Pharmacology & Pharmacy
Vol.05 No.11(2014), Article ID:50980,6 pages
10.4236/pp.2014.511116
Novel Therapeutic Options for the Treatment of Nonvalvular Atrial Fibrillation
Rupal Patel Mansukhani1,2, Lucio R. Volino1,3
1Department of Pharmacy Practice and Administration, Ernest Mario School of Pharmacy, Rutgers, The State University of New Jersey, Piscataway, USA
2Morristown Medical Center, Morristown, USA
3The Great Atlantic and Pacific Tea Company, Kenilworth, USA
Email: rupie@rci.rutgers.edu
Copyright © 2014 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 22 August 2014; revised 21 September 2014; accepted 18 October 2014
ABSTRACT
Objective: To review the literature for the emerging oral anticoagulants, dabigatran, rivaroxaban, and apixaban currently available in the United States. Data Source: A literature review was performed in MEDLINE (1947?July 2014) using the keywords atrial fibrillation AND dabigatran OR rivaroxaban OR apixaban. The references identified from the literature review were then evaluated. All of the literature retrieved from MEDLINE that was published as an original clinical trial was included in this review. Other pertinent articles published related to the original clinical trials were also considered. The references included in this review were limited to studies conducted in humans and written in the English language. Conclusion: The new oral anticoagulant agents have demonstrated benefit over warfarin. The pharmacologic profiles of the newer agents are predictable, with rapid onsets of action. The newer agents are also more convenient for patients since they do not require regular INR monitoring. Although there are many advantages to the newer agents, a patient evaluation must be considered prior to initiating them.
Keywords:
Atrial Fibrillation, Dabigatran, Rivaroxaban, Apixiaban

1. Introduction
Atrial Fibrillation (AF) is the most common type of arrhythmia and affects between 2.7 and 6.1 million American adults annually. Atrial fibrillation can increase the risk of stroke and impair cardiac function, possibly leading to a myocardial infarction (MI). Symptoms of AF include fatigue, palpitations, dyspnea, hypotension, or syncope [1] .
Atrial fibrillation produces changes in atrial function and structure. Electrical remodeling takes place within the first few days of AF. After cardioversion, the heart can lead to reduced atrial transport function, increasing the chance of a thrombus formation. This also results in a reduction of atrial contractility, which can lead to the persistence of AF. Atrial enlargement occurs after chronic repeated remodeling. The longer the heart remains in AF, the more difficult it becomes to restore normal sinus rhythm [2] .
Based on symptoms, patients can fall into one of four categories [1] :
1) Paroxysmal AF―AF terminates spontaneously or with intervention within 7 days of onset.
2) Persistent AF―continuous AF that is sustained greater than 7 days.
3) Longstanding persistent AF―continuous AF for greater than 12 months duration.
4) Nonvalvular AF―AF in the absence of rheumatic mitral stenosis, a mechanical or bioprosthetic heart valve, or mitral valve repair.
A few reasons that potentially could be reversed include “binge drinking, cardiothoracic andnoncardiac surgery, myocardial infarction (MI), pericarditis, myocarditis, hyperthyroidism, electrocution, pneumonia, and pulmonary embolism” [1] . Initial evaluation of AF should include chest radiography, complete metabolic and blood count, echocardiogram, electrocardiogram, and any other pertinent labs. Atrial fibrillation patients typically show irregular R-R intervals, absence of distinct repeating P waves, and irregular atrial activity in an electrocardiogram. Patients should be evaluated to rule out other comorbidities that may cause similar symptoms such as pneumonia, vascular congestions, hyperthyroidism, or any other disease state [3] .
The outcomes of therapy depend on the number of AF episodes. The initial goal is to determine cardiac stability and provide emergency stabilization. Long term management includes rhythm or rate control. Rate control is recommended for most patients because data shows patients assigned to rhythm control have more hospitalizations. When rate control fails or patient remains symptomatic, rhythm control should be considered. Stroke prevention should be considered in both groups with anticoagulation therapy [3] .
