World Journal of Cardiovascular Diseases
Vol.3 No.2(2013), Article ID:30390,2 pages DOI:10.4236/wjcd.2013.32032
Computed tomography imaging of an ectopic thyroid on the ascending aorta*
![]()
1Department of Cardiovascular Radiology, The First Affiliated Hospital of Dalian Medical University, Dalian, China
2Department of Cardiovascular Surgery, The First Affiliated Hospital of Dalian Medical University, Dalian, China
Email: #wzx1128@163.com
Copyright © 2013 Chongfu Jia et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 15 January 2013; revised 10 March 2013; accepted 13 April 2013
Keywords: Aorta; Tomography; X-Ray Computed; Ectopic Thyroid
ABSTRACT
Ectopic thyroid on the ascending aorta is extremely rare, and its radiologic characteristics have not been reported in the radiologic literature. A case of ectopic thyroid on the ascending aorta is reported, and its imaging characteristics on computed tomography are discussed.
1. INTRODUCTION
Ectopic thyroid has been found mainly in midline locations from the tongue to the mediastinum, the lingual thyroid is the most common site and found in 90% of ectopic thyroid cases [1]. Ectopic thyroid on the ascending aorta is extremely rare. To our knowledge, only 3 cases of ectopic thyroid on the ascending aorta have been previously reported in the literature [2-4]. Its imaging characteristics have not been described in the radiologic literature, however. We report a case of ectopic thyroid on the ascending aorta and discuss its imaging characteristics on computed tomography (CT).
2. CASE REPORT
A 56-year-old woman was admitted to our hospital with a history of chest pain and palpitation. Transthoracic echocardiogram showed a mass on the right atrium. Before excision, the patient underwent a preoperative cardiac computed tomography angiography to rule out coronary artery disease. Plain CT scan demonstrated a well-circumscribed round mass (4.8 cm ´ 4.9 cm ´ 6.2 cm) of high density (72 Hounsfield units [HU]) near the ascending aorta on the right atrium. After contrast injection, the mass was enhanced dramatically (130HU). A punctiform calcification and small low density areas in the mass were seen. Small vessels arising from ascending aorta supplied the mass. Pericardium and right atrium were oppressed by the mass (Figures 1(a)-(c)).
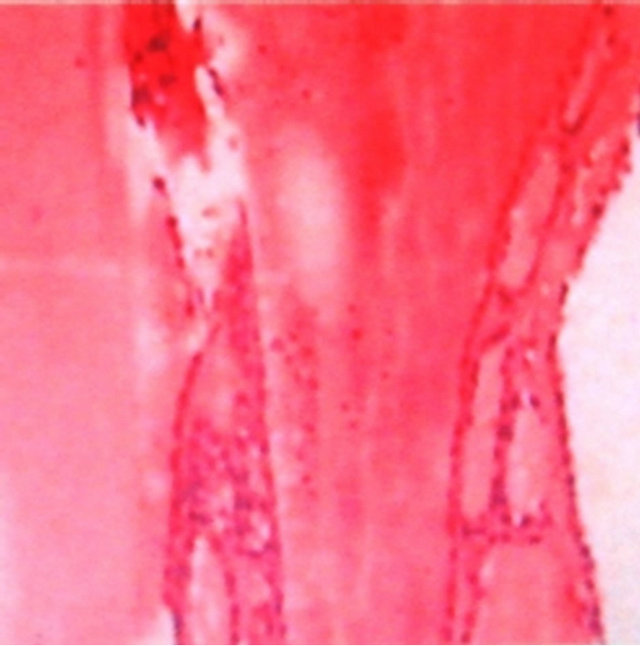
The patient underwent a sternotomy and on opening the pericardium, a firm and encapsulated tumor was found attached to the anterolateral surface of the ascending aorta. The small vessels arising from ascending aorta supplying the tumor was ligated. The tumor was resected completely. Histopathologic examination identified the tumor as an ectopic nodular goiter (Figure 1(d)).
The patient’s postoperative course was uneventful. The cervical ultrasonography showed thyroid tissue in the normal anatomic position. The patient’s thyroid function was normal.
3. DISCUSSION
Ectopic thyroid in the anterior mediastinum, pericardium, or heart has probably originated embryologically from rudiments of developing thyroid dragged into the chest during the descent of the heart and great vessels with the development of the embryonic neck and the unfolding of the embryo [5]. During embryogenesis, as the heart and aorta descend, the thyroid is drawn caudally, and it is thought that ectopic mediastinal thyroid tissue occurs as a result of abnormal positional relationships; thus, ectopic thyroid on the ascending aorta is the result of over-descending in our patient.
In general, ectopic thyroid has imaging characteristics similar to normal thyroid tissue which is higher in density than muscle tissue on plain CT image because of its high concentration of iodine, and is enhanced dramatically after contrast injection because of its rich blood vessel. Thus, ectopic thyroid can usually be differentiated from other mass near the ascending aorta on CT.
 (a)
(a)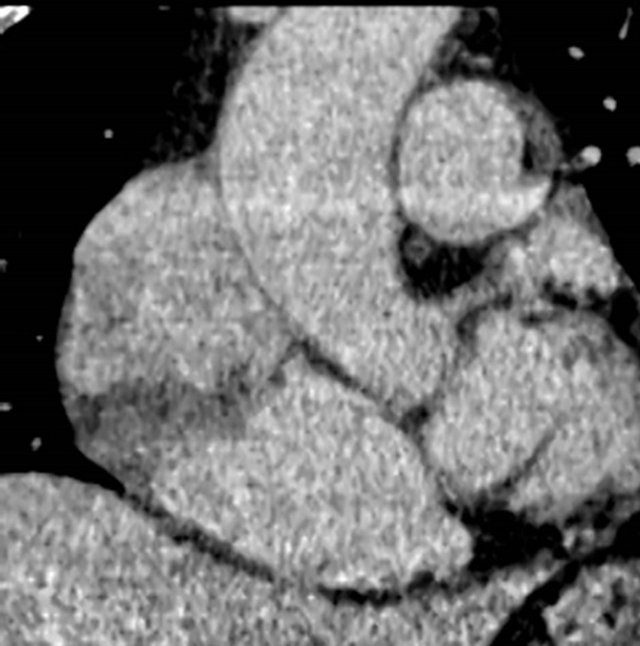 (b)
(b)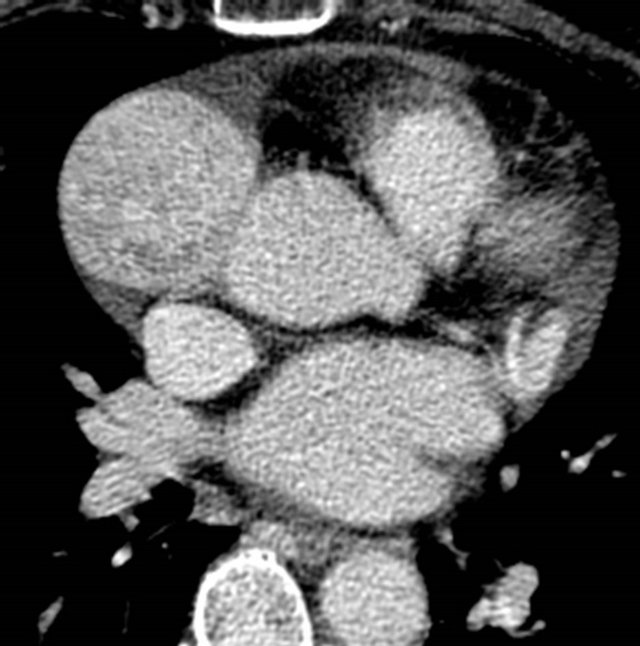 (c)
(c) (d)
(d)
Figure 1. (a) Plain CT image shows a well-circumscribed round mass (4.8 cm ´ 4.9 cm ´ 6.2 cm) of high density near the ascending aorta on the right atrium(arrow); (b) Enhanced CT image shows dramatic enhancement mass with small low density areas in it (arrow); (c) Multiplanar reconstructed CT image shows right atrium (black arrow) that is oppressed by the mass near the ascending aorta (white arrow); (d) Histopathologic examination shows the tumor as an ectopic nodular goiter (H&E, ×100).
There are some reports in which the utility of CT in diagnosing of ectopic thyroid was described [6-8]. In our patient, plain CT image showed a mass near the ascending aorta of higher density and was enhanced dramatically after contrast injection, these provided the diagnosis of ectopic thyroid probably. Diseases such as goiter or Papillary carcinoma which occur in the normal thyroid may also occur in ectopic thyroid [4,9,10]. In our patient, CT image showed a punctiform calcification and small low density areas in the mass suggestive of goiter.
In conclusion, we reported a case of ectopic thyroid on the ascending aorta, and described its imaging characteristics on CT. We recommend when a mass near the ascending aorta is detected on CT, especially with the imaging characteristics we have discussed above, ectopic thyroid must be considered in the differential diagnosis.
REFERENCES
- Noyek, A.M. and Friedberg, J. (1981) Thyroglossal duct and ectopic thyroid disorders. Otolaryngologic Clinics of North America, 14, 187-201.
- Taylor, M.A., Bray, M. and Roberts, W.C. (1986) Aberrant thyroid gland attached to ascending aorta. American Journal of Cardiology, 57, 708.
- Williams, R.J., Lindop, G. and Butler, J. (2002) Ectopic thyroid tissue on the ascending aorta: An operative finding. The Annals of Thoracic Surgery, 73, 1642-1643. doi:10.1016/S0003-4975(01)03439-7
- Ozpolat, B., Dogan, O.V., Gökaslan, G., et al. (2007) Ectopic thyroid gland on the ascending aorta with a partial pericardial defect: Report of a case. Surgery Today, 37, 486-488. doi:10.1007/s00595-006-3439-7
- Gamblin, T.C., Jennings, G.R., Christie, D.B., et al. (2003) Ectopic thyroid. The Annals of Thoracic Surgery, 75, 1952-1953. doi:10.1016/S0003-4975(03)00007-9
- Declerck, S., Casselman, J.W., Depondt, M., et al. (1993) Lingual thyroid imaging. Journal Belge de Radiologie, 76, 241-242.
- Glazer, G.M., Axel, L. and Moss, A.A. (1982) CT diagnosis of mediastinal thyroid. American Journal of Roentgenology, 138, 495-498. doi:10.2214/ajr.138.3.495
- Kobayashi, H., Tashita, H., Hara, H., et al. (2005) Utility of computed tomography in identifying an ectopic thyroid in infants and pre-school children. Endocrine Journal, 52, 189-192. doi:10.1507/endocrj.52.189
- Lee, C.C., Chen, C.Y., Chen, F.H., et al. (1998) Imaging of huge lingual thyroid gland with goiter. Neuroradiology, 40, 335-337. doi:10.1007/s002340050595
- Kandogan, T., Erkan, N. and Vardar, E. (2008) Papillary carcinoma arising in subhyoid ectopic thyroid gland. Thyroid, 18, 477-478. doi:10.1089/thy.2007.0240
NOTES
*We have no conflict of interest regarding our article.
#Corresponding author.