Surgical Science
Vol. 3 No. 1 (2012) , Article ID: 17015 , 4 pages DOI:10.4236/ss.2012.31007
The 45-Degree Arthroscope Improves Visualization of the Femoral Attachment of the Anterior Cruciate Ligament
Department of Orthopaedic Surgery, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan
Email: *okazaki@med.kyushu-u.ac.jp
Received September 16, 2011; revised December 9, 2011; accepted December 13, 2011
Keywords: Arthroscope; Knee; Anterior Cruciate Ligament (ACL); Surgical Device
ABSTRACT
Background: Exposure of the insertion site of the anterior cruciate ligament (ACL) is important for appropriate tunnel placement in ACL reconstruction surgery. However, observing the femoral ACL insertion site via the standard anterolateral portal is sometimes difficult. In this study, we compared views of the femoral ACL insertion site between 30-degree and the 45-degree arthroscopes. Methods: We first inserted the 30-degree and the 45-degree arthroscope into the anterolateral portal of a knee simulator in which we had drawn a lattice pattern on the lateral intercondylar notch based on the quadrant method. Next, we compared the arthroscopic views provided by the 30-degree and 45-degree arthroscopes during ACL reconstruction surgery by measuring the area of the lateral intercondylar notch visible through each of the arthroscopes. Results: In the knee simulator, the 45-degree arthroscope showed the entire area of the lateral intercondylar notch, whereas the 30-degree arthroscope had to be introduced more deeply to show the most superior and posterior quadrant, where the attachment of the anteromedial bundle of ACL is located. During the ACL reconstruction, the area of the lateral intercondylar notch in the field of view was larger through the 45-degree arthroscope than through the 30-degree arthroscope. Conclusion: The 45-degree arthroscope provides a better view of the femoral ACL insertion site via the anterolateral portal, which may be helpful during ACL reconstruction.
1. Introduction
Appropriate tunnel placement is one of the essential issues for successful anterior cruciate ligament (ACL) reconstruction. Recent detailed studies of the insertion site of the ACL have contributed to development of ACL reconstruction techniques and improvement in the accuracy of graft positioning [1-4]. Identification of the native ACL footprint plays an important part in anatomic ACL reconstruction surgery. The surgeon usually inserts the arthroscope via the anterolateral portal and inserts surgical devices via the anteromedial portal because the surgical devices can more easily gain access to the femoral ACL insertion site via the anteromedial portal. However, conditions during surgery can occasionally necessitate switching the portals, for instance, encountering difficulties in exposing the whole area of the ACL insertion site at the lateral femoral condyle when viewing via the anterolateral portal. We hypothesized that the 45-degree arthroscope would provide a better view of the femoral ACL insertion site than the standard 30-degree arthroscope. Before starting this study, we measured the angle of view of the 45-degree arthroscope and compared it with that of the 30-degree arthroscope. We found that the 45-degree arthroscope covers 0 to 90 degrees of view whereas the 30 degree arthroscope has a more limited range of 0 to 75 degrees, suggesting that the larger angle of the 45-degree arthroscope angle might improve the view of the lateral intercondylar notch via the anterolateral portal. The purpose of this study is to compare views of the femoral ACL insertion site between 30-degree and 45-degree arthroscopes.
2. Materials and Methods
2.1. Arthroscopes
Arthroscopes with two different oblique angles of 30 degrees and 45 degrees were purchased from Smith & Nephew Inc. (Andover, MA, USA).
2.2. Knee Simulator Model
We drew a lattice pattern on the lateral intercondylar notch of a Sawbone® knee simulator based on the quadrant method of Bernard et al. [5], in which the total sagittal diameter of the lateral femoral condyle along Blumensaat’s line is divided into quadrants on the lateral X-ray image. To apply this method to a three-dimensional bone model, we modified it by drawing multiple lines to divide up the distance from the edge of the articular surface to the posterior wall of the intercondylar notch along the roof of the notch. For the height of the lateral femoral condyle, we measured the distance from the roof of the notch to the edge of the articular surface and then drew a horizontal line dividing the distance in half. Zantop et al. reported the location of center of anteromedial bundle and posterolateral bundle of ACL on the quadrant method [2]. We marked the center of the femoral insertion of the anteromedial bundle and posterolateral bundle of the ACL in accord with the method described by Zantop et al. [2] We then placed the knee simulator on the table in a flexion angle of 50 degrees and introduced, in turn, the 30- and 45-degree arthroscopes via the anterolateral portal and via the anteromedial portal of the knee simulator. The arthroscope was held keeping the distal edge of the lateral intercondylar notch at the edge of view while the oblique face of the arthroscope pointed to 3 o’clock. The views from the 30- and 45-degree arthroscopes were compared.