With the addition of newer agents to the market, anticoagulation therapy has expanded to include many different treatment options. Warfarin has been the gold standard to prevent thromboembolic stroke in patients with atrial fibrillation. It is indicated for prophylaxis and treatment of venous thrombosis and pulmonary embolism; prophylaxis and treatment of thromboembolic complications associated with AF and/or cardiac valve replacement, and reduction in the risk of death, recurrent myocardial infarction, and thromboembolic events such as stroke or systemic embolization after myocardial infarction. It works by inhibiting vitamin K dependent coagulation factors (II, VII, IX, X, and proteins C and S). Warfarin has been shown to be superior to antiplatelet medications like aspirin and clopidogrel, however it has many limitations. Warfarin has a narrow therapeutic window in patients with AF and patients must be monitored for their prothrombin time (PT). The PT is reported as an international normalized ratio (INR). INR monitoring should be done on AF patients frequently to achieve a goal of 2.0 - 3.0. Warfarin also has multiple food, drug, and disease state interactions, which can cause unpredictable dose responses [4] .
The US Food and Drug Administration (FDA) have, recently approved three novel oral anticoagulants, dabigatran, apixaban, and rivaroxaban, for AF. These newer agents provide some advantages over warfarin such as predictable profiles, faster onset of action, less drug-drug interactions, less monitoring, and reductions in stroke and systemic embolisms compared to warfarin. However, they come at a higher medication cost, greater risk for thrombotic events with premature discontinuation, and an increased risk of bleeding since their pharmacological action cannot be reversed. Additionally, patients with chronic renal disease may be at an increased risk of bleeding and may not benefit from the newer agents [4] - [7] . Basic characteristics of the oral anticoagulants used for atrial fibrillation are included in Table 1.
2. Dabigatran
Dabigatran (Pradaxa®) is an oral direct thrombin inhibitor approved to reduce the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation and to reduce the risk of deep venous thrombosis (DVT) and pulmonary embolism (PE) recurrence in patients who have been previously treated. Dabigatran is also approved for the treatment of DVT and PE in patients who have been treated with a parenteral anticoagulant for 5 - 10 days [6] . Its safety and efficacy were evaluated in the trial, A Randomized Evaluation of Long-term Anticoagulant Therapy, Warfarin, compared with Dabigatran (RE-LY).

Table 1. New oral anticoagulant medications.
CrCl = creatinine clearance; SCr = serum creatinine.
The RE-LY trial randomized 18,113 patients to dabigatran 110 mg, dabigatran 150 mg, and open labeled dose adjusted warfarin to target an INR of 2.0 - 3.0.
The baseline characteristics included patients with atrial fibrillation with average age 72 years, mean CHADS2 score of 2.1, and history of stroke (20%), myocardial infarction (16.6%), and heart failure (32%). Half of the patients had received long-term therapy with warfarin. Dabigatran 150 mg was superior to warfarin in the prevention of stroke or systemic embolism (dabigatran 1.11% per year vs. warfarin 1.69% per year; RR = 0.66; 95% CI = 0.53 - 0.82; P < 0.001 superiority and P < 0.001 noninferiority). The 110 mg dabigatran dose was noninferior to warfarin (P < 0.001) but not superior (P = 0.34). The risk of death from any cause was lower in the dabigatran 150 mg group vs. warfarin (3.64% per year vs. 4.13% per year; RR = 0.88; 95% CI = 0.77 - 1.00; P = 0.051) and the risk of MI was greater in the dabigatran 150 mg group (0.74% per year vs. 0.53% per year; relative risk = 1.38, 95% CI = 1.00 - 1.91; P = 0.048). The risk of major bleeding, when comparing dabigatran 150 mg vs. warfarin, was not significantly different (3.11% per year vs. 3.36% per year; relative risk = 0.93; 95% CI = 0.81 - 1.07; P = 0.31). The risk of gastrointestinal bleeding (1.51% per year vs. 1.02% per year; relative risk = 1.50; 95% CI = 1.19 - 1.89; P < 0.001) and intracranial bleeding (0.30% per year vs. 0.74% per year; relative risk = 0.40; 95% CI = 0.27 - 0.60; P < 0.001) was higher in the dabigatran 150 mg group vs. warfarin [8] .
