Surgical Science
Vol.4 No.1(2013), Article ID:27085,6 pages DOI:10.4236/ss.2013.41007
Quality Assurance in Wound Management in a Developing Country: How Satisfied Are Our Patients?
Reconstructive Plastic Surgery & Burns Unit, Komfo Anokye Teaching Hospital, School of Medical Sciences, Kwame Nkrumah University of Science & Technology, Kumasi, Ghana
Email: pimagben@yahoo.com
Received November 8, 2012; revised December 10, 2012; accepted December 18, 2012
Keywords: Quality Assurance; Patient Satisfaction; Wound Management; Health Resources
ABSTRACT
Background: Quality is important in every setting especially in the health service where the needs of patients should be an utmost priority. However, this is sometimes not the situation in most health care centres due to increasing stress because of inadequate resources and increasing demands for services. This present study seeks to assess quality assurance in the management of wounds. Method: A descriptive survey involving 280 participants; data was collected using structured questionnaire. The questionnaires included some quality indicators which were used to assess the quality of care patients received from the health facility. Results: Out of the 280 participants, females were 57.1% (n = 160) and males, 42.9% (n = 120). Ages of the participants ranged from 15 - 70+ years with a mean age of 35.8 ± 1.5; 28.6% (n = 80) of staff had an excellent attitude while 5.7% (n = 16) had a fair attitude. The condition of 112 did not require surgery (40.0%), however, out of the 168 who underwent surgery, 32 (19.0%) were not satisfied while 136 (81.0%) were satisfied. Also, 97.1% (n = 272) were accorded privacy, 51.4% (n = 144) were assured of confidentiality, 48.6% (n = 136) were educated on diagnoses and treatment, 91.4% (n = 256) understood pharmacy instruction, 57.1% (n = 160) were satisfied with time spent in the facility, 97.1% (n = 272) were not shun by nurses because of their wounds. Conclusion: Patient satisfaction should be the priority of all persons working in the health facility. In accessing quality service, patient satisfaction can be met if quality assurance measures are put in place. This quality assurance measures should include all units of the health delivery system since it would help to ensure judicious use of resources in order to meet the health needs of patients.
1. Introduction
Quality Assurance (QA) is a process-centered approach to ensuring that an institution or organization is providing the best possible products or services. Among the parts of the process that are considered in QA are planning, design, development, production and service. Quality assurance comprises a variety of approaches which are integrated to meet particular needs based on situation. Quality assurance has evolved as an internationally important aspect in the provision of health care services [1].
Quality assurance should ensure that medical activities are systematic and controlled. Patient satisfaction in delivery of quality healthcare is essential. When people go to seek medical care, their main aim is that they are given the needed attention and care in order to relieve them of their pain so that they feel better. However, sometimes they are refused these and more. According to Offei et al., (2004) quality of care implies healthcare activities that the medical, nursing, laboratory fields etc. perform daily to benefit patients without causing harm to them [2].
Quality of care demands that attention is paid to the needs of patients and clients. Also methods that have been tested to be safe, affordable and can reduce deaths, illness and disability have to be used. Furthermore, healthcare delivery personnel are expected to practice according to set standards as lay down by clinical guidelines and protocols. To improve upon quality, there should be supervision and regular monitoring. Quality assurance programs for health care are paramount to the realization of good quality health care because of their ability to identify gaps in service provision. The reasons for the poor quality of healthcare services may be few resources, shortage of staff, poor interpersonal relationship between healthcare providers and patients, difficulty in accessibility of health facilities to patients, inefficiency of health services, and technical incompetence of some healthcare providers among others.
Good management of wound and ulcers aids in the healing process and also important because of the impact on the quality of life of the individual and the society at large [3,4]. This study seeks to assess quality assurance in the management of wounds and ulcers.
2. Methods
2.1. Study Setting
This survey was undertaken at Global Evangelical Mission Hospital, located at Apromase, in the Ejisu-Juaben Municipality of the Ashanti Region of Ghana, West Africa.
