010) Effects of a physical activity program on static balance and functional autonomy in elderly women. Macedonian Journal of Medical Sciences, 3, 21-26. doi:10.3889/MJMS.1857-5773.2010.0083
- Marfell-Jones, M., Olds, T., Stewart, A. and Carter, L. (2006) International standards for anthropometric assessment. ISAK, Potchefstroom.