A long-term, multicenter, observational study of dabigatran treatment in patients with atrial fibrillation (RELY-ABLE) followed 5851 patients on dabigatran for 28 months after completion of the RE-LY trial. Patient baseline characteristics were similar to those participating in RE-LY however patients in RELY-ABLE were less likely to have heart failure (27.5% vs. 36.5%). RELY-ABLE examined long-term effects of dabigatran 110 mg and 150 mg. The results showed dabigatran 150 mg continued to prevent stroke or systemic embolism (dabigatran 150 mg 1.15% per year and dabigatran 110 mg 1.24% per year; Hazards Ratio (HR) = 0.92; 95% CI = 0.67 - 1.27). Rates of myocardial infarction in dabigatran 150 mg and 110 were also low at 0.69% and 0.72% per year. (HR = 0.96; 95% CI = 0.63 - 1.45). Death rates were lower compared to RE-LY at 3.02% and 3.10% per year (HR = 0.97; 95% CI = 0.80 - 1.19). Long term rates of major bleeding were 3.74% and 2.99% per year (HR = 1.26; 95% CI = 1.04 - 1.53). Rates in dabigatran 150 mg and 110 mg for gastrointestinal (1.54% and 1.56% per year; HR = 0.99; 95% CI = 0.75 - 1.31) and intracranial (0.33% and 0.25% per year; HR, 1.31; 95% CI 0.68 - 2.51) bleeding were similar. The long-term data on incidences of stroke as well as intracranial bleeding show dabigatran can help protect patients with atrial fibrillation [9] .
3. Rivaroxaban
Rivaroxaban is a factor Xa inhibitor anticoagulant approved for the reduction of stroke and systemic embolism risk in patients with nonvalvular atrial fibrillation. In addition, it is indicated to treat and reduce the risk of recurrence of DVT and PE and prevent DVT which may lead to PE in patients undergoing knee or hip replacement surgery [7] . One pivotal trial evaluated rivaroxaban’s use for stroke and systemic embolism prevention in atrial fibrillation patients: rivaroxaban―Once Daily, Oral, Direct Factor Xa inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKET AF).
ROCKET AF was a randomized, double-blinded, double-dummy, event-driven, noninferiority trial evaluating the prevention of stroke (ischemic or hemorrhagic) and systemic embolism in 14,264 nonvalvular atrial fibrillation patients with moderate-to-high risk for stroke. The baseline characteristics included atrial fibrillation patients with average age 73 years, mean