2.2. Sampling Method
A descriptive survey involving 280 participants from Global Evangelical Mission Hospital using questionnaires was undertaken from May 1, 2011 to April 30, 2012. The participants were assured of confidentiality prior the exercise; their consent was also sought before the exercise. Data was collected using a structured questionnaire. Demographic data was also obtained from them; these included their gender, age, religion and educational background.
2.3. Data Analysis
The descriptive data was presented using Statistical Package for Social Sciences (SPSS) 16.0 Edition. Graphs were drawn using Microsoft Excel.
2.4. Ethical Approval
The appropriate ethical approval was obtained from the Committee on Human Research, Publications and Ethics of the Kwame Nkrumah University of Science and Technology, School of Medical Sciences and Komfo Anokye Teaching Hospital, Kumasi.
3. Results
3.1. Demographic Features of Respondents
Out of the 280 participants, females were 57.1% (n = 160) and males, 42.9% (n = 120). Ages of the participants ranged from 15 - 70+ years with a mean age of 35.8 ± 1.5 (Figure 1). Concerning educational background, participants who had junior high education recorded the greatest number, 28.6%, followed by secondary education which recorded 22.9%, primary and tertiary education both recorded 17.1% while respondents who had never been to school constituted the least number of persons, 14.3%. In terms of religion, Christians recorded the greatest number, 71.4%, followed by Muslims, 20% and finally Traditional and other religions recorded 8.6%.
3.2. Quality Indicators Used for Assessing Wound Management
Out of the 280 participants interviewed, 28.6% (n = 80) indicated that attitude of staff was excellent, 65.7 % (n = 184) had good and 5.7 % (n = 16) had fair attitude (Figure 2).
Out of 280 participants, the condition of 168 (60.0%) required surgery while the condition of 112 (40.0%) did not require surgery. However, out of the 168 who underwent surgery, 32 (19.0%) were not satisfied while 136 (81.0%) were satisfied with the results (Figure 3).
Out of the 280 participants, 97.1% (n = 272) were accorded privacy; 51.4% (n = 144) were assured of confidentiality. More so, 48.6% (n = 136) were educated on diagnoses and treatment; 91.4% (n = 256) understood instructions given to them by pharmacists; 57.1% (n = 160) were satisfied with time spent in the facility; 2.9% (n = 8) of participants were shun by nurses because of their wound (Figure 4).
4. Discussion
4.1. Indicators
4.1.1. Attitude of Staff
The attitude of staff toward delivery of quality service cannot be understated. Most patients are offended by odd attitudes of medical workers especially when they are disrespectful and harsh. Even though patients may be satisfied with their treatment and care, staff’s behavior may reduce their satisfaction. From the current study, only 5.7% of participants stated that the staff attitude was fair and hence needed to sit up and relate to the needs of patients since this would help to promote excellent health outcome. People need to be listened to and understood in terms of what is important to them. They want to be treated as individuals, as we would ourselves. When dignity and respect are absent from care, people feel devalued, lack control and comfort. They may also lack confidence, be unable to make decisions for themselves, and feel humiliated, embarrassed and ashamed [5]. Love, care and support shown to patients are a step in the right direction to help them. The study by Walsh et al. (2002) involved interviews with nine staff and patients who
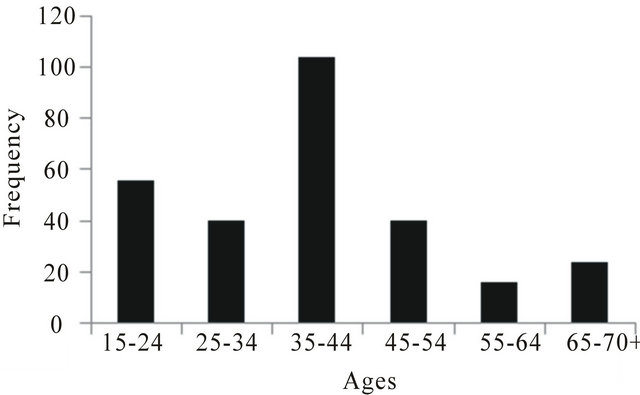
Figure 1. Age distribution of participants.
