Journal of Cosmetics, Dermatological Sciences and Applications
Vol. 2 No. 2 (2012) , Article ID: 20115 , 6 pages DOI:10.4236/jcdsa.2012.22016
Facial Skin Rejuvenation with High Frequency Ultrasound: Multicentre Study of Dual-Frequency Ultrasound*
![]()
1Derma-Clinic, Karlsruhe, Germany; 2Die Ästheten, Munich, Germany; 3Optima Clinic, Karlsruhe, Germany; 4Skinline Clinic, SintPieters-Leeuw, Belgium; 5Wellcomet GmbH, Karlsruhe, Germany.
Email: dirk@meyer-rogge.de
Received March 27th, 2012; revised April 30th, 2012; accepted May 14th, 2012
Keywords: Skin Rejuvenation; Dual-Frequency Ultrasound; Matrix Metalloproteinases; Heat Shock Proteins
ABSTRACT
According to modern theories, the process of skin ageing may be connected with local up-regulation of matrix metalloproteinases (MMP) and down-regulation of heat shock proteins (HSP) in the skin. In this pragmatic, non-randomised, multicentre study we investigated the skin rejuvenation effect of dual-frequency ultrasound, with frequencies of 3 and 10 MHz, which has the ability to modulate both MMPs and HSPs. It was shown that such waves can significantly improve different visual appearances of ageing skin. This safe, non-invasive method yields results that are not as marked as those shown by injecting of fillers, but can be successfully used by subjects with a broad spectrum of visual skin ageing problems, which have to be treated simultaneously.
1. Introduction
Skin ageing is a continuous process, which occurs on a cellular as well as on a molecular level. It is traditionally divided into intrinsic (chronological) and extrinsic ageing. The former is considered to be genetically pre-determined; the latter is mainly caused by different environmental factors. These two ageing processes have different pathophysiological mechanisms and lead to different visual changes of the skin. It is strongly believed that intrinsic ageing is mainly responsible for skin appearances such as fine wrinkles, a reduction in firmness, enlarged pores, sagging and dryness as well as for thin and fragile skin. Extrinsic ageing is connected with the production of fine and coarse wrinkles, skin hyperpigmentation, loss of skin turgor, freckles and roughness as well as with dilatation of blood vessels.
The reasons for intrinsic skin ageing are largely unknown. One classic pathophysiological mechanism is the excessive oxidative phosphorylation with an accumulation of superoxides. Another is a continuous reduction in the number of synthetically active fibroblasts, which are mainly responsible for the dynamic balance in the active connective tissue and the progressive accumulation of senescent fibrocytes presented in inactive connective tissue. This process leads to the subsequent reduction in collagen content in the ageing skin [1] and may be also responsible for the reduction of glycosaminoglycanes, which, consequently, can modify the skin micro-relief and reduce its turgor. These mechanisms can be also involved in extrinsic ageing.
Two other pathophysiological mechanisms of skin ageing have recently been proposed. The first is based on the overproduction of matrix metalloproteinases (MMPs) as a result of chronic, intrinsic inflammation or external exposure to UVor IR-radiation. Connective tissue normally stands in dynamic balance between the processes of its production and destruction. A temporary increase in MMPs activity makes this system unbalanced, increasing the rate of its destruction. Depending on the duration and strength of this process, the connective tissue structure and its mechanical properties can afterwards fully or partly restore. MMPs activation occurs in both chronological and photo-induced skin ageing [2-5]. The increase in MMPs activity can be dramatic, even with sub-erythemal doses of UV radiation, which could be enough for significant degradation of dermal connective tissues [2]. Such pathophysiology of skin ageing led to the formulation of new prevention and treatment strategies for anti-ageing therapy that are based on the inhibition of production and/or activity of some specific MMPs in the skin [4].