CHADS2 score of 3.47, and history of stroke, systemic embolism, or TIA (54.8%) and heart failure (62.5%). Significantly less patients in the rivaroxaban group (16.6%) experienced previous myocardial infarctions compared to patients on warfarin (18.0%) P < 0.05. Approximately 62% of patients used a vitamin K antagonist (VKA) and 37% used aspirin prior. Patients received rivaroxaban (20 mg once a day or 15 mg once day for those with CrCl of 30 - 49 mL/min) or warfarin adjusted to an INR of 2.0 - 3.0 [10] [11] . Considering the combined data collected from the treatment and follow-up periods, rivaroxaban was noninferior to warfarin at reducing stroke and systemic embolism (rivaroxaban 2.1% per year vs. warfarin 2.4% per year; HR = 0.88; 95% CI = 0.74 - 1.03; P < 0.001 for noninferiority and P = 0.12 for superiority). During treatment, rivaroxaban reduced the risk of stroke and systemic embolism (rivaroxaban 1.7% per year vs. warfarin 2.2% per year; HR = 0.79; 95% CI = 0.66 - 0.96; P = 0.02) but follow-up on patients who discontinued either therapy (median 117 days of follow-up after discontinuation) showed no difference in prevention of primary events (rivaroxaban 4.7% per year vs. warfarin 4.3% per year; HR = 1.10; 95% CI = 0.79 - 1.52; P = 0.58). There were no significant differences between groups for the intent-to-treat analysis in all cause rates of death (P = 0.15). Bleeding risk assessments combined major and clinically relevant nonmajor bleeds which were not significantly different between rivaroxaban and warfarin (rivaroxaban 14.9% per year vs. warfarin 14.5% per year; HR = 1.03; 95% CI = 0.96 - 1.11; P = 0.44). Although the overall major bleeding (rivaroxaban 3.6% per year v. warfarin 3.4% per year; HR = 1.04; 95% CI = 0.90 - 1.20; P = 0.58) and myocardial infarction rates (rivaroxaban 0.9% per year vs. warfarin 1.1% per year; HR = 0.81; 95% CI = 0.63 - 1.06; P = 0.12) were comparable between groups, major gastrointestinal bleeds were more common in patients on rivaroxaban (3.2%) compared to warfarin (2.2%) P < 0.001. Intrancranial hemorrhage rates were also found to be significantly lower in the rivaroxaban group (rivaroxaban 0.5% per year vs. warfarin 0.7% per year; HR = 0.67; 95% CI = 0.47 - 0.93; P = 0.02) [11] .
4. Apixaban