2.3. In Vivo Measurement
We examined the femoral ACL insertion site in 15 knees with both the 30- and the 45-degree arthroscopes introduced via the anterolateral portal during ACL reconstruction surgery. We placed the anterolateral portal approximately 1cm above the lateral joint line and adjacent to the lateral margin of the patellar tendon. The arthroscope was held keeping the distal edge of the lateral intercondylar notch at the edge of view while the oblique face of the arthroscope pointed to either 3 o’clock for left knees or 9 o’clock for right knees. We measured the area of the lateral intercondylar notch using image J software (public domain software). The ratio of the area of the lateral intercondylar notch to the area of the whole arthroscopic view provided by the 30-degree arthroscope was compared with that provided by the 45-degree arthroscope. We used the Wilcoxon signed-rank test for our statistical analysis, setting the level of statistical significance at p < 0.05.
3. Results
3.1. Analysis in the Knee Simulator Model
Using a knee simulator, we compared views of the lateral intercondylar notch on which we had drawn a lattice pattern based on the quadrant method (Figure 1). The 45- degree arthroscope was able to encompass the entire lattice pattern via the anterolateral portal, whereas the 30-degree arthroscope could visualize only the anterior two quadrants. When we positioned the arthroscope to keep the edge of view on the most proximal tangent line, the mark on the femoral attachment of the anteromedial bundle was visible only in the 45-degree arthroscope (Figures 1(a) and (b)), whereas the 30 degree arthroscope had to be introduced more deeply towards the second tangent line to show the mark (Figure 1(c)). Identification of the posterior edge of the lateral intercondylar notch (the fifth tangent line) was easier using the 45-degree arthroscope than the 30-degree arthroscope (Figures 1(c) and (d)). On the other hand, we obtained good visualization with both arthroscopes via the anteromedial portal (Figures 1(e) and (f)).
3.2. In Vivo Measurement during ACL Reconstruction
During ACL reconstruction, we compared views of the

Figure 1. A lattice pattern is drawn on a Sawbone knee simulator based on the quadrant method. The horizontal line divides the height of lateral femoral condyle in half. The arthroscopes were introduced via the anterolateral portal and held in the same position, keeping the edge of view on the most proximal tangent line (a), (b) or on the second tangent line (c), (d). The arthroscopes also were introduced via the anteromedial portal (e), (f). The most superior and posterior quadrant, which contains the femoral attachment of the anteromedial bundle of the ACL (white asterisk), can be seen more clearly in the images from the 45-degree arthroscope (b), (d) than in the images from the 30-degree arthroscope (a), (c). The black asterisk identifies the attachment of the posterolateral bundle of the ACL.
lateral intercondylar notch after removal of the ACL remnant (Figure 2). We used image J software to measure the visible area of the lateral wall of the intercondylar notch through the 45-degree and 30-degree arthroscopes, positioning both arthroscopes the same. The area of the lateral intercondylar notch was 48.3% ± 22.0% (mean ± SD) larger in the view provided by the 45-degree arthroscope than in the view provided by the 30-degree arthroscope via the anterolateral portal (Table 1). No significant difference in viewing area was observed between arthroscopes via the anteromedial portal.
4. Discussion
Our study results demonstrated that the 45-degree arthroscope provided a wider viewing field and improved visualization of the lateral intercondylar notch via the anterolateral portal compared with the 30-degree arthroscope, which in turn suggests that the 45-degree arthroscope would improve the view of femoral ACL attachment in this orientation. On the other hand, neither arthroscope was superior to the other when viewing via the anteromedial portal.
Obtaining a good view of the femoral attachment of the ACL is key to creating a proper femoral tunnel. Several cadaveric studies have described the location of the ACL insertion site. Burnard et al. reported that the center of the femoral insertion site of the whole ACL was located at the corner of most superoposterior quadrant, as they defined their quadrants [5]. More recent studies have identified the location of both the anteromedial (AM) bundle and the posterolateral (PL) bundle of the ACL. Zantop et al. reported that the center of the AM bundle was located 5.3 mm from the notch and 5.7 mm from the intercondylar line, while the center of the PL bundle was located 9.5 mm from the shallow cartilage margin and 5.8 mm from the inferior cartilage margin [2].