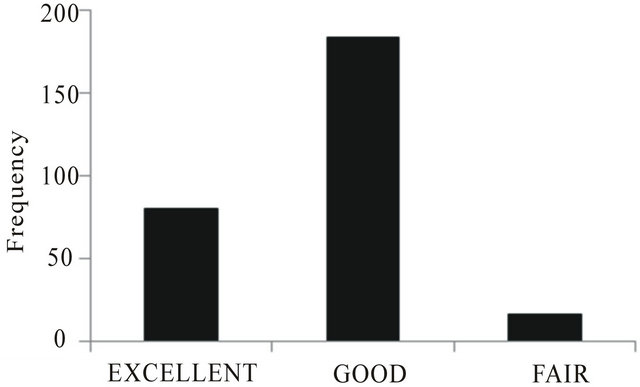
Figure 2. Attitude of staff.
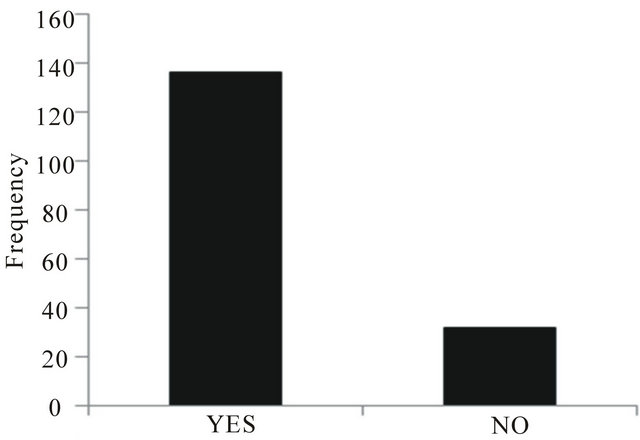
Figure 3. Patients’ satisfaction with surgery.
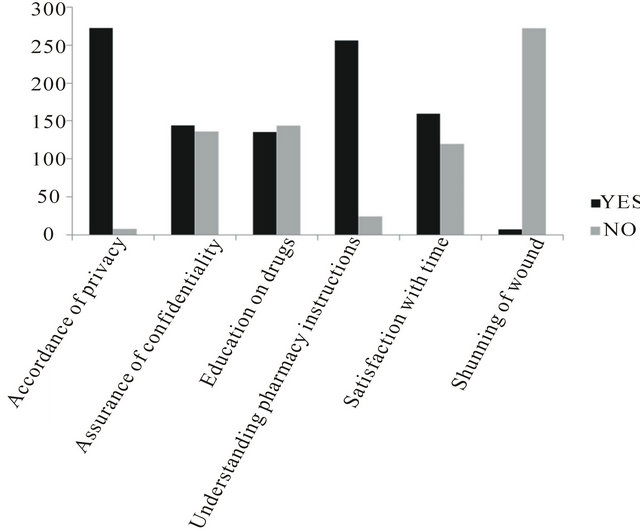
Figure 4. Indicators used in assessing quality assurance.
identified that staff behaviour could threaten or promote dignity [6]. The study’s findings supported previous research identifying that staff behaviour can threaten patients’ dignity [6-9].
4.1.2. Patients’ Satisfaction with Surgery
There is a need for patients to be counseled before they undergo surgery. Patients who are optimistic about surgery and are fully supported or not by relatives had higher satisfaction as compared to pessimistic patients who had support or no support. Williams et al. (1968) found out that high pre-operative anxiety levels can lead to increased post-operative analgesic requirement and prolonged hospital stay [10]. During the early stage after surgery, patients with a high degree of interpersonal sensitivity, whose close relatives do not support surgery, or who accept surgery passively tend to be more dissatisfied. Patients who have realistic expectations are more satisfied in the long term. Finally, it is important for clinicians to know that it has been clearly demonstrated that satisfied patients improve physician satisfaction [11]. Some pre-surgery and post-surgery photos are shown below (Figures 5-7).
4.1.3. Privacy
The privacy of every individual should be respected. Some patients would not like the presence of observers when undergoing certain treatments. Therefore the presence of other persons aside assigned health worker(s) and relative invade their privacy. The current study showed 97.1% of the respondents stated they were accorded privacy which has helped to promote very goodstaff and patient relationship. For those who were not accorded privacy they
 (a)
(a) (b)
(b)
Figure 5. (a) Pre-surgery (before operation); (b) Post-surgery (after operation—shaving and skin grafting).