Similar to rivaroxaban, apixaban is a factor Xa inhibitor anticoagulant approved for the reduction of stroke and systemic embolism risk in patients with nonvalvular atrial fibrillation [5] . Two pivotal studies evaluated efficacy and safety in atrial fibrillation patients at risk for stroke: Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) and Apixaban Versus Acetylsalicylic Acid to Prevent Stroke in Atrial Fibrillation Patients Who Have Failed or Are Unsuitable for Vitamin K Antagonist Treatment (AVERROES).
ARISTOTLE, a randomized, double-blinded trial was a noninferiority assessment of apixaban compared to warfarin for the reduction of stroke (ischemic or hemorrhagic) and systemic embolism in 18,201 atrial fibrillation patients with at least one additional risk factor for stroke [12] [13] . The baseline characteristics included atrial fibrillation patients with average age 70 years, mean CHADS2 score of 2.1, and history of stroke, TIA or systemic embolism (19.5%), myocardial infarction (14.7%), and heart failure or reduced left ventricular ejection fraction (35.5%). Patients received apixaban (5 mg twice a day or 2.5 mg twice a day for those with a minimum of two criteria including age ≥ 80 years, body weight ≤ 60 kg or serum creatine ≥ 1.5 mg/dL) or warfarin adjusted to an INR of 2.0 - 3.0. Apixaban was found to decrease stroke or systemic embolism risk (apixaban 1.27% per year vs. warfarin 1.60% per year; HR = 0.79; 95% CI = 0.66 - 0.95; P < 0.001 for noninferiority and P = 0.01 for superiority). Apixaban also demonstrated lower all cause death rates (3.52% per year vs. 3.94% per year; HR = 0.89; 95% CI = 0.80 - 0.998; P = 0.047) and major bleeding (2.13% per year vs. 3.09% per year; HR = 0.69; 95% CI = 0.60 - 0.80; P < 0.001), including intracranial bleeding (0.33% per year vs. 0.80% per year;
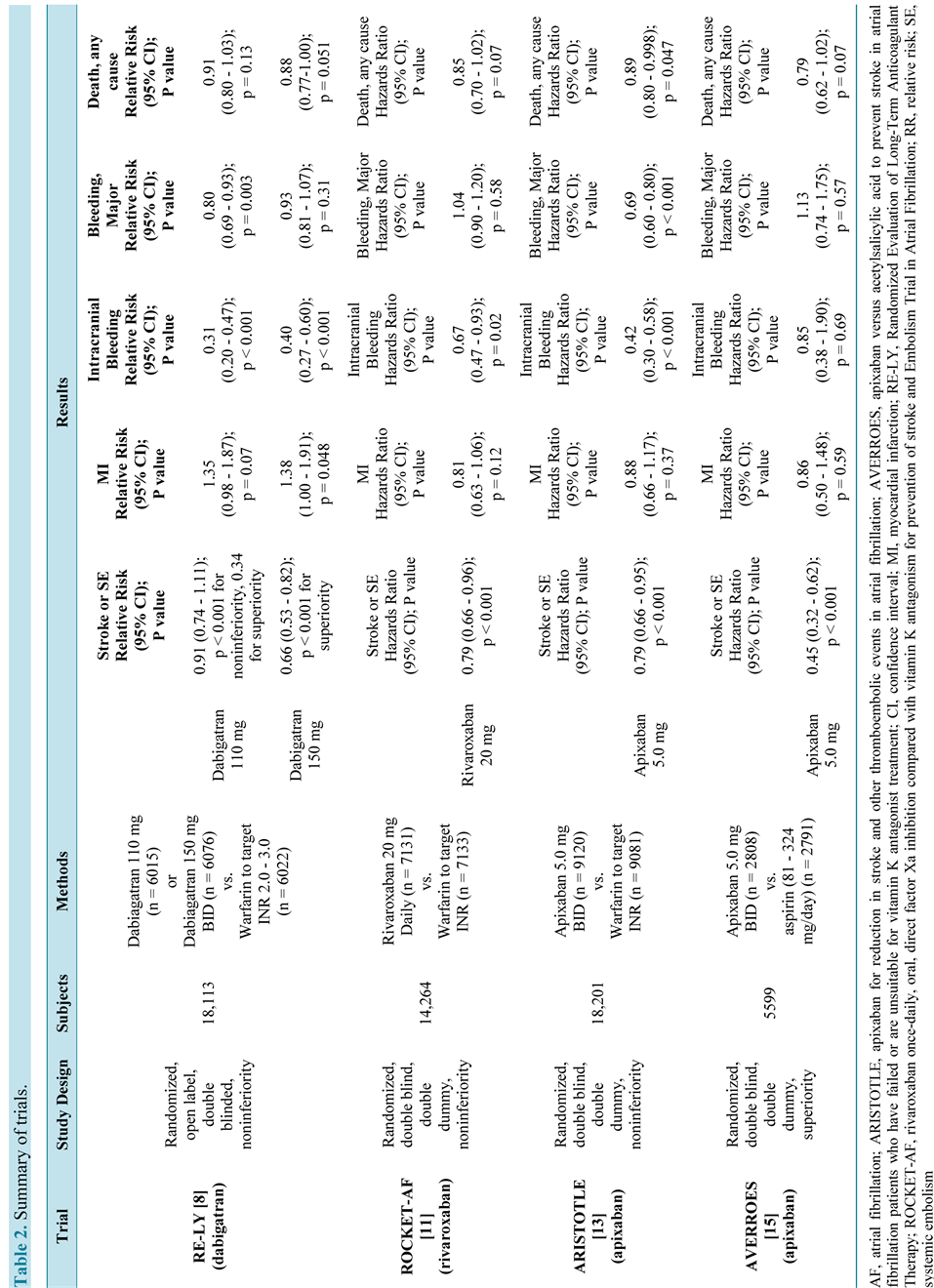
Table 2. Summary of trials.
HR = 0.42; 95% CI = 0.30 - 0.58; P < 0.001) compared to warfarin with comparable rates of myocardial infarction (0.53% per year vs. 0.61% per year; HR = 0.88; 95% CI = 0.66 - 1.17; P = 0.37) and gastrointestinal bleeding (0.76% per year vs. 0.86% per year; HR = 0.89; 95% CI = 0.70 - 1.15; P = 0.37). Both adverse events and serious adverse events were similar between apixaban (81.5% and 35.0%) and warfarin (83.1% and 36.5%), respectively [13] .