In cases where observing the ACL attachment via the anterolateral portal proves difficult, the surgeon should be prepared to employ alternative methods to obtain a better view. Since a medially located portal improves visualization of the lateral intercondylar notch, one possible alternative is to switch the viewing portal to the anteromedial portal during surgery. Another approach would be to create a different portal, such as a transpatellar portal. Some surgeons use a 70-degree arthroscope to improve their view when looking at the femoral attachment. Our study findings indicate that a 45-degree arthroscope can provide a good view of the femoral attachment via the standard anterolateral portal.
The transtibial technique of ACL reconstruction consists of drilling a femoral tunnel through the tibial tunnel. This technique has been widely used for a long time [6,7] and may be familiar to many surgeons. This technique requires introduction of the tibial drilling guide via the anteromedial portal while looking through the arthroscope via the anterolateral portal. Because the femoral tunnel is drilled from the tibial tunnel, accurate determination of the direction of drilling for the tibial tunnel is vital to subsequently positioning the femoral tunnel at an ideal point on the femoral attachment of the ACL. Therefore, placing the tibial drilling guide at the center of the tibial insertion site while simultaneously correctly aiming the guide towards the subsequent femoral drilling site is critical to a successful femoral drilling outcome. To achieve this, good visualization of the femoral insertion site from the anterolateral portal is required because the anteromedial portal is occupied by the tibial guide during tibial drilling in this technique. Although the transtibial technique is relatively straightforward, some articles have noted difficulties in positioning the femoral tunnel at an optimal location through the tibial tunnel [8,9]. Alternative approaches are available, including drilling the femoral tunnel from an accessory far-medial portal or employing an outside-in technique while looking at the
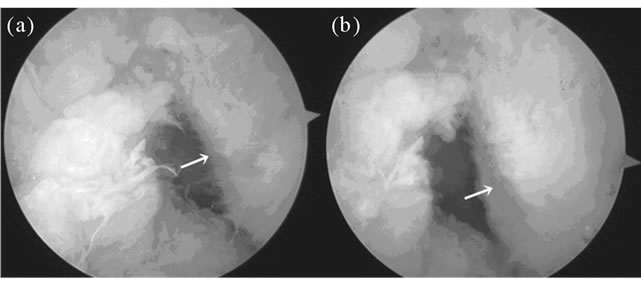
Figure 2. Arthroscopic views during the ACL reconstruction surgery. The 30-degree (a) or 45-degree; (b) Arthroscope is positioned to maintain the edge of view on the anterior border of the lateral intercondylar notch. The visible area of the lateral intercondylar notch is measured with image J software. The area from the 45-degree arthroscope was 38% larger than that from the 30-degree arthroscope in this case. The 45-degree arthroscope showed the ACL footprint (arrow) more clearly than the 30-degree arthroscope.

Table 1. The ratio of the area of the lateral intercondylar notch to the area of the whole arthroscopic view (average ± SD, %).
femoral insertion site from the anteromedial portal, which provides a better view [8,10-13]. However, for surgeons utilizing the transtibial technique for ACL reconstruction, the improved view of the femoral insertion site via the anterolateral portal afforded by the 45-degree arthroscope should be especially helpful for properly angling the drill so as to optimally direct the tibial tunnel towards the femoral attachment.
5. Conclusion
The current study shows that a 45-degree arthroscope provides an improved visualization of femoral ACL attachment from the anterolateral portal compared with a 30-degree arthroscope inserted from the same portal. An improved view of the ACL insertion site via the anterolateral portal may be particularly helpful to surgeons when they need to use the anteromedial portal for surgical devices.
6. Competing Interests
The authors declare that they have no competing interests.
7. Authors’ Contributions
KO conceived of the study and participated in its design. SM and YT participated in the design of the study. YI organized the study group and participated in the final decisions regarding this study.
REFERENCES
- S. Kopf, V. Musahl, S. Tashman, M. Szczodry, W. Shen and F. H. Fu, “A Systematic Review of the Femoral Origin and Tibial Insertion Morphology of the ACL,” Knee Surgery, Sports Traumatology, Arthroscopy, Vol. 17, No. 3, 2009, pp. 213-219. doi:10.1007/s00167-008-0709-5
- T. Zantop, M. Wellmann, F. H. Fu and W. Petersen, “Tunnel Positioning of Anteromedial and Posterolateral Bundles in Anatomic Anterior Cruciate Ligament Reconstruction: Anatomic and Radiographic Findings,” American Journal of Sports Medicine, Vol. 36, No. 1, 2008, pp. 65-72. doi:10.1177/0363546507308361
- S. Lorenz, F. Elser, M. Mitterer, T. Obst and A. B. Imhoff, “Radiologic Evaluation of the Insertion Sites of the 2 Functional Bundles of the Anterior Cruciate Ligament Using 3-Dimensional Computed Tomography,” American Journal of Sports Medicine, Vol. 37, No. 12, 2009, pp. 2368-2376. doi:10.1177/0363546509341577
- K. Shino, T. Suzuki, T. Iwahashi, T. Mae, N. Nakamura, K. Nakata and S. Nakagawa, “The Resident’s Ridge as an Arthroscopic Landmark for Anatomical Femoral Tunnel Drilling in ACL Reconstruction,” Knee Surgery, Sports Traumatology, Arthroscopy, Vol. 18 No. 9, 2010, pp. 1164-1168. doi:10.1007/s00167-009-0979-6
- M. Bernard, P. Hertel, H. Hornung and T. Cierpinski, “Femoral Insertion of the ACL. Radiographic Quadrant Method,” American Journal of Knee Surgery, Vol. 10, No. 1, 1997, pp. 14-22.
- P. Aglietti, R. Buzzi, S. D’Andria and G. Zaccherotti, “Arthroscopic Anterior Cruciate Ligament Reconstruction with Patellar Tendon,” Arthroscopy, Vol. 8, No. 4, 1992, pp. 510-506. doi:10.1016/0749-8063(92)90017-6
- G. T. Hardin, B. R. Bach Jr., C. A. Bush-Joseph and J. Farr, “Endoscopic Single-Incision Anterior Cruciate Ligament Reconstruction Using Patellar Tendon Autograft: Surgical Technique. 1992 [Classical Article],” Journal of Knee Surgery, Vol. 16, No. 3, 2003, pp. 135-144; discussion 145-147.
- E. S. Abebe, C. T. Moorman III, T. S. Dziedzic, C. E. Spritzer, R. L. Cothran, D. C. Taylor, W. E. Garrett Jr. and L. E. DeFrate, “Femoral Tunnel Placement during Anterior Cruciate Ligament Reconstruction: An in Vivo Imaging Analysis Comparing Transtibial and 2-Incision Tibial Tunnel-Independent Techniques,” American Journal of Sports Medicine, Vol. 37, No. 10, 2009, pp. 1904-1911. doi:10.1177/0363546509340768
- M. K. Kaseta, L. E. DeFrate, B. L. Charnock, R. T. Sullivan and W. E. Garrett Jr., “Reconstruction Technique Affects Femoral Tunnel Placement in ACL Reconstruction,” Clinical Orthopaedics and Related Research, Vol. 466, No. 6, 2008, pp. 1467-1474. doi:10.1007/s11999-008-0238-z
- T. Zantop, A. K. Haase, F. H. Fu and W. Petersen, “Potential Risk of Cartilage Damage in Double Bundle ACL Reconstruction: Impact of Knee Flexion Angle and Portal Location on the Femoral PL Bundle Tunnel,” Archives of Orthopaedic and Trauma Surgery, Vol. 128, No. 5, 2008, pp. 509-513. doi:10.1007/s00402-007-0480-y
- K. Shino, K. Nakata, N. Nakamura, Y. Toritsuka, S. Horibe, S. Nakagawa and T. Suzuki, “Rectangular Tunnel Double-Bundle Anterior Cruciate Ligament Reconstruction with Bone-Patellar Tendon-Bone Graft to Mimic Natural Fiber Arrangement,” Arthroscopy, Vol. 24, No. 10, 2008, pp. 1178-1183. doi:10.1016/j.arthro.2008.06.010
- C. A. Q. Martins, E. J. Kropf, W. Shen, C. F. van Eck and F. H. Fu, “The Concept of Anatomic Anterior Cruciate Ligament Reconstruction,” Operative Techniques in Sports Medicine, Vol. 16, No. 3, 2008, pp. 104-113. doi:10.1053/j.otsm.2008.10.008
- T. Zantop, S. Kubo, W. Petersen, V. Musahl and F. H. Fu, “Current Techniques in Anatomic Anterior Cruciate Ligament Reconstruction,” Arthroscopy, Vol. 23, No. 9, 2007, pp. 938-947. doi:10.1016/j.arthro.2007.04.009
NOTES
*Corresponding author.