 (a)
(a) (b)
(b)
Figure 6. (a) Pre-surgery (before operation); (b) Post-surgery (after operation—shaving and skin grafting).
 (a)
(a) (b)
(b)
Figure 7. (a) Pre-surgery (before operation); (b) Post-surgery (after operation—shaving and skin grafting.
stated, they were sometimes interrupted during their examination and felt a bit embarrassed. The patient has the right to privacy during consultation, examination and treatment. In cases where it is necessary to use the patient or his/her case notes for teaching and conferences, the consent of the patient must be sought [12]. Meredith and Wood (1996) reported in their study that, some patients were sometimes frustrated since they could not ask their consultants some sensitive questions because there was no privacy [13]. Clients want their privacy to be respected and time to build relationships with staff.
4.1.4. Confidentiality
People need to feel that their confidentiality is not being compromised and that their care is individualised and based around their specific circumstances. Confidentiality at health delivery centres is very important as it builds trust and can promote good communication and relation between patients and health care professionals. Patients would love to share their health problems to their health professionals but in the situation where the health worker seems unconcerned, it makes it difficult for patients to approach them and this breaks confidentiality. It also happens when health workers cannot keep patients’ problems shared secret. The study revealed almost a little above half of patients were assured of confidentiality, this is not the best; patients need to feel that they are accepted and valued, regardless of their life situation or lifestyle choices [5]. Ford and Cooke (1994) stated clients had to feel that they could expose parts of themselves in the safe and sure knowledge that they would not be judged, or the information used to refer them elsewhere or to discharge them from care [14].
4.1.5. Education on Diagnosis and Treatment
All clients should be informed about their condition and the necessary treatment being given to them. Patients need to be educated on the kind of treatment to be given to them. Knowledge about their treatment prepares them for other up-comings and promotes speedy recovery. Education on cause of sickness and treatment needs to be promoted as that will enhance health outcome. This study shows that 51.4% were not given any education. This is contrary to what is provided in the Patient Charter of Ghana Health Service (GHS), which states that “the patient is entitled to full information on his/her condition and management and the possible risks involved except in emergency situations when the patient is unable to make a decision and the need for treatment is urgent” [12]. Several studies have suggested that shared medical decision making between patients and providers can improve patient satisfaction and even improve some clinical outcomes [15-17].
4.1.6. Understanding Pharmacy Instructions
Patient’s satisfaction with healthcare encompasses all the units of healthcare system including the pharmacy. Drugs prescription is a very important aspect of patients’ care and treatment because it performs one of the major roles of the healing process. From the current study 8.6% of participants did not understand pharmacy instructions. Pharmacists need to explain instructions of drugs to patients to help them better understand and adhere to instructions. This would help them take their medications regularly and avoid over or under dosage; they can also report in case they suffer any allergic reaction and hence can be better taken care of. Lack of understanding by patients of their disease condition and treatment regimen may affect the medication adherence [18-20]. Many interventions designed to improve patient’s understanding have led to better adherence [21]. There is a need for pharmacists to offer pharmaceutical care to patients in order to improve their health needs not only dispensing the medication [22,23].
4.1.7. Satisfaction with Time
Time spent in healthcare facilities could sometimes be frustrating. Time lost can never be regained therefore it must be utilized judiciously. As the adage goes “time is money”; patients though are concerned with their health they cannot afford to waste a whole lot of time to seek medical treatment. Long waiting times at the hospital increases stress and frustration. This study shows 42.9% of patients were not satisfied with time spent in the facility. This was as a result of long queues at the Out Patients Department (OPD), delay in seeing the doctor, delay in collecting their medications at the pharmacy and delay in getting their laboratory tests done and their results; they stated all these delays are very costly to them and can prevent them from accessing some kind of service they need. Client satisfaction is an important measure of quality care [24] and has been identified as an important dimension for assessing the quality of health care services [25-27]. Bain et al. (1999) in his research stated that dissatisfaction was largely related to waiting times between admission, operation, and discharge [28]. Longer waiting times were associated with lower patient satisfaction. Furthermore, there is compelling evidence from well-developed lines of research demonstrating that increasing patient satisfaction improves clinical outcomes, such as functional status and physiological measures of health.