The second new pathophysiology of skin ageing is connected with the phenomenon of continuously reduced production of heat shock proteins (HSPs) in ageing skin. Modulation of HSPs is actually considered to be an important component of the treatment strategy in modern gerontology used to delay the ageing processes and/or to reduce the signs of ageing [6-8]. This effect can be, at least partly, explained through the correlation of HSPs content with fibroblasts’ activity and their collagen production [9,10].
These pathophysiological features of skin ageing led to the development of new anti-ageing treatment strategies based on the modulation of the local MMPs and/or HSPs activity in the skin. Such modulation can lead to the dynamic balance in the connective tissue being restored, improving its mechanical properties and consequently reducing visual ageing appearances of the skin such as wrinkles and pores as well as increasing the skin turgor.
The aim of this study was to assess the efficacy of high-frequency dual-wave ultrasound (US) with frequencies of up to 10 MHz in facial anti-ageing treatments. This dual-frequency modality has demonstrated high efficiency in the modulation of both MMPs (results not published) and HSPs in vitro [11], which made it possible to formulate the hypothesis of anti-ageing treatment strategy through the application of 10 MHz US [12]. The high efficacy of dual-frequency US waves for treatment of ulcus cruris, which apparently also needs the modulation of different MMPs and HSPs in the wound, was recently demonstrated [13].
2. Study Protocol
In this pragmatic, non-randomised, multicentre study we tested the skin rejuvenation effect of dual-frequency US waves with frequencies of 3 and 10 MHz. The wave formation (LDM®) is shown in Figure 1 and was described in detail in [13]. The commercially available machine, LDM®-MED (Wellcomet, Germany), was used as a dual wave generator. US intensity was controlled by the digital US power meter UPM-DT-10 (Ohmic Instruments Co., USA).
Since it is well known that participants can correctly identify whether their treatment consisted of placebo or active US (especially for high US intensities, which were used in this study) [14], it was not possible to blind neither participants nor the study nurses and the doctors.
2.1. Participants
As a preliminary step to this study, two subjects received
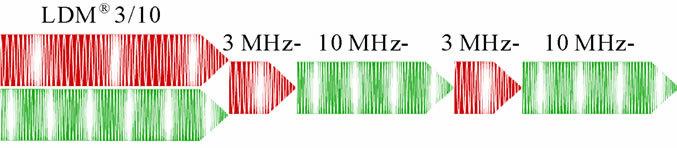
Figure 1. Wave formation in dual wave LDM® technology.
one half of their faces treated in a contra-lateral control test to exclude the placebo effect.
39 healthy subjects (32 females and seven males) without signs of severe sun-damaged skin, between the ages of 30 and 63 years were selected for this study that was trialled in four medical centres. Sample size estimation for the multicentre study was done in a preliminary pilot study with 12 subjects in accordance with the sample sizes evaluation for descriptive studies [15].
2.2. Interventions
All subjects were treated twice per week with the number of sessions totalling between eight and twelve. One whole-face treatment lasted 20 minutes and had the following parameters: 10 MHz, continuously at an intensity of 1.5 W/cm2 for 10 minutes, then LDM 3/10 MHz (3 ms 3 MHz/7 ms 10 MHz) at US intensity of 1.5 W/cm2. During the treatment the whole face was treated uniformly. The treatment was done semi-statically with an approximately 10 second application per spot. Normal US contact gel was used as a coupling medium.
The staff at each participating clinic received the same in-house training for the technique of US application.
2.3. Clinical Assessments
The following skin conditions were evaluated and documented before the first treatment and approximately one week after the last treatment: fine/coarse wrinkles, skin pores and skin turgor.
The severity of wrinkles was rated according to the 5-grade Wrinkle Severity Rating Scale (WSRS) [16]: 1) absent, continuous skin line; 2) mild wrinkles, minor facial feature; 3) moderate wrinkles, clear facial feature visible at normal appearance but not by stretching; 4) severe wrinkles, prominent facial feature, less than 1 mm deep when stretched; 5) very severe wrinkles, prominent facial feature, more than 1 mm deep when stretched. The length, width and depth of wrinkles were taken into account by rating. The reliability and statistical significance of WSRS scoring was confirmed in [17].