AVERROES was a double-blinded study evaluating stroke (ischemic or hemorrhagic) or systemic embolism incidence in 5599 atrial fibrillation patients with ≥1 stroke risk factor and who were not suitable for or failed VKA therapy [14] [15] . The baseline characteristics included atrial fibrillation patients with average age 70 years, mean CHADS2 score of 2.1, and history of stroke or TIA (13.5%), and heart failure (39%). Approximately 15% of patients used a VKA and 76% used aspirin within 30 days prior to screening. Patients received either apixaban (5 mg twice a day or 2.5 mg twice a day with the aforementioned criteria listed for ARISTOTLE) or aspirin 81 - 324 mg a day (based on investigator discretion). Compared to aspirin, apixaban significantly reduced the risk for stroke or systemic embolism (apixaban 1.6% per year vs. aspirin 3.7% per year; HR = 0.45; 95% CI = 0.32 - 0.62; P < 0.001) without affecting rate of death (apixaban 3.5% per year vs. aspirin 4.4% per year; HR = 0.79; 95% CI = 0.62 - 1.02; P = 0.07), myocardial infarctions (apixaban 0.8% per year vs. aspirin 0.9% per year; HR = 0.86; 95% CI = 0.50 - 1.48; P = 0.59), and major bleeding events (apixaban 1.4% per year vs. aspirin 1.2% per year; HR = 1.13; 95% CI = 0.74 - 1.75; P = 0.57), including gastrointestinal (apixaban 0.4% per year vs. aspirin 0.4% per year; HR = 0.86; 95% CI = 0.40 - 1.86; P = 0.71) and intracranial bleeding (apixaban 0.4% per year vs. aspirin 0.4% per year; HR = 0.85; 95% CI = 0.38 - 1.90; P = 0.69). Fewer patients on apixaban (22%) experienced serious adverse events compared to those on aspirin (27%) P < 0.001 [15] (Table 2).
5. Conclusions
Sixty years following the approval of warfarin by the FDA, dabigatran, rivaroxaban, and apixaban came to market. All three oral anticoagulant agents have demonstrated some benefit over warfarin. The pharmacologic profiles of the newer agents are predictable, with rapid onsets of action. This allows for patients to be protected sooner and eliminates the need to use parenteral anticoagulation agents for bridging therapy. The newer agents are also more convenient for patients since they do not require regular INR monitoring; are not affected by vitamin K rich foods; and have fewer drug-drug interactions. All three agents also showed reductions in the risk of stroke and systemic embolism with a lower risk of intracranial bleeding compared to warfarin [4] - [7] .
Although there are many advantages to the newer agents, a patient evaluation must be considered prior to initiating them. Factors such as medication cost and access should be taken into consideration. Monthly out of pocket medication expenses for patients without insurance are comparable for apixaban, dabigatran and rivaroxaban (~$350) but much higher than warfarin ($19.90―average cost based on a 5 mg daily dose from four major generic manufacturers) or aspirin ($0.45―average cost based on 81 mg or 325 mg daily dose from two generic manufacturers) [16] . Patients with prescription insurance plans may also experience higher costs from brand or tiered copayment structures and access or convenience issues related to potential prior authorization requirements since the newer anticoagulant agents are only available as brand name products. Another factor to consider when using the newer agents is medication adherence. Due to their short half-lives, stroke prevention decreases considerably upon discontinuation or periods of missed doses. This led to the FDA issuing a black box warning that premature discontinuation increases the risk of thrombotic events. Reversal agents are also not currently available; therefore, if bleeding or overdose occurs, patients should immediately discontinue the medication. Activated charcoal can be used to slow absorption but will not reverse the medication’s effect. Renal function should also be assessed for patients as all three agents need renal dosing adjustments. Patients with severe end stage chronic renal disease should use warfarin over the new oral anticoagulants. Dabigatran is dialyzable, but apixaban and rivaroxaban are not. The intricacy of managing patients on warfarin may have decreased with the newer agents, however patients still need to be monitored closely to ensure optimal patient outcomes [4] - [7] .