4.1.8. Shunning of Wound
Client satisfaction is an important measure of quality care [24]. The study shows that 2.9% of participants were shun by nurses because of their wounds. The nurses’ attitude could be as a result of patients not taking care of their dressings, others not reporting regularly for their dressings to be changed and therefore the wounds produced very offensive odour, very dirty or extremely soiled bandages, not applying medications to the wound regularly and as often as needed. In other situations, some patients proved to be difficult when they are being attended to; they make unnecessary complains and noise during wound dressing. But this notwithstanding, there should be tolerance, patience, love and much help given to patients as this would help to promote excellent outcome. Nurses who are satisfied with their jobs show higher levels of patient safety and less medication errors which help increase patient satisfaction [29]. Nursing attitude towards wound care should always aim at improving quality of life of the patients.
5. Conclusion
Quality assurance is very important in all units of the healthcare system. The need to provide quality healthcare to patients utilizing the various health facilities cannot be understated. Patients satisfaction is a necessary tool to improved health outcomes hence it is expedient that patients are given the kind of care they deserve in order to avoid under utilization or over-utilization of health resources. Patient satisfaction is met when quality assurance measures are put in place and implemented.
6. Acknowledgements
The author is grateful to Mr. Faith Amanfu, Miss Mayvor Agbenorku and Miss Catherine Acquaye for assisting in the data collection that formed the basis of this study.
REFERENCES
- P. L. N. Thi, et al., “Factors Determining Inpatient Satisfaction with Care,” Social Science & Medicine, Vol. 54, No. 4, 2002, pp. 493-504. doi:10.1016/S0277-9536(01)00045-4
- A. K. Offei, et al., “Healthcare Quality Assurance Manual, July 2004,” 2012. http://www.ghanaqhp.org/fileadmin/user_upload/QHP/Healthcare_Quality_subdistrict.pdf
- G. Schultz, G. Sibbald, V. Falanga, E. Ayello, C. Dowsett, K. Harding, M. Romanelli, M. Stacey, L. Teot and W. Vanscheidt, “Wound Bed Preparation: A Systematic Approach to Wound Management,” Wound Repair and Regeneration, Vol. 11, No. S1, 2003, pp. 1-28. doi:10.1046/j.1524-475X.11.s2.1.x
- S. Thomas, “Wound Management and Dressings,” The Pharmaceutical Press, London, 1990.
- Royal College of Nursing, “Defending Dignity: Challenges and Opportunities for Nursing,” RCN, London, 2008.
- K. Walsh and I. Kowanko, “Nurses’ and Patients’ Perceptions of Dignity,” International Journal of Nursing Practice, Vol. 8, No. 3, 2002, pp. 143-151. doi:10.1046/j.1440-172X.2002.00355.x
- J. Öhlén, “Violation of Dignity in Care-Related Situations,” Research and Theory for Nursing Practice, Vol. 18, No. 4, 2004, pp. 371-385.
- A. Gallagher and D. Seedhouse, “Dignity in Care: The Views of Patients and Relatives,” Nursing Times, Vol. 98, No. 43, 2002, pp. 39-40.
- M. R. Matiti, “Patient Dignity in Nursing: A Phenomenological Study,” Unpublished Thesis, University of Huddersfield, Huddersfield, 2002.
- J. G. I. Williams and J. R. Jones, “Psychophysiological Responses to Anesthesia and Operation,” Journal of the American Medical Association, Vol. 203, 1968, pp. 415- 417. doi:10.1001/jama.203.6.415
- P. J. Torcson, “Patient Satisfaction: The Hospitalist’s Role,” The Hospitalist, 2005, pp. 27-30.
- Ghana Health Service, “The Patients’ charter,” 2012. http://www.ghanahealthservice.org/aboutus.php?inf=Patients 
- P. Meredith and C. Wood, “Aspects of Patient Satisfaction with Communication in Surgical Care: Confirming Qualitative Feedback through Quantitative Methods,” International Journal for Quality in Health Care, Vol. 8. No. 3, 1996, pp. 253-264.
- J. Repper, R. Ford and A. Cooke, “How Can Nurses Build Trusting Relationships with People Who Have Severe and Long-Term Mental Health Problems? Experiences of Case Managers and Their Clients,” Journal of Advanced Nursing, Vol. 19, No. 6, 1994, pp. 1096-1104. doi:10.1111/j.1365-2648.1994.tb01193.x
- S. Kaplan, S. Greenfield and J. Ware, “Assessing the Effects of Physician-Patient Interactions on the Outcomes of Chronic Disease,” Medical Care, Vol. 27, No. 3, 1989, pp. 110-127. doi:10.1097/00005650-198903001-00010
- C. Laine and F. Davidoff, “Patient-Centered Medicine,” Journal of the American Medical Association, Vol. 175, 1996, pp. 152-156. doi:10.1001/jama.275.2.152
- J. M. Deadman, S. J. Leinster, R. G. Owens, M. E. Dewey and P. D. Slade, “Taking Responsibility for Cancer Treatment,” Social Science and Medicine, Vol. 53, No. 5, 2001, pp. 669-677. doi:10.1016/S0277-9536(00)00369-5
- W. Insull, “The Problem of Compliance to Cholesterol Altering Therapy,” Journal of Internal Medicine, Vol. 241, No. 4, 1997, pp. 317-325. doi:10.1046/j.1365-2796.1997.112133000.x
- K. P. Krueger, B. G. Felkey and B. A. Berger, “Improving Adherence and Persistence: A Review and Assessment of Interventions and Description of Steps toward a National Adherence Initiative,” Journal of the American Pharmacists Association, Vol. 43, No. 6, 2003, pp. 668- 678. doi:10.1331/154434503322642598
- J. H. LaRosa and J. C. LaRosa, “Enhancing Drug Compliance with Lipid-Lowering Treatment,” Archives of Family Medicine, Vol. 9, No. 10, 2000, pp. 1169-1175. doi:10.1001/archfami.9.10.1169
- R. B. Haynes, X. Yao, A. Degani, S. Kripalani, A. Garg and H. P. McDonald, “Interventions for Enhancing Medication Adherence,” Cochrane Database of Systematic Reviews, Vol. 16, No. 2, 2008, Article ID: CD000011.
- C. D. Hepler and L. M. Strand, “Opportunities and Responsibilities in Pharmaceutical Care,” American Journal of Hospital Pharmacy, Vol. 47, No. 3, 1990, pp. 533-543.
- J. C. Schommer and S. N. Kucukarslan, “Measuring Patient Satisfaction with Pharmaceutical Services,” American Journal of Health-System Pharmacy, Vol. 54, No. 23, 1997, pp. 2721-2732.
- A. Donabedian, “Exploration in Quality Assessment and Monitoring,” Vol. 1, Health Administration Press, Ann Arbor, 1980.
- M. Calnan, et al., “Major Determinants of Consumer Satisfaction with Primary Care in Different Health System,” Family Practice, Vol. 11, No. 4, 1994, pp. 468-478. doi:10.1093/fampra/11.4.468
- K. R. Epstein, C. Laine, N. J. Farber, E. C. Nelson and F. Davidoff, “Patients’ Perceptions of Office Medical Practice: Judging Quality through the Patients Eyes,” American Journal of Medical Quality, Vol. 11, No. 2, 1996, pp. 73-80. doi:10.1177/0885713X9601100204
- B. Williams, “Patient Satisfaction: A Valid Concept?” Social Science and Medicine, Vol. 38, No. 4, 1994, pp. 509- 516. doi:10.1016/0277-9536(94)90247-X
- J. Bain, H. Kelly, D. Snadden and H. Staines, “Day Surgery in Scotland: Patient Satisfaction and Outcomes,” Quality in Health Care, Vol. 8 No. 2, 1999, pp. 86-91. doi:10.1136/qshc.8.2.86
- C. Rathert and R. Douglas, “Health Care Work Environments, Employee Satisfaction, and Patient Safety: Care Provider Perspectives,” Health Care Management Review, Vol. 32, No. 1, 2007, pp. 2-11. doi:10.1097/00004010-200701000-00002