The same rating method was applied for the classification of skin pores: 1) almost no visible pores; 2) mild pores; 3) moderate pores; 4) enlarged pores; 5) very enlarged pores.
Skin turgor was evaluated according to the 5-grade Global Aesthetic Improvement Scale (GAIS) [18]: 1) worse than before the treatment; 2) no change; 3) obvious improvement; 4) marked improvement; 5) strong improvement.
Additionally, the satisfaction of the participants (PS) and of the doctors (DR) was evaluated according to a 10-grade scale between 0 and 10: 0-dissatisfied; 10-maximum satisfaction.
All the participating doctors received the in-house training for evaluation procedures. Statistical evaluation of treatment results was provided with c2-test.
3. Results
All the patients showed more than one kind of skin improvement. The first visual changes were normally seen after the first treatment; mainly this was pore reduction and/or turgor improvement.
The non-placebo effect of this treatment was evidenced by face splitting. Both treated subjects demonstrated an obvious improvement in skin condition on the treated side directly after the therapy (Figure 2).
Coarse wrinkles (CW) and fine wrinkles (FW) in the participants of the multicentric study were improved by 0.63 ± 0.72 WSRS grades (p < 0.05, c2-Test) (Figure 3) and by 0.73 ± 0.52 WSRS grades (p < 0.05, c2-Test) (Figure 4) from baseline, respectively. The skin pores (SP) were improved by 0.65 ± 0.57 WSRS grades (p < 0.05, c2-Test) (Figure 5). Skin turgor (ST) was increased by 2.88 ± 0.71 GAIS grades (Figure 6), showing on average an “obvious improvement”, according to the GAIS scale, which supports the statistical significance of this parameter [18].
The satisfaction of participants and doctors was 6.87 ± 1.68 and 7.23 ± 1.62, respectively (Figure 7); the difference was statistically insignificant. The coefficient of correlation between PS and DS was 0.75, which demonstrates good compliance of result assessment in both groups.

Figure 2. Change of the skin condition after one treatment. Face splitting with contra-lateral control to exclude a placebo effect. The change of the pores’ structure and wrinkles is clearly seen.
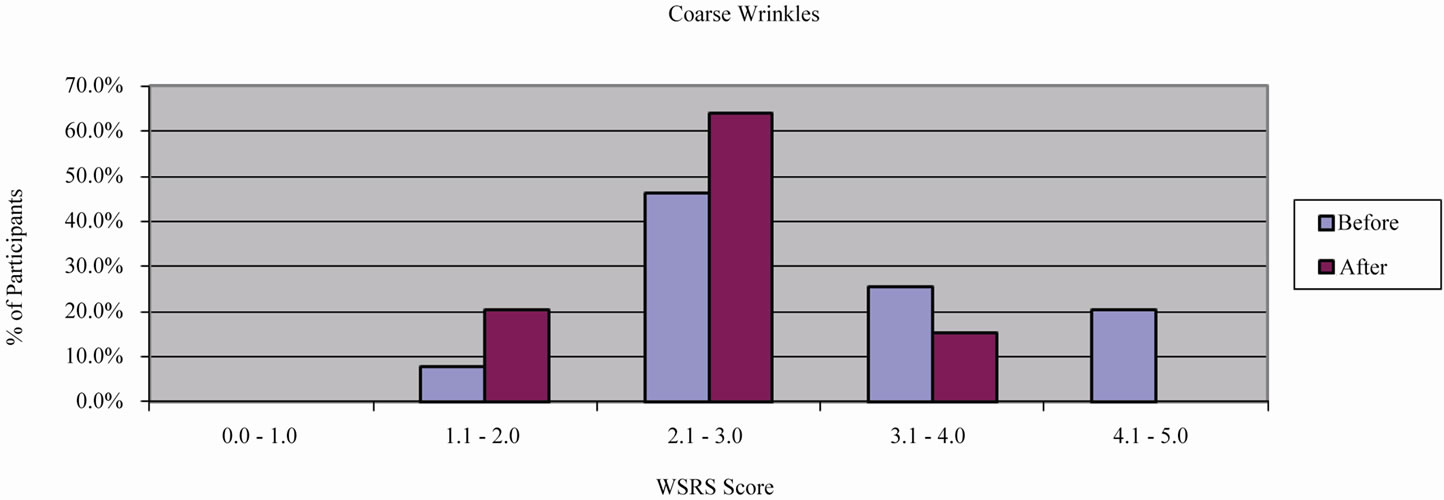
Figure 3. Investigator-graded WSRS score for coarse wrinkles.