References
- January, C.T., Wann, L.S., Alpert, J.S., Calkins, H., Cleveland, J.C., Cigarroa, J.E., et al. (2014) 2014 AHA/ACC/HRS Guideline for the Management of Patients with Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Journal of the American College of Cardiology, 14, S0735-S1097.
- Allessie, M., Ausma, J. and Schotten, U. (2002) Electrical, Contractile and Structural Remodeling during Atrial Fibrillation. Cardiovascular Research, 54, 230-246. http://dx.doi.org/10.1016/S0008-6363(02)00258-4
- Guyatt, G.H., Akl, E.A., Crowther, M., Gutterman, D.D., Schuünemann, H.J., et al. (2012) Executive Summary: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest, 141, 7S-47S.
- Coumadin [Prescribing Information] (2011) Bristol-Myers Squibb Company, Princeton.
- Eliquis [Prescribing Information] (2014) Bristol-Myers Squibb Company, Princeton.
- Pradaxa [Prescribing Information] (2014) Boehringer Ingelheim Pharmaceuticals, Inc., Ridgefield.
- Xarelto [Prescribing Information] (2014) Janssen Pharmaceuticals, Inc., Titusville.
- Connolly, S.J., Ezekowitz, M.D., Yusuf, S., Eikelboom, J., Oldgren, J., Parekh, A., et al. (2009) Dabigatran versus Warfarin in Patients with Atrial Fibrillation. The New England Journal of Medicine, 361, 1139-1151. http://dx.doi.org/10.1056/NEJMoa0905561
- Connolly, S.J., Wallentin, L., Ezekowitz, M.D., Eikelboom, J., Oldgren, J., Reilly, P.A., et al. (2013) The Long-Term Multicenter Observational Study of Dabigatran Treatment in Patients with Atrial Fibrillation (RELY-ABLE) Study. Circulation, 128, 237-243. http://dx.doi.org/10.1161/CIRCULATIONAHA.112.001139
- Becker, R., Berkowitz, S.D., Breithardt, G., Califf, R.M., Fox, K. and Hacke, W. (2010) Rivaroxaban-Once Daily, Oral, Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation: Rationale and Design of the ROCKET AF Study. American Heart Journal, 159, 340-347.
- Patel, M.R., Mahaffey, K.W., Garg, J., Pan, G., Singer, D.E., Hacke, W., et al. (2011) Rivaroxaban versus Warfarin in Nonvalvular Atrial Fibrillation. The New England Journal of Medicine, 365, 883-891. http://dx.doi.org/10.1056/NEJMoa1009638
- Lopes, R.D., Alexander, J.H., Al-Khatib, S.M., Ansell, J., Diaz, R., Easton, J.D., et al. (2010) Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) Trial: Design and Rationale. American Heart Journal, 159, 331-339. http://dx.doi.org/10.1016/j.ahj.2009.07.035
- Granger, C.B., Alexander, J.H., McMurray, J.J., Lopes, R.D., Hylek, E.M., Hanna, M., et al. (2011) Apixaban versus Warfarin in Patients with Atrial Fibrillation. The New England Journal of Medicine, 365, 981-992. http://dx.doi.org/10.1056/NEJMoa1107039
- Eikelboom, J.W., O’Donnell, M., Yusuf, S., Diaz, R., Flaker, G., Hohnloser, S., et al. (2010) Rationale and Design of AVERROES: Apixaban versus Acetylsalicylic Acid to Prevent Stroke in Atrial Fibrillation Patients Who Have Failed or Are Unsuitable for Vitamin K Antagonist Treatment. American Heart Journal, 159, 348-353.e1. http://dx.doi.org/10.1016/j.ahj.2009.08.026
- Connolly, S.J., Eikelboom, J., Joyner, C., Diener, H.C., Hart, R., Golitsyn, S., et al. (2011) Apixaban in Patients with Atrial Fibrillation. The New England Journal of Medicine, 364, 806-817. http://dx.doi.org/10.1056/NEJMoa1007432
- Red Book Online [Database Online] (2014) Truven Health Analytics, Inc., Greenwood Village.