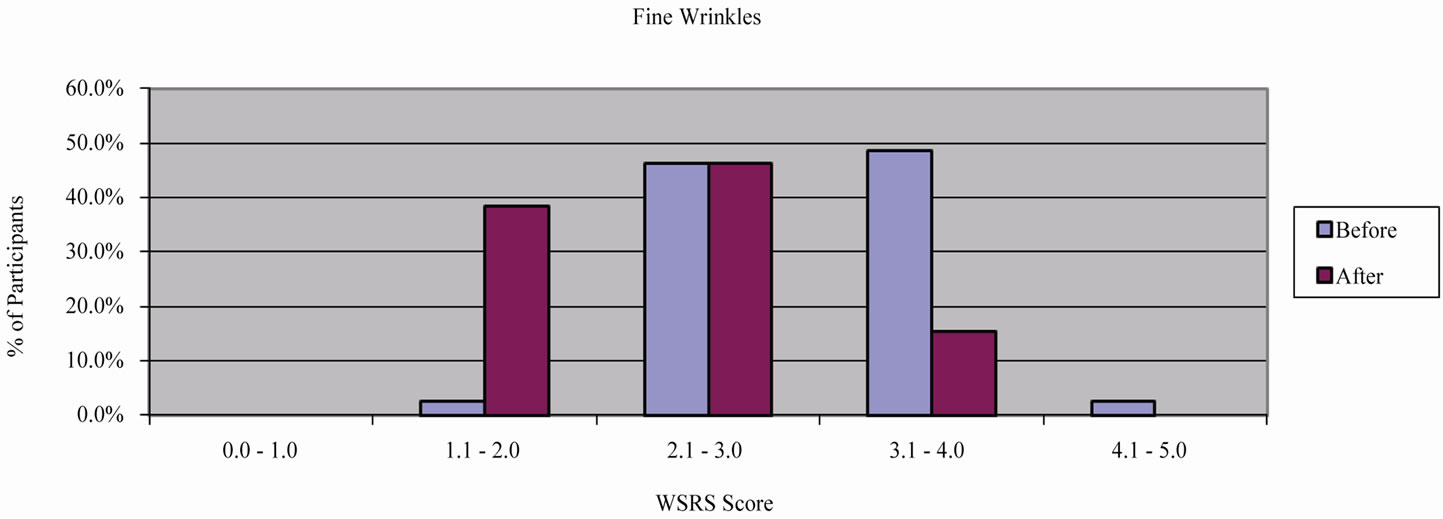
Figure 4. Investigator-graded WSRS score for fine wrinkles.
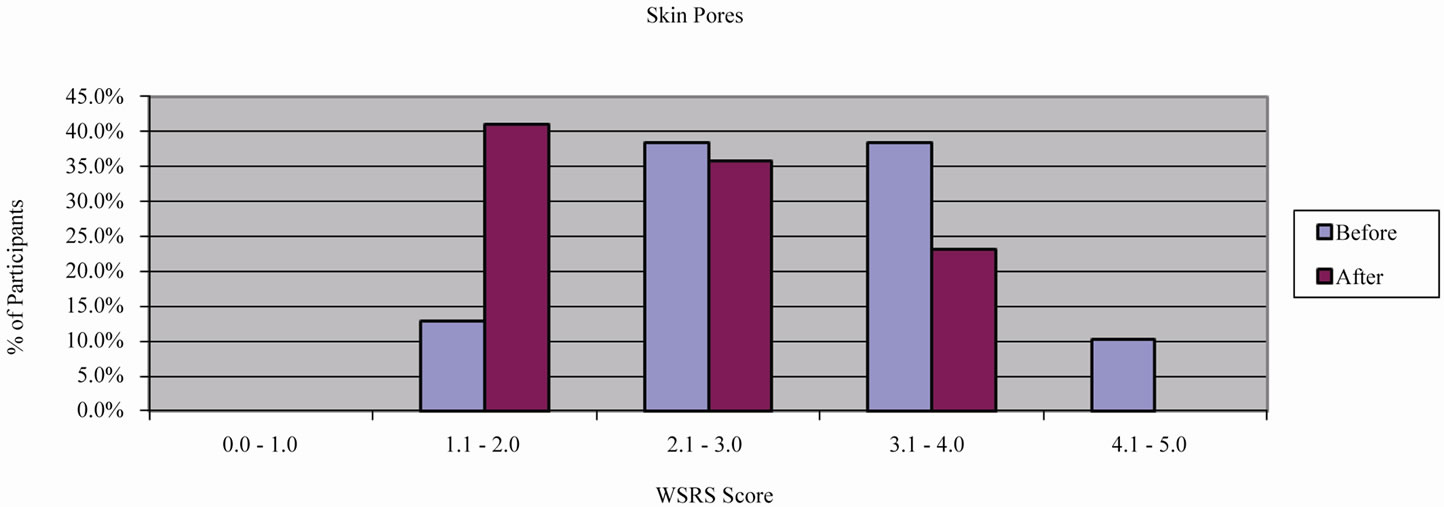
Figure 5. Investigator-graded WSRS score for skin pores.
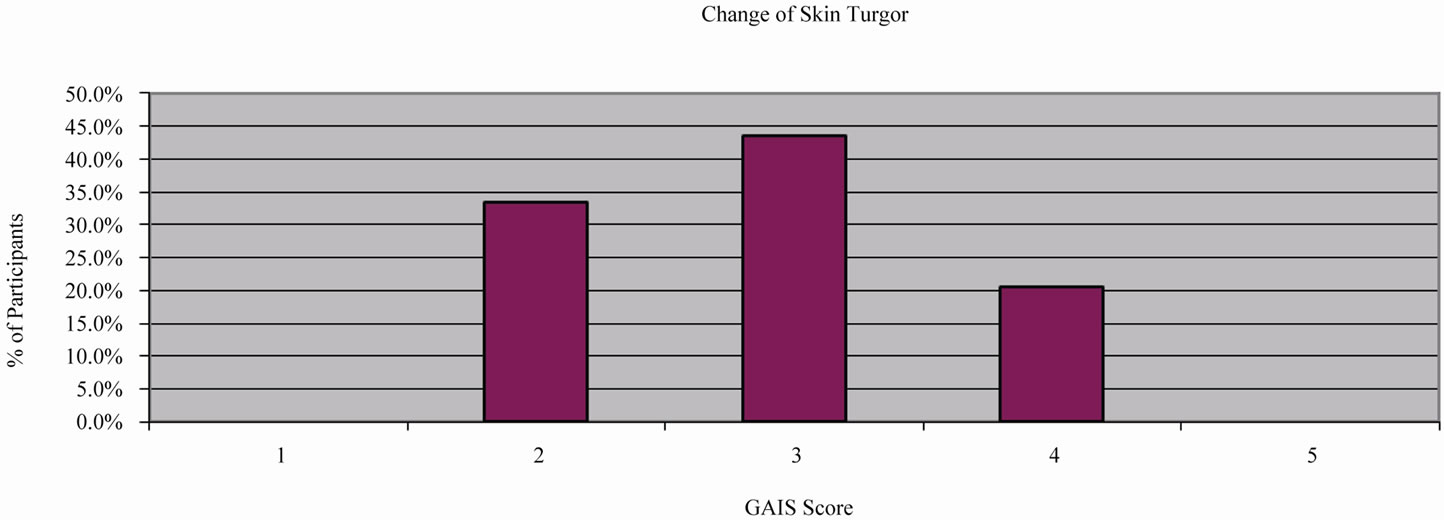
Figure 6. Investigator-graded GAIS score for skin turgor improvement.
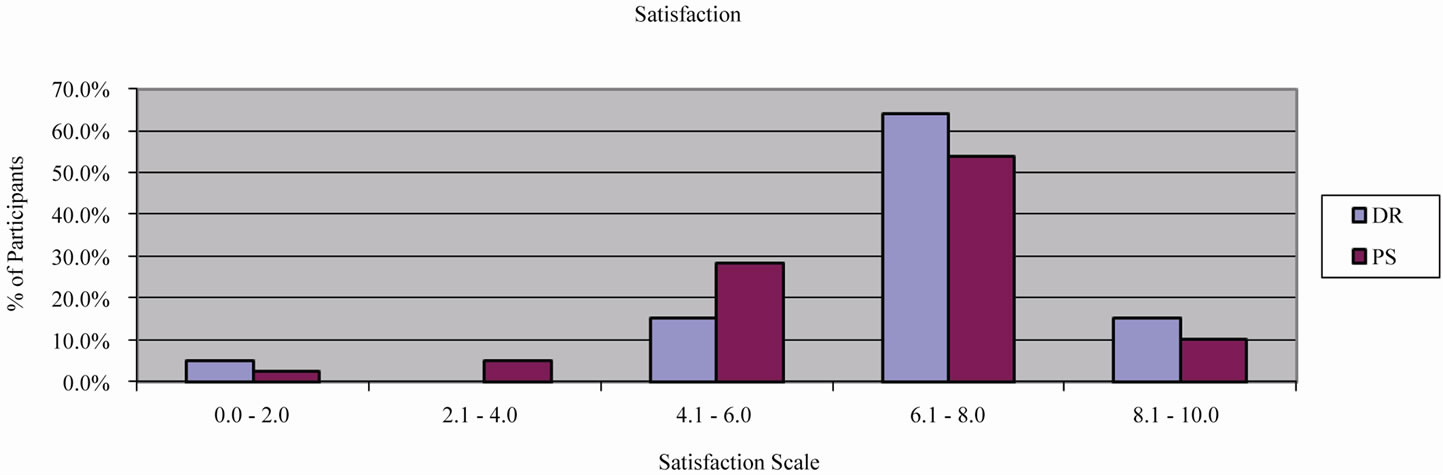
Figure 7. Satisfaction of participants and doctors with the treatment results.
An example of a visual skin modification after treatment is shown in Figure 8. The improvement in the appearance of fine wrinkles, skin micro-relief, pore size and skin turgor can be clearly seen.
The treatment had no side effects and was pain-free.
Some subjects demonstrated a short-termed erythema directly after the treatment
4. Discussion
This multicentric study has demonstrated the significant
 (a)
(a) (b)
(b)
Figure 8. Visual skin improvement: (a) before; (b) after treatment.
improvement of different visual skin appearances (such as wrinkles, skin pores and turgor) through multiple applications of dualfrequency US waves with frequencies of 3 and 10 MHz. Improvement of the skin turgor, reduction of pore size and wrinkles all point to the spatial rearrangement of the connective tissue structure, with an increase in its collagen and water content.
Intrinsic and extrinsic skin ageing are traditionally considered to be separate processes with different pathophysiological pathways and diverse visual appearances. However, these two processes share some important molecular features [4]. Both processes are cumulative and it appears that they follow similar pathways, including shifting of the balanced connective tissue towards its degradation through the short-termed or chronic activation of some MMPs. Each procedure that can temporarily reduce the activity of MMPs and/or increase the activity of HSPs in the skin should improve the collagen content and consequently, at least partly, restore the connective tissue balance. The treatment methods based on this pathophysiology are applied more and more in skin rejuvenation therapies (see e.g. [6,19]).
Because high-frequency US of 10 MHz as well as dual-frequency US waves can modulate the MMPs (unpublished) activity and significantly increase the rate of production of HSPs [11], these phenomenological results can indirectly support the new pathophysiological ideas of skin ageing, connecting this process with an increased concentration of MMPs and decreased activity of HSPs in the aged skin.
5. Conclusion
The present multicentre study has demonstrated that application of dual-frequency US waves and very high frequency US of 10 MHz significantly improves different visual appearances of ageing skin, which supports the hypothesis formulated in [12]. This safe non-invasive method yields results that are not as marked as those shown in the improvement of folds by injecting fillers (see e.g. [16], which has demonstrated the improvement of nasolabial folds by 1.1 to 1.7 WSRS grades), but can be used alternatively by subjects with a broad spectrum of visual skin ageing problems that they would like to have treated effectively and simultaneously.
REFERENCES
- P. K. Mays, J. E. Bishop and G. J. Laurent, “Age-Related Changes in the Proportion of Types I and III Collagen,” Mechanisms of Ageing and Development, Vol. 45, No. 3, 1988, pp. 203-212. doi:10.1016/0047-6374(88)90002-4
- C. Kut, W. Hornebeck, N. Groult, G. Redziniack, G. Godeau and B. Pellat, “Influence of Successive and Combined Ultraviolet A and B Irradiations on Matrix Metalloproteinases Produced by Human Dermal Fibroblasts IN Culture,” Cell Biology International, Vol. 21, No. 6, 1997, pp. 347-352. doi:10.1006/cbir.1997.0150
- S. R. Sandeman, R. G. A. Faragher, M. C. A. Allen, C. Liu and A. W. Lloyd, “Does MMP-2 Expression and Secretion Change with Increasing Serial Passage of Keratinocytes in Culture?” Mechanisms of Ageing and Development, Vol. 122, No. 2, 2001, pp. 157-167. doi:10.1016/S0047-6374(00)00227-X
- G. J. Fisher, S. Kang, J. Varani, Z. Bata-Csorgo, Y. Wan, S. Datta and J. J. Voorhees, “Mechanisms of Photoaging and Chronological Skin Aging,” Archives of Dermatology, Vol. 138, No. 11, 2002, pp. 1462-1470. doi:10.1001/archderm.138.11.1462
- M. Brennan, H. Bhatti, K. C. Nerusu, N. Bhagavathula, S. Kang, G. J. Fisher, J. Varani and J. J. Vorhees, “Matrix Metalloproteinase-1 Is the Major Collagenolytic Enzyme Responsible for Collagen Damage in UV-Irradiated Human Skin,” Photochemistry and Photobiology, Vol. 78, No. 1, 2003, pp. 43-48. doi:10.1562/0031-8655(2003)078<0043:MMITMC>2.0.CO;2
- J. Fonager, R. Beedholm, B. F. C. Clark and S. I. S. Rattan, “Mild Stress-Induced Stimulation of Heat Shock Protein Synthesis and Improved Functional Ability of Human Fibroblasts Undergoing Aging in Vitro,” Experimental Gerontology, Vol. 37, No. 10-11, 2002, pp. 1223- 1238.
- S. I. S. Rattan, “Hormetic Modulation of Aging and Longevity by Mild Heat Stress,” Dose-Response, Vol. 3, No. 4, 2005, pp. 533-546. doi:10.2203/dose-response.003.04.008
- S. K. Calderwood, A. Murshid and T. Prince, “The Shock of Aging: Molecular Chaperons and the Heat Shock Response in Longevity and Ageing—A Mini Review,” Gerontology, Vol. 55, No. 5, 2009, pp. 550-558. doi:10.1159/000225957
- A. E. Mayes and C. D. Holyoak, “Repeat Mild Heat Shock Increases Dermal Fibroblast Activity and Collagen Production,” Rejuvenation Research, Vol. 11, No. 2, 2008, pp. 461-465.
- S. D. Dams, M. de Liefde-van Beest, A. M. Nuijs, C. W. J. Oomens and F. P. T. Baaijens, “Heat Shocks Enhances Procollagen Type I and III Expression in Fibroblasts in ex Vivo Human Skin,” Skin Research and Technology, Vol. 17, No. 2, 2011, pp. 167-180. doi:10.1111/j.1600-0846.2010.00473.x
- W. Sontag and I. Kruglikov, “Expression of Heat Shock Proteins after Ultrasound Exposure in HL-60 Cells,” Ultrasound in Medicine & Biology, Vol. 35, No. 6, 2009, pp. 1032-1041. doi:10.1016/j.ultrasmedbio.2008.12.011
- I. Kruglikov and W. Sontag, “Ultrasound of 10 MHz Frequency as a Novel Strategy for Skin Anti-Aging Therapy,” Medical Hypotheses, Vol. 74, No. 3, 2010, pp. 620-621. doi:10.1016/j.mehy.2009.10.048
- I. Kruglikov and E. Kruglikova, “Dual Treatment Strategy by Venous Ulcers: Pilot Study to Dual-Frequency Ultrasound Application,” Journal of Cosmetics, Dermatological Sciences and Applications, Vol. 1, No. 4, 2011, pp. 157-163. doi:10.4236/jcdsa.2011.14024
- D. S. Downing and A. Weinstein, “Ultrasound Therapy of Subacromial Bursitis: A Double Blind Trial,” Physical Therapy, Vol. 66, No. 2, 1986, pp. 194-199.
- J. Eng, “Sample Size Estimation: How Many Individuals Should Be Studied?” Radiology, Vol. 227, No. 2, 2003, pp. 309-313. doi:10.1148/radiol.2272012051
- R. S. Narins, S. H. Dayan, F. S. Brandt and E. K. Baldwin, “Persistence and Improvement of Nasolabial Fold Correction with Nonanimal-Stabilized Hyaluronic Acid 100,000 Gel Particles/ml Filler on Two Retreatment Schedules: Results up to 18 Months on Two Retreatment Schedules,” Dermatology Surgery, Vol. 34, Suppl. 1, 2008, pp. 2-8. doi:10.1111/j.1524-4725.2008.34236.x
- D. Day, C. Littler, R. Swift and S. Gottlieb, “The Wrinkle Severity Rating Scale: A Validation Study,” American Journal of Clinical Dermatology, Vol. 5, No. 1, 2004, pp. 49-52. doi:10.2165/00128071-200405010-00007
- A. Di Pietro, D. M. Colombo and N. Giordan, “Facial Wrinkles Correlation and Skin Rejuvenation (Biostimulation) by Auto-Cross-Linked Hyaluronic Acid,” Journal of Plastic Dermatology, Vol. 3, No. 2, 2007, pp. 5-13.
- R. Kafi, H. S. R. Kwak, W. E. Schumacher, S. Cho, V. N. Hanft, T. A. Hamilton, A. L. King, J. D. Neal, J. Varani, G. J. Fischer, J. J. Voorhees and S. Kang, “Improvement of Naturally Aged Skin with Vitamin A (Retinol),” Archives of Dermatology, Vol. 143, No. 5, 2007, pp. 606- 612. doi:10.1001/archderm.143.5.606
NOTES
*Conflict of interest: Dr. I. Kruglikov is the managing partner of Wellcomet GmbH. He was involved in neither clinical treatments nor in the assessment of